
Abstract
Single-shot fast spin-echo (SSFSE)-based magnetic resonance imaging (MRI) has been introduced as a technique with less distortion and fewer artifacts for diffusion tensor imaging (DTI). The purpose of this study was to compare mean diffusivity maps, fractional anisotropy (FA) maps, and three-dimensional white-matter tractography using data obtained with SSFSE diffusion-tensor MRI technique and the much more common DTI method, echo-planar imaging (EPI), in the brain using a 1.5-Tesla clinical MR imager. Thirty patients with neurological disorders were scanned with both SSFSE-DTI and EPI-DTI using comparable scan times. Mean diffusivity and FA maps were calculated from the SSFSE-DTI and EPI-DTI data and qualitatively compared using two criteria. Three-dimensional fiber tracking was also performed on each data set. SSFSE-DTI produced image artifacts less frequently than EPI-DTI. However, demonstration of three-dimensional fiber-tracking of white matter on SSFSE-DTI was inferior to that on EPI-DTI. In conclusion, SSFSE-DTI is a promising alternative to conventional EPI-DTI imaging, producing fewer image artifacts and geometric distortions. However, for 3D streamline fiber-tracking, EPI data produced more consistent and reliable results.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Diffusion tensor imaging (DTI) is now widely applied as a noninvasive MR technique for assessing brain development or pathological conditions. In addition, DTI data may also be used for three-dimensional reconstruction of complex white-matter tracts (tractography). The information on white-matter fibers is helpful for radiologists to comprehend the anatomical structures of white matter [1] and the relationship between white matter and surrounding lesions [2].
For DTI, the most commonly applied acquisition strategy is single-shot echo-planar imaging (SS-EPI), due to its rapid acquisition speed, insensitivity to motion artifacts, and high signal-to-noise ratio (SNR) efficiency (SNR per unit scan time), compared with multi-shot spin-echo or gradient-echo approaches. With SS-EPI, substantial susceptibility-induced anatomical distortions and/or signal drop-outs are usually visible surrounding bone, the sinuses, or metallic objects (i.e., aneurysm clips), even with the use of advanced distortion correction or parallel imaging techniques.
Another method for DTI, single-shot fast spin-echo (SSFSE)-based MR technique, has been introduced in some reports [3, 4]. The advantages of this technique over EPI diffusion-weighted imaging are reduced image distortions and signal drop-outs resulting from tissue susceptibility differences. Therefore, SSFSE may offer significant advantages for evaluating the cervical spine [5, 6], where large susceptibility and main magnetic field inhomogeneity-induced artifacts are commonly seen in SS-EPI data.
Although SSFSE suffers reduced SNR and increased blurring compared with SS-EPI, the effects on the processed mean diffusivity, FA, or reconstructed fiber tracts have not been investigated in comparison with EPI technique.
The purpose of this study was to compare mean diffusivity maps, fractional anisotropy (FA) maps, and three-dimensional white-matter tractography between the SSFSE diffusion-tensor MRI technique and the more common EPI method in the brain using a 1.5-Tesla clinical MR imager.
Methods
A total of 30 patients (20 men and 10 women, mean age 59.4 years) with neurological disease participated in this study. Informed consent was obtained from each patient. We obtained ethical approval from the institutional review board before the study. Pathological conditions of the patients included primary brain tumors [n = 10; malignant lymphoma (n = 6), glioblastoma (n = 2), astrocytoma (n = 2)], acute infarction (n = 14), intracranial hemorrhage (n = 4) and hypoxic encephalitis (n = 2). Diagnoses were made by brain biopsy (primary brain tumors) or by clinical history, presentation, and/or follow-up imaging studies. Hypoxic encephalitis was diagnosed in a patient with astrocytoma following neurosurgery.
All MR imaging was performed on a 1.5-Tesla MR imager (Signa Lx, GE Healthcare, Milwaukee, WI, USA) with a birdcage head coil. After conventional T2- and T1-weighted transverse scan, SSFSE-DTI and EPI-DTI were performed. Imaging parameters of SSFSE-DTI were as follows: TR/ TE = 20,000/73 ms, matrix 128 × 128, bandwidth = 32 kHz, FOV = 260 × 260 mm, slice thickness/gap = 5/0 mm, slice number = 30, and b value of 0 and 1,000 s/mm2 with the maximum b value applied in 13 directions. Imaging parameters of EPI-DTI were as follows: TR/ TE = 10,000/70 ms, bandwidth = 116 kHz with the maximum b value applied in 15 directions. FOV, spatial resolution, slice thickness, slice gap, slice number and b value of EPI-DTI were the same as SSFSE-DTI. Total scan time was 4 min and 43 s for SSFSE-DTI and 3 min for EPI-DTI. The parameters of SSFSE-DTI did not completely agree with those of EPI-DTI because of technical and clinical limitations.
All diffusion tensor images were transferred to an independent workstation. Calculated mean diffusivity maps and FA maps on gray-scaled and three-dimensional tract projections of two major white-matter fibers, including the cortico-spinal tracts and corpus callosum fibers, were obtained by using dTV 1.5 software (Image Computing and Analysis Laboratory, Tokyo, Japan.) [2].
For the three-dimensional reconstruction of white-matter fibers, we used the region-of-interest (ROI) approach [1, 2] and set the same fiber threshold for both data sets in each patient. The authors placed ROIs on the cerebral peduncle and internal capsule (Fig. 1a and b) on each side of axial images for cortico-spinal tracts and on the corpus callosum (Fig. 1c) at a midsagittal level on a reconstructed sagittal image for corpus callosum fibers. Fiber density ratio [7] was calculated as the number of the fibers passing through the ROI divided by the number of pixels in the ROI for each image. In patients with pathological conditions affecting the tractography, the ROIs were excluded from this estimation.

Transverse (a and b) and sagittal (c) SSFSE-DTI images obtained with a b value of 0 s/mm2 show ROIs used for the data analysis. ROIs were placed in the cerebral peduncle (a) and internal capsule (b) for 3D tractography of cortico-spinal tracts and in the corpus callosum (c) at a midsagittal level on reconstructed sagittal image for 3D tractography of corpus callosum fibers
SSFSE-DTI images were each compared with the corresponding EPI-DTI images using two qualitative criteria, conspicuousness of lesions (abnormal bright signals) and presence of distortion artifacts on mean diffusivity maps and gray-scaled diffusion tensor images.
The evaluation was performed by two experienced neuroradiologists as follows. Conspicuousness of lesions and image distortion artifact were graded as 1 = SSFSE-DTI definitely inferior to EPI-DTI, 2 = SSFSE-DTI slightly inferior to EPI-DTI, 3 = SSFSE-DTI comparable with EPI-DTI, 4 = SSFSE-DTI slightly superior to EPI-DTI, 5 = SSFSE-DTI definitely superior to EPI-DTI. Demonstration of major white-matter fibers was also graded on a 5-point scale: 1 = no demonstration of major white-matter fibers, 2 = some short fibers were visualized along the major white-matter fibers, 3 = major white-matter fibers were identified but not completely, 4 = major white-matter fibers were visualized with some extra fibers, 5 = major white-matter fibers were clearly visualized without extra fibers. They made their evaluations based on anatomical knowledge and existing literature [1].
No quantitative evaluation was done in this study for two reasons. First, imaging-pathologic correlation was too difficult for cerebral white matter and pathologic conditions. Second, image quantization characteristics, such as volume of white-matter fibers, were expected to be unreliable because these values depend on algorithm parameters of the software, which are sensitive to arbitrary distinctions.
Results
In all patients, both SSFSE-DTI and EPI-DTI were effective in demonstrating gray-scaled DTI and white-matter fiber-tracking.
Mean scale for conspicuousness of lesions on diffusion tensor images was 2.62 ± 1.12 (neuroradiologist 1) and 2.53 ± 0.64 (neuroradiologist 2).
Mean scale for distortion artifacts was 3.81 ± 1.14 (neuroradiologist 1) and 3.67 ± 0.62 (neuroradiologist 2). In particular, SSFSE-DTI was the preferred method in patients who had undergone some neurosurgical procedures and had lesions in the brain stem and posterior fossa because there were fewer artifacts and less distortion in the images (Figs. 2 and 3).

A 29-year-old woman with suspected hypoxic encephalopathy after suicide. She had a history of neurosurgical operation for astrocytoma, 5 years before. Three-plane (axial, coronal and sagittal plane) of SSFSE-DTI (TR/TE/excitations: 20,000 ms/73 ms/1) images (a) demonstrate fewer artifacts and distortions due to susceptibility effects, compared with those of EPI-DTI (TR/TE/excitations: 10,000 ms/70 ms/1) (b) (arrows). Partial defect of the right temporal lobe (open arrow) and presence of multiple hyperintense changes in white matter are shown

A 72-year-old man with acute infarction in the brain stem. Three-plane (axial, coronal and sagittal plane) isotropic diffusion-weighted images and white matter fibers of cortico-spinal tract derived from the SSFSE-DTI (TR/TE/excitations: 20,000 ms/73 ms/1) data (a) and EPI-DTI (TR/TE/excitations: 10,000 ms/70 ms/1) data (b). Both axial images show a small hyperintense lesion in the pons, suggesting acute infarction. EPI-based images (b) show more artifacts (arrows) and spatial distortions (arrowhead) compared with SSFSE-based images (a)
Mean fiber density ratios for cortico-spinal tracts and corpus callosum were 0.40 ± 0.15 and 0.92 ± 0.07 on EPI-DTI and 0.06 ± 1.13 and 0.96 ± 1.34 on SSFSE-DTI, respectively. As shown in Figs. 3 and 4, there were fewer visible white-matter tract fibers in the SSFSE-DTI compared with EPI-DTI (Fig. 4).

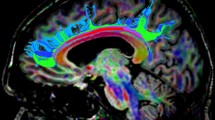
A 37-year-old man with multiple infarctions after neurosurgical operation for Moya-moya disease. Demonstration of white-matter fibers of cortico-spinal tract on SSFSE-DTI (a) three-dimensional fiber-tracking is inferior to that on EPI-DTI (b) in oblique-sagittal view
Discussion
Diffusion tensor imaging has become more important as a tool not only for research but also for clinical use for neuro-imaging. EPI has long been the conventional approach for acquiring DTI data, however, this method is susceptible to geometric distortions and signal drop-outs. FA maps or three-dimensional tractography from EPI-DTI data may not reflect the accurate pathological or anatomical conditions of the brain. Therefore, there have been some reports of methods or technical developments to avoid the artifacts and distortions in EPI-DTI images, including parallel imaging technique or other refined imaging methods. Here we have investigated an alternative acquisition strategy, SSFSE, which is less susceptible to these effects.
SSFSE-DTI proved advantageous to avoid susceptibility artifacts compared with EPI-DTI. This result was as expected and SSFSE-DTI proved to be the preferred method when image distortions and/or artifacts due to magnetic homogeneity (i.e., after neurosurgical procedures or for lesions near bone or air components) are predicted before MR examinations.
We hypothesized that reconstructed fiber tracts would be comparable for the two acquisition strategies. However, as shown in Fig. 4, results derived from the SSFSE data were inferior to those of the SS-EPI data. Reasons for this poor performance are likely related to the intrinsically lower SNR and increased blurring present in the SSFSE data, as noted in previous studies. This may be partially addressed through the use of custom multi-channel RF coils (as shown by Xu et al. [8]). The effect of blurring, however, is more difficult to correct and, as it affects adjacent and neighboring voxels, results in errors in the calculated principle diffusion direction. The combination of higher-field magnet (3T) and SSFSE-DTI may improve results because of increased signal-to-noise ratio. Moreover, SS-EPI would suffer more severe artifacts on 3T MR imager due to B0 field inhomogeneity.
The limitations of our study included the small numbers of patients and their heterogeneous pathologies. Further investigation is needed before the SSFSE-DTI can become a useful tool in evaluation of the brain. Quantitative assessment and sequence optimization are desirable in particular.
Another limitation is the MR imaging sequence. Some more advanced MR imaging techniques, such as EPI with parallel imaging, non-CPMG SSFSE-DTI and PROPELLER-DTI [9, 10], have been proposed to acquire diffusion tensor images with higher image quality. Comparison between these methods may lead to different solutions to the problem, including alternative methods of non-EPI sequencing.
Conclusion
In conclusion, SSFSE-DTI is a promising method for obtaining fewer artifacts and less distortion, compared with EPI-DTI in some clinical cases. This sequence is useful in particular for the patients with image distortions or susceptibility artifacts, including after neurosurgical procedure. However, SSFSE did not provide high quality tractography results.
References
Wakana S, Jiang H, Nagae-Poetscher LM, van Zijl PC, Mori S (2004) Fiber tract-based atlas of human white matter anatomy. Radiology 230:77–87
Kunimatsu A, Aoki S, Masutani Y, Abe O, Mori H, Ohtomo K (2003) Three-dimensional white matter tractography by diffusion tensor imaging in ischaemic stroke involving the corticospinal tract. Neuroradiology 45:532–535
Bastin ME, Le Roux P (2002) On the application of a non-CPMG single-shot fast spin-echo sequence to diffusion tensor MRI of the human brain. Magn Reson Med 48:6–14
Lovblad KO, Jakob PM, Chen Q et al (1998) Turbo spin-echo diffusion-weighted MR of ischemic stroke. AJNR Am J Neuroradiol 19:201–208
Fujikawa A, Tsuchiya K, Koppera P, Aoki C, Hachiya J (2003) Case report: spinal cord infarction demonstrated on diffusion-weighted MR imaging with a single-shot fast spin-echo sequence. J Comput Assist Tomogr 27:415–419
Tsuchiya K, Katase S, Fujikawa A, Hachiya J, Kanazawa H, Yodo K (2003) Diffusion-weighted MRI of the cervical spinal cord using a single-shot fast spin-echo technique: findings in normal subjects and in myelomalacia. Neuroradiology 45:90–94
Roberts TP, Liu F, Kassner A, Mori S, Guha A (2005) Fiber density index correlates with reduced fractional anisotropy in white matter of patients with glioblastoma. AJNR Am J Neuroradiol 26:2183–2186
Xu D, Henry RG, Mukherjee P et al (2004) Single-shot fast spin-echo diffusion tensor imaging of the brain and spine with head and phased array coils at 1.5 T and 3.0 T. Magn Reson Imaging 22:751–759
Cheryauka AB, Lee JN, Samsonov AA, Defrise M, Gullberg GT (2004) MRI diffusion tensor reconstruction with PROPELLER data acquisition. Magn Reson Imaging 22:139–148
Wang FN, Huang TY, Lin FH et al (2005) PROPELLER EPI: an MRI technique suitable for diffusion tensor imaging at high field strength with reduced geometric distortions. Magn Reson Med 54:1232–1240
Acknowledgements
We thank Masaya Hirano and Hiroyuki Kabasawa, GE Yokogawa Medical Systems, for technical assistance and advice.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hori, M., Ishigame, K., Shiraga, N. et al. Mean diffusivity, fractional anisotropy maps, and three-dimensional white-matter tractography by diffusion tensor imaging. Comparison between single-shot fast spin-echo and single-shot echo-planar sequences at 1.5 Tesla. Eur Radiol 18, 830–834 (2008). https://doi.org/10.1007/s00330-007-0805-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-007-0805-9