
Abstract
The BLADE and PROPELLER (periodically rotated overlapping parallel lines with enhanced reconstruction) techniques have been proposed to reduce the effect of head motion. Preliminary results have shown that BLADE also reduces pulsation artifacts from venous sinuses. The purpose of this study was to compare T1-weighted FLAIR acquired with BLADE (T1W-FLAIR BLADE) and T1-weighted spin-echo (T1W-SE) for the detection of contrast enhancement in a phantom and in patients with suspected brain lesions and to compare the degree of flow-related artifacts in the patients. A phantom filled with diluted Gd-DTPA was scanned in addition to 27 patients. In the phantom study, the peak contrast-to-noise ratio of T1W-FLAIR BLADE was larger than that of T1W-SE, and the position of the peak was shifted to a lower concentration. In patients, the degree of flow-related artifacts was significantly higher in T1W-SE. Among the 27 patients, 9 had metastatic tumor, and 18 did not. On a patient-by-patient basis, the sensitivity and specificity for the detection of metastatic lesions on axial T1W-SE were 100% and 55.6% respectively, while on axial T1W-FLAIR BLADE they were 100% and 100%. T1W-FLAIR BLADE seems to be capable of replacing T1W-SE, at least for axial post-contrast imaging to detect brain metastases.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Contrast-enhanced magnetic resonance imaging (MRI) of the brain is acquired in various disorders such as tumor, inflammation, vascular disease and so on. For example, typically two-dimensional conventional spin-echo images in the axial, coronal and/or sagittal orientation are employed for the detection of metastatic tumors in the brain [1, 2]. Flow-related artifacts are sometimes prominent, especially in the posterior cranial fossa, and these mimic the contrast-enhanced lesions or prevent the detection of contrast-enhanced lesions. To overcome this problem, contrast-enhanced imaging with a three-dimensional MP-RAGE sequence can be used; however, some lesions do not show sufficient contrast enhancement in comparison with a conventional spin-echo sequence [1, 2]. The BLADE and PROPELLER (periodically rotated overlapping parallel lines with enhanced reconstruction) techniques were proposed to reduce the effect of head motion in translation and rotation [3, 4]. Unlike rectilinear k-space sampling, this method acquires multiple echo trains with a turbo spin-echo (TSE) sequence in a rotating (with respect to rectilinear k-space), partially overlapping fashion, so-called “blades” [5].
Preliminary clinical results have shown that BLADE acquisition reduces pulsation artifacts from the transverse and sigmoid sinuses on non-contrast-enhanced T1-weighted fluid-attenuated inversion recovery (FLAIR) and T2-weighted FLAIR, even without motion correction [5].
The purpose of this study was to compare T1-weighted FLAIR images with BLADE (T1W-FLAIR BLADE) and conventional T1-weighted spin-echo (T1W-SE) images for the detection of contrast enhancement in a Gd phantom and in patients with suspected brain metastasis and to compare the degree of flow-related artifacts in the patients.
Materials and methods
This study consisted of two subparts and one main part. The first of the two subparts was the phantom study to evaluate the contrast features of T1W-SE and T1W-FLAIR BLADE. The second of the subparts employed two patients for the comparison of T1W-FLAIR (Cartesian k trajectory) and T1W-FLAIR BLADE. The main part of this study was to compare contrast-enhanced axial T1W-SE and contrast-enhanced axial T1W-FLAIR BLADE in an additional 27 patients.
Phantom study
Firstly, to confirm that there was no paradoxical enhancement (Gd-DTPA-related signal decrease) in T1W-FLAIR and to compare the Gd-DTPA sensitivity of T1W-SE to that of T1W-FLAIR, a diluted-Gd line phantom was scanned. The phantom was built from multiple 2.5-ml syringes filled with diluted Gd-DTPA-BMA. The Gd-DTPA-BMA was diluted with saline to Gd-DTPA concentrations of 2−n, where n = 0, 1, 2, ..., 24. The contrast-to-noise ratios (CNRs), for the contrast between each Gd-DTPA concentration and saline were plotted for both sequences.
Comparison between T1W-FLAIR (Cartesian k trajectory) and T1W-FLAIR BLADE
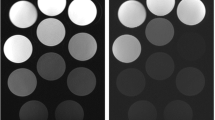
Before starting the main part of this study with 27 patients, contrast-enhanced T1W-SE, T1W-FLAIR BLADE and T1W-FLAIR with a conventional Cartesian k-space trajectory were obtained in two separate patients. Conventional T1W-FLAIR showed prominent flow-related artifacts (Fig. 1); thus, this sequence was not used in additional comparisons.

A 41-year-old man with lung cancer. No metastatic lesion was detected. (a) T1W-FLAIR BLADE, (b) T1W SE, (c) T1W-FLAIR with Cartesian trajectory. Prominent flow-related artifacts are seen on (b) and (c)
Main part of this study
Finally, 27 patients (16 men and 11 women, mean age 69.3±11.3 years old) with known or suspected metastatic brain lesions were included in this study. Among the 27 patients, 25 had lung cancer (14 adenocarcinoma, 6 squamous cell carcinoma, 3 small-cell lung cancer, 1 adenosquamous cell carcinoma, and 1 neuroendocrine carcinoma), 1 had colon cancer, and 1 had breast cancer.
In this patient study, before the administration of Gd-DTPA-BMA (0.1 mmol/kg, Omniscan, Daiichi pharmaceutical Co. Ltd., Osaka, Japan), axial T1W-SE and axial T2W-turbo-SE images were acquired. After the administration of Gd-DTPA-BMA, axial T1W-FLAIR BLADE and T1W-SE were acquired, followed by coronal T1W-SE. The scans were initiated 4 min after intravenous administration of Gd-DTPA-BMA in a single dose. It has been reported that the contrast-to-noise ratio between gray matter and tumor with blood-brain barrier damage did not change significantly from 3.5 min after Gd-DTPA injection until 25 min after [6]. Furthermore, the order of the axial scans was balanced among the patients. Among the 27 patients, T1W-FLAIR BLADE was acquired first in 14 patients, and T1W-SE was acquired first in the other 13 patients. In the non-BLADE axial and coronal images, the phase-encoding direction was set right-to-left. The comparison between post-contrast T1W-SE and T1W-FLAIR BLADE was made only for the axial images. This study was approved by the medical ethics committee of the hospital, and all subjects provided written informed consent.
MR imaging
All phantom and patient scans were performed on a 1.5-T MR scanner using a 12-channel phased-array head coil (Avanto, Siemens Medical Solutions, Erlangen, Germany). The scan parameters for T1W-SE were repetition time (TR)/echo time (TE): 551/14, 192×256 matrix, two signal averages, bandwidth of 100 Hz/pixel and flip angle of 80 degrees; while those for T1W-FLAIR BLADE were TR/TE/TI 1,800/57/860, echo-train length (ETL) of 19, echo spacing of 5.74 ms, 35 blades with 161.9% k-space coverage, 256-square matrix, refocusing flip angle of 150 degrees, bandwidth of 362 Hz/pixel and the same slice thickness (6 mm with 1.2-mm gap) and field of view (20 cm) as T1W-SE. The scan time was 3.5 min for both T1W-SE and T1W-FLAIR BLADE, and parallel imaging techniques were not applied to either scan. For T1W-FLAIR BLADE, no correction for translational and rotational movement was applied. Since the motion correction option requires the ETL to be larger than 29 on the current system, it would result in a longer TE like 80 ms. Such a long echo time would result in decreased T1 contrast and decreased sensitivity to Gd-DTPA enhancement.
Standard of reference in the patient study
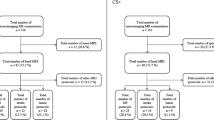
A standard of reference was established by two neuro-radiologists who reviewed all MR imaging series including pre-contrast axial T1W-SE and T2W-turbo-SE, post-contrast axial and coronal T1W-SE, and axial T1-FLAIR-BLADE images, as well as clinical records and, when available, follow-up MR examinations. There was no discrepancy between the two neuro-radiologists in the process of establishing a standard of reference. For the presence of metastatic lesions, results were determined patient-by-patient as positive or negative. Among the 27 patients, 9 had one or more metastatic tumors (positive), and 18 had no tumor (negative). The total number of lesions was 55. Pathological proof was obtained in one patient with metastatic adenocarcinoma that had originated in the colon. The other eight positive patients received radiation therapy and/or chemotherapy. Among these eight patients with metastatic tumors, two died within 3 months, while six had a follow-up MR examination 3–4 months later. Among the 18 patients without metastatic brain tumors, 10 had a follow-up MR examination 3–4 months later to confirm the absence of metastatic brain tumors. The remaining eight patients did not show any clinical sign for the development of brain metastases even after 3–4 months. These medical records were also utilized to establish a standard of reference.
Evaluation of the degree of flow artifacts in 27 patients
The degree of flow-related artifacts was scored subjectively as 0, 1, 2 or 3, corresponding to none, slight, moderate or severe, by one of the neuro-radiologists who participated in the set-up process of the standard of reference. The scores of two sequences were compared using the Wilcoxon signed-ranks test.
Detection of metastatic lesions in axial images
This comparison included the 27 patients described above with known or suspected metastatic brain lesions.
Qualitative analysis
The presence or absence of metastatic tumor was recorded by two neuroradiologists who had not participated in the set-up process of the standard of reference. They independently reviewed the images on a DICOM viewer without access to clinical information. In the first reading session, either post-contrast T1W-SE or T1W-FLAIR BLADE was reviewed. To avoid recall bias, the other scan was reviewed after 2 weeks. The location and number of lesions were recorded and divided between the supratentorial cranial region and the infratentorial cranial region. If there were discrepancies between the two readers, consensus was obtained by discussion after both reading sessions were completed.
Quantitative analysis
The CNRs of lesions with a diameter of 6 mm or larger, detected on both T1W-SE and T1W-FLAIR BLADE were measured and compared using a Student’s t-test. Lesions with overlapping flow artifacts were excluded. The region of interest for each lesion was drawn as large as possible while excluding the non-enhancing central area of the lesion. A noise region of interest was drawn in artifact-free air space. Each contrast-to-noise ratio was calculated as the signal intensity of the lesion minus the signal intensity of corresponding normal brain parenchyma in the contralateral hemisphere, divided by the standard deviation in the noise region of interest. This measurement was performed by one of the two neuroradiologists who participated in the standard-of-reference set-up process.
Results
Phantom study
The CNR of the diluted-Gd-DTPA phantom lines were plotted (Fig. 2). The peak CNR (or enhancement) of T1W-FLAIR BLADE was larger and was shifted to a lower concentration compared to that of T1W-SE. However, the CNR at high concentrations of Gd-DTPA was smaller for T1W-FLAIR BLADE than for T1W-SE. No paradoxical enhancement was seen on T1W-FLAIR BLADE images.

CNR plots of diluted Gd-DTPA phantom lines. The peak height of CNR is higher for T1W-FLAIR BLADE than for T1W-SE, where as the Gd-DTPA concentration for the peak is smaller for T1W-FLAIR than for T1W-SE
Evaluation of the degree of flow artifacts in 27 patients
In patients, the degree of flow-related artifacts was significantly lower for T1W-FLAIR BLADE than for T1W-SE. In all patients, T1W-FLAIR BLADE had a score of 0; however, T1W-SE had a score of 3 in 21 patients, and a score of 2 in the other 6 patients (p<0.01).
Detection of metastatic lesions in axial images (Fig. 3)
Qualitative analysis
For qualitative analysis, see Fig. 3.

A 76-year-old man with small cell lung cancer. Flow-related artifact is less prominent on T1W-FLAIR BLADE (a) than on T1W-SE (b). Two additional metastatic lesions can be detected on (a, arrows). These lesions were also visualized on coronal T1W-SE (arrows, c)
In a patient-by-patient analysis, T1W-SE showed seven false-positive cases and no false-negative cases, giving a sensitivity of 100% and a specificity of 55.6%. T1W-FLAIR BLADE had a sensitivity of 100% and a specificity of 100%.
T1W-SE showed 13 false-positive lesions and 4 false-negative lesions. Four false-positive lesions were found in the supratentorial cranial region, and the other nine were found in the infratentorial cranial region. All four false-negative lesions were located in the infratentorial region. These false-positive and -negative lesions were thought to be due to flow artifacts on T1W-SE. T1W-FLAIR BLADE showed no false-positive lesions and one false-negative lesion. This false-negative lesion was very small, on the order of 2 mm.
Discrepancies between the two reviewers appeared with regard to the three false-positive lesions. The shapes of the lesions and the presence of ghosts aligned with the phase-encoding direction of the T1W-SE images were discussed, and then consensus was obtained.
Quantitative analysis
Sixteen out of the 55 lesions were included in this analysis, and within these 16, the scan order of T1W-SE and T1W-FLAIR BLADE was balanced. For the contrast between enhanced lesion and brain parenchyma, the mean CNR on T1W-SE was 48.9±37.2 and that on T1W-FLAIR BLADE was 44.5±21.3 (p=0.73).
Disucussion
Propeller and BLADE sequences reduce gross motion artifacts, such as those due to translation and rotation of the head, with motion correction [3, 7]. In the present study, we showed that flow-related artifacts after Gd-DTPA administration can also be reduced, even without motion correction. T1W-FLAIR with a conventional Cartesian trajectory in k-space showed prominent flow-related artifacts. Thus, the reduction of flow-related artifacts on T1W-FLAIR BLADE was due mainly to the BLADE k-space trajectory. As a result of the BLADE trajectory, flow-related artifacts were expected to be scattered widely around the entire field of view, and thus to be less prominent. Flow artifacts on T1W-SE and T1W-FLAIR with a conventional Cartesian trajectory are prominent because the artifacts align and superpose along the phase-encoding direction.
The k-space trajectory used in BLADE requires a pulse sequence such as turbo spin echo or turbo gradient spin echo that is capable of covering multiple k-space lines per excitation [3, 8]. Typically, an echo train length of 15–30 is employed, resulting in an elongation of the effective echo time. To obtain T1-weighted contrast, a pre-inversion pulse is necessary to compensate for the elongation of the echo time.
As shown in the phantom study, T1W-FLAIR BLADE was more sensitive to lower concentrations of Gd-DTPA than T1W-SE, probably due to the presence of the pre-inversion pulse; while T1W-SE was more sensitive to higher concentration of Gd-DTPA than T1W-FLAIR-BLADE, probably due to the shorter echo time of T1W-SE. It has been reported that the three-dimensional MP-RAGE sequence is less sensitive to faint contrast enhancement than a two-dimensional conventional spin-echo sequence [9]. Thus, T1W-FLAIR BLADE should be more sensitive than MP-RAGE in the detection of faint contrast enhancement.
In the clinical setting, it is necessary to confirm that faint contrast enhancements, such as those due to small multiple-sclerosis plaques or low-grade gliomas, can be visualized more clearly in T1W-FLAIR BLADE than in T1W-SE. On the other hand, it is also necessary to confirm that T1W-FLAIR BLADE can readily visualize strongly enhancing lesions such as meningiomas, high-grade gliomas, hemangiopericytomas, and so on, before replacing T1W-SE as the sequence of choice for standard post-contrast images. Two limitations of this study were the lack of pathological proof in most of the patients and the lack of concrete confirmation of the presence or absence of metastatic lesions, although medical records of clinical follow-up or MR imaging data obtained 3–4 months later were available and reviewed in most cases. Another limitation was that lesion detection was analyzed only for axial images. In the clinical setting, the detection of metastatic lesions is performed using not only axial images, but also coronal and/or sagittal images. If we had referred to all three orientations, we expect that the specificity of T1W-SE would have been higher than that found in the present study for axial T1W-SE alone.
The results of the present study are predicated on a slice thickness of 6 mm, a single dose of Gd-DTPA, and a main field of 1.5 T. It is necessary to perform the same kind of study to confirm whether the replacement of T1W SE by T1W-FLAIR BLADE is also feasible for different scan conditions such as thinner slices, smaller or larger doses of contrast material, the application of magnetization transfer contrast pulse, and a magnetic field of 3 T. Flow-related artifacts might depend on any of these three parameters [10]. However, T1W-FLAIR BLADE seems to be able to replace T1W-SE for the detection of metastatic lesions at 1.5 T with a 6-mm slice thickness and a single dose of contrast medium.
Conclusions
T1W-FLAIR BLADE is less susceptible to flow-related artifacts than T1W-SE. T1W-FLAIR BLADE seems to be able to replace T1W-SE, at least as the post-contrast imaging sequence used to detect brain metastasis in the axial orientation at 1.5 T.
References
Wenz F, Hess T, Knopp MV, Weisser G, Bluml S, Schad LR, Hawighorst H, van Kaick G (1994) 3D MPRAGE evaluation of lesions in the posterior cranial fossa. Magn Reson Imaging 12(4):553–558
Wetzel SG, Johnson G, Tan AG, Cha S, Knopp EA, Lee VS, Thomasson D, Rofsky NM (2002) Three-dimensional, T1-weighted gradient-echo imaging of the brain with a volumetric interpolated examination. AJNR Am J Neuroradiol 23(6):995–1002
Pipe JG (1999) Motion correction with PROPELLER MRI: application to head motion and free-breathing cardiac imaging. Magn Reson Med 42(5):963–969
Forbes KP, Pipe JG, Karis JP, Farthing V, Heiserman JE (2003) Brain imaging in the unsedated pediatric patient: comparison of periodically rotated overlapping parallel lines with enhanced reconstruction and single-shot fast spin-echo sequences. AJNR Am J Neuroradiol 24(5):794–798
Wintersperger BJ, Runge VM, Biswas J, Nelson CB, Stemmer A, Simonetta AB, Reiser MF, Naul LG, Schoenberg SO (2006) Brain magnetic resonance imaging at 3 Tesla using BLADE compared with standard rectilinear data sampling. Invest Radiol 41(7):586–592
Akeson P, Nordstrom CH, Holtas S (1997) Time-dependency in brain lesion enhancement with gadodiamide injection. Acta Radiol 38(1):19–24
Forbes KP, Pipe JG, Bird CR, Heiserman JE (2001) PROPELLER MRI: clinical testing of a novel technique for quantification and compensation of head motion. J Magn Reson Imaging 14(3):215–222
Pipe JG, Zwart N (2006) Turboprop: improved PROPELLER imaging. Magn Reson Med 55(2):380–385
Mugler JP 3rd, Brookeman JR (1991) Rapid three-dimensional T1-weighted MR imaging with the MP-RAGE sequence. J Magn Reson Imaging 1(5):561–567
Naganawa S, Koshikawa T, Nakamura T, Kawai H, Fukatsu H, Ishigaki T, Komada T, Maruyama K, Takizawa O (2004) Comparison of flow artifacts between 2D-FLAIR and 3D-FLAIR sequences at 3 T. Eur Radiol 14(10):1901–1908
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Naganawa, S., Satake, H., Iwano, S. et al. Contrast-enhanced MR imaging of the brain using T1-weighted FLAIR with BLADE compared with a conventional spin-echo sequence. Eur Radiol 18, 337–342 (2008). https://doi.org/10.1007/s00330-007-0741-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-007-0741-8