
Abstract
The aim of this study was the evaluation of the diagnostic usefulness of ductal or segmental enhancement in dynamic breast MRI. Segmental and ductal enhancement have been established as the breast MRI hallmarks of intraductal breast cancer (DCIS); however, the positive predictive value of this imaging finding is still unknown. In our study, we analysed the overall prevalence of a segmental or a linear enhancement pattern on breast MRI for an unselected cohort of patients. The aim was to evaluate the diagnostic usefulness of segmental or linear enhancement. Second, we asked whether biopsy was necessary also in the absence of mammographic findings suggestive of DCIS. Prospective, consecutive evaluation of 1,003 patients undergoing bilateral dynamic breast MRI. Studies were interpreted by two experienced breast radiologists. A diagnostic or screening two-view mammogram was available for all patients. Biopsy or short-term breast MRI follow-up was recommended for patients showing a segmental or a linear enhancement pattern on breast MRI. The patients’ final diagnoses were established by imaging guided excisional or core biopsy or by clinical plus conventional imaging follow-up for a period of 2 years. The prevalence of segmental or linear enhancement was determined for patients with a final diagnosis of benign breast disease compared with those with a diagnosis of breast cancer. One hundred twenty patients had invasive breast cancer, 24 patients had DCIS and 859 patients had unsuspicious breast MRI or benign breast disease. A segmental or a linear enhancement pattern was found for 50/1,003 (5%) patients (17 DCIS, 33 benign breast diseases). Accordingly, the positive predictive value of segmental and linear enhancement is 34% (17/50); the specificity of this criterion is 96% (826/859). For 4/24 (17%) patients, DCIS was visible as segmental or linear enhancement on dynamic breast MRI, whereas no abnormalities were visible on the corresponding mammogram. The overall prevalence of a ductal or a segmental enhancement pattern on breast MRI is low. But this finding has a high specificity and a moderate positive predictive value for intraductal neoplastic changes. We conclude that if segmental or linear enhancement is identified on breast MRI further work-up is necessary. We recommend either direct MR-guided vacuum-assisted core biopsy or short-term follow-up breast MRI within 3 months. If ductal enhancement then persists, MR-guided biopsy should be recommended even in the absence of mammographically visible signs of DCIS
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In addition to conventional imaging methods, breast MRI is increasingly used for further work-up of breast diseases [1–3]. MRI has been shown to be highly specific in the differentiation of fibrosis versus tumor recurrence [4] after breast-conserving therapy. Breast MRI is recommended as an additional imaging method for patients scheduled for breast-conserving therapy in order to rule out multicentric or contralateral breast tumors [5–8]. Recently, the value of breast MRI in screening high-risk patients has been pointed out [9].
The role of breast MRI in the diagnosis of intraductal breast cancer (DCIS) is still the subject of controversial discussion. Reported sensitivities for the identification of DCIS on breast MRI range from 40 to 100% [10–15].
Dynamic enhancement rates of DCIS are extremely variable [16], but morphological criteria such as segmental or linear enhancement have been reported to be the imaging hallmarks of DCIS on breast MRI [15, 17–23]. However, the positive predictive value of this enhancement pattern is still unknown. To investigate the diagnostic usefulness of this criterion, we analyzed the prevalence of a segmental and a linear enhancement pattern on breast MRI in an unselected patient cohort. The aim was to find out how specific this enhancement pattern is and whether biopsy should be recommended even in the absence of mammographic findings suggestive of DCIS.
Materials and methods
Study design and inclusion criteria
The prospective study was done on 1,003 consecutive patients (mean age 51 years) who underwent breast MRI from 1999 through 2000 for various indications: inconclusive clinical and conventional imaging findings (group A, 326 patients), preoperative staging of patients with suspected DCIS or invasive breast cancer (group B, 81 patients), follow-up after breast cancer (group C, 387 patients) and screening of patients with familial risk for breast cancer (group D, 209 patients).
The study design was approved by the author’s institutional review board; all patients gave informed consent to be examined after the nature of the procedure had been fully explained to them.
Data validation of segmental and linear enhancement on breast MRI
A two-view mammogram was available for all 50 patients who had a segmental or a linear enhancement pattern on breast MRI.
For patients whose mammogram showed microcalcifications indicative of DCIS, we recommended immediate breast biopsy (13/17 patients with DCIS and segmental or linear enhancement on breast MRI). For the remaining (37/50) patients for whom breast MRI showed a segmental or a linear enhancement pattern but who had a normal mammogram, we first performed targeted breast ultrasonography. If the lesion was visible on breast MRI only, we offered the patient either immediate MR-guided breast biopsy or short-term follow-up breast MRI within 3 months. For those patients who had decided to have short-term follow-up with breast MRI, we performed regular follow-up with clinical examination and conventional imaging if segmental or linear enhancement disappeared on the short-term follow-up breast MRI. If segmental or linear enhancement persisted on the short-term follow-up breast MRI, we recommended MR-guided breast biopsy.
In the end, the patients’ final diagnoses were established by imaging-guided excisional or core biopsy (38/50; 76%; Tables 1, 2) or by clinical and conventional imaging follow-up (12/50; 24%) for more than 2 years.
Breast MRI technique
Breast MRI was performed with a 1.5-T system (ACS II and ACS-NT; Philips Medical Systems, Best, The Netherlands) using a standard double-breast surface coil. The protocol consisted of a T2 turbo spin echo sequence (field of view, FOV, 280–320 mm; 31 slices with 3-mm slice thickness without a gap; echo time, TE/repetition time, TR/turbo factor 120 ms/3,800 ms/19; number of signals averaged 2; 512×512 matrix), followed by a rapid dynamic series (2D-gradient-echo technique) of seven dynamic images (TE/TR/flip angle, FA, 4.6 ms/260 ms/90°; full 256×256 matrix, 31 slices with a slice thickness of 3 mm without a gap; FOV 300–320 mm, temporal resolution 60 s) or a dynamic series of five dynamic image stacks (TE/TR/FA 4.6 ms/260 ms/90°; 384×512 matrix; 31 slices with a slice thickness of 3 mm without a gap; FOV 300–320 mm, temporal resolution 115 s).
The first series was obtained just before bolus injection of 0.1 mmol gadopentate dimeglumine (Magnevist; Schering, Berlin, Germany) per kilogram of body weight and a 20-ml saline solution flush. After the dynamic series, image subtraction was performed to suppress the signal from fat. Enhancement rates were quantified by region-of-interest-based analysis [24].
Data analysis
In a first step, two experienced breast radiologists (C.K.K., N.M.) interpreted breast magnetic resonance images (see detailed description in Ref. [1]) without additional information on clinical history, mammographic and ultrasonographic findings. The breast radiologists were asked to record the presence of a segmental or a linear enhancement pattern during the film reading for each breast MRI study.
Segmental enhancement was defined as non-mass-related enhancement with a triangular shape, the tip pointing to the nipple, corresponding to several ductal systems. Ductal enhancement was defined as non-mass-related enhancement presenting as a single line or several branching lines pointing to the nipple.
The magnetic resonance diagnosis was prospectively established for each patient after the breast radiologists had been provided with data on clinical history, mammographic and ultrasonographic findings in a second step.
We calculated the overall prevalence of linear and segmental enhancement in our unselected patient cohort (n=1,003 breast MRI studies). Furthermore, we calculated the prevalence of segmental and linear enhancement both for benign (n=859) and for malignant (n=144) breast disease.
In addition, the prevalence of segmental and linear enhancement was calculated separately for group A (patients with inconclusive clinical and conventional imaging findings), group B (preoperative staging of patients with suspected DCIS or invasive breast cancer), group C (follow-up after breast cancer) and group D (screening of patients with familial risk for breast cancer).
Based on the patients’ final diagnoses, we calculated specificity and the positive predictive value for the criterion “segmental and linear enhancement” on breast MRI. The positive predictive value was calculated for the unselected patient cohort and separately for patients from groups A–D.
In addition, we prospectively analyzed the internal architecture of enhancing DCIS and benign breast disease distinguishing between homogeneous and clumped enhancement patterns [14].
Statistics
For statistical analysis, the software packages SPSS (SPSS, Chicago, USA) and Excel 2000 (Microsoft, Redmond, USA) were used. The diagnostic indices (specificity, positive predictive value of segmental and linear enhancement) were calculated.
The Mann–Whitney U test (unpaired samples) was performed to evaluate the statistical significance of the enhancement pattern (homogeneous or clumped) for DCIS and benign breast disease. A p level of p<0.05 was considered significant.
Results
Patients’ final diagnoses
One hundred forty-four patients had malignant breast disease (120 invasive breast cancers, 24 DCIS). All invasive breast cancers of our study cohort presented as focal masses on breast MRI. Eight hundred fifty-nine patients had unsuspicious breast MRI studies or benign breast disease (Tables 1, 2).
Prevalence of segmental and linear enhancement
The overall prevalence of segmental and linear enhancement on breast MRI was 5% (50/1,003) for the unselected patient cohort.
Segmental and linear enhancement occurred in 33/859 (3.8%) patients with benign breast disease; high-risk lesions such as atypical ductal hyperplasia or lobular carcinoma in situ were not observed. None of those patients had suspicious microcalcifications on mammograms.
Segmental or linear enhancement was present for 17/24 (71%) patients with DCIS. For 4/24 (17%) patients, DCIS was visible as linear or segmental enhancement on breast MRI only, whereas no abnormalities were visible on the corresponding mammogram. On the other hand, 7/24 patients with DCIS had suspicious microcalcifications on mammograms, whereas the corresponding breast magnetic resonance images revealed only nonspecific focal contrast enhancement (6/7 patients) or absent enhancement (1/7 patient).
In group A, segmental and linear enhancement occurred for 19/326 (5.8%) patients, whereas it occurred more often for group B (8/81 patients; 9.8%), less frequently for group C (9/387; 2.3%) and nearly equally frequently for group D (14/209; 6.7%).
Diagnostic indices
The calculated positive predictive value of segmental and linear enhancement on breast MRI in the unselected patient cohort was 17/50 (34%) (Table 3).
The calculated positive predictive value of segmental and linear enhancement was 21% (4/19) for group A, whereas it was much higher for group B (7/8; 87.5%), higher for group C (4/9; 44.4%) and lower for group D (2/14; 14.2%). This criterion has a specificity of 96% (826/859).
Analysis of the internal architecture
Analysis of the internal archtitecture of segmental and linear enhancement revealed a homogeneous enhancement pattern for 33/50 (66%) patients (Fig. 1).

Prevalence of clumped and homogeneous enhancement pattern in intraductal breast cancer (DCIS) and in benign breast disease
A clumped internal architecture was present in 17/50 patients comprising 10/17 (59%) of the enhancing DCIS and 7/33 (21%) patients with benign breast disease. This difference was statistically significant (p=0.008).
Discussion
Mammographic screening has led to increased detection of DCIS. This tumor seldom (10%) presents with clinical symptoms such as palpable mass, nipple discharge or Paget’s disease of the nipple. Diagnosis of DCIS is mainly based on the detection of clustered microcalcifications on screening mammography. Liberman et al. [25] reported that the linear shape of microcalcifications and the segmental or ductal distribution of microcalcifications have a high positive predictive value for malignancy.
The potential of breast MRI in diagnosing DCIS is still a subject of controversial discussion. The few studies dealing with detection of DCIS by breast MRI show that DCIS has variable enhancement dynamics and enhancement kinetics. It has been pointed out that 10% of the DCIS did not enhance at all. Moreover, 30% of the enhancing DCIS showed a nonspecific enhancement that cannot be distinguished from fibrocystic breast disease [18].
On the other hand, Kuhl et al. [17] pointed out the meaning of morphologic criteria in the assessment of DCIS. The authors reported that segmental and ductal enhancement were the imaging hallmarks of DCIS on breast MRI and concluded that if additional morphological analysis of the enhancement pattern was performed, the sensitivity for the detection of DCIS on breast MRI could be significantly increased.
However, the specificity and the positive predictive value of segmental or linear enhancement are still unknown. To investigate the diagnostic usefulness of this criterion, we analyzed the prevalence of segmental and linear enhancement on breast MRI in an unselected patient cohort. We wondered whether segmental and linear enhancement were present only for malignant breast diseases or if they could be observed for benign breast diseases too.
Our data [26] show that the overall prevalence of segmental and linear enhancement on breast MRI is low. Only 5% (50/1,003) of the patients of the unselected patient cohort revealed this imaging feature on breast MRI.
Yet, it has to be noted that, in contrast to benign breast disease—such as fibrocystic breast disease, papilloma, focal mastitis or galactophoritis—which had a very low prevalence (3.8%; 33/259) for segmental or linear enhancement, the prevalence of this imaging finding was much higher with enhancing DCIS (71%; 17/24).
In our study population, segmental or linear enhancement was the most frequent manifestation of DCIS on dynamic breast MRI.
Although it was not the aim of this study to calculate the overall sensitivity of breast MRI regarding DCIS, we want to point out that breast MRI was able to diagnose additional conventionally occult DCIS. Four out of 17 (23%; 4/17) enhancing DCIS were visible on breast MRI only exhibiting segmental or linear enhancement, whereas they did not show any microcalcifications on the corresponding mammogram. The likelihood of DCIS was even higher if the internal architecture of the enhancement showed a clumped pattern [17].
The overall positive predictive value of the single MRI sign “linear or segmental enhancement” with regard to the diagnosis of DCIS was moderate (34%) but can be compared with the positive predictive value of the ductal distribution of microcalcifications on mammograms [25, 27].
Considering the different groups separately, it becomes obvious that the positive predictive value of segmental and linear enhancement was highest in group B patients who underwent breast MRI preoperatively. We want to point out that seven out of the eight patients of group B had been referred for preoperative breast MRI owing to suspicious microcalcifications on mammograms; these patients had mere DCIS. One out of the eight patients of group B was referred for breast MRI with the diagnosis of invasive breast cancer. The preoperative breast MRI revealed an additional segmental enhancement pattern in the contraleral breast, which was excised after MR-guided hook-wire placement and turned out to be adenosis. The positive predictive value was moderate for group C patients—who were in follow-up after breast conservative therapy—and group A patients (inconclusive clinical and conventional imaging findings) and was rather low for group D patients (patients with familial risk of breast cancer).
Leaving indications for breast MRI, we think that further work-up is needed if ductal enhancement occurs on breast MRI owing to the high prevalence of DCIS among segmental and linear enhancement on breast MRI. This recommendation also holds true for group D patients because these rather young patients have a very high risk of developing breast cancer.
The question arises how further work-up should be performed in the case of a ductal enhancement pattern on breast MRI. We recommend performing a targeted breast ultrasound examination first. If this targeted breast ultrasound examination reveals a correlate for the segmental enhancement pattern, biopsy can be performed under ultrasound guidance.
In our study, segmental and linear enhancement were visible on breast MRI only. Because we are not dealing with invasive breast cancer but at most with DCIS in the case of segmental or linear enhancement, further work-up can be performed either with short-term follow-up breast MRI or with immediate breast biopsy.
Meanwhile, vacuum-assisted core biopsy is also available under MR guidance [28]. Thus, a minimally invasive biopsy procedure that allows representative tissue sampling can be offered to the patient for further clarification.
Because group B patients are already scheduled for breast surgery, these patients should have preoperative MR-guided biopsy or MR-guided hook-wire placement of areas with ductal enhancement which do not have a correlate on mammograms, because diagnosis of additional conventionally occult DCIS could alter the patient’s treatment. For group A, group C and group D patients, it is a reasonable alternative to perform short-term follow-up breast MRI within 3 months because ductal enhancement may resolve in the case of benign breast disease. In these cases, the patients can undergo regular follow-up.
If ductal enhancement persists on the short-term follow-up breast MRI, these patients should also undergo MR-guided breast biopsy in order to rule out conventionally occult DCIS. If vacuum-assisted core biopsy reveals benign breast disease, these patients can also undergo regular follow-up.
In the meantime, a retrospective study [20] has largely confirmed our data. The authors of that study report a prevalence of 21% for ductal enhancement on breast MRI and a positive predictive value of 26%.
Our study has the following limitations. Because anaylsis of the magnetic resonance images was done in consensus, data on interobserver variability cannot be provided. Furthermore, we cannot provide histologic correlation for all 50 patients who had segmental or linear enhancement in the initial breast MRI study. Twelve patients (12/50) underwent short-term follow-up with breast MRI only and did not undergo MR-guided breast biopsy. For those patients, malignancy was excluded because segmental or linear enhancement disappeared on short-term follow-up breast MRI studies within 3–6 months. In addition, conventional imaging of those patients was inconspicuous. It is important to note that none of those patients developed breast cancer in the meantime. Therefore, we assume that the previous segmental or linear enhancement was due to spontaneous enhancement, fibrocystic disease, focal mastitis or galactophoritis.
Conclusion
The overall prevalence of a ductal or a segmental enhancement pattern on breast MRI is low. This finding has a high specificity and a moderate positive predictive value for intraductal neoplastic changes. We conclude that if segmental or linear enhancement is identified on breast MRI further work-up is necessary. We recommend either direct MR-guided vacuum-assisted core biopsy or short-term follow-up breast MRI within 3–6 months. If ductal enhancement then persists, MR-guided biopsy should be recommended even in the absence of mammographically visible signs of DCIS (Figs. 2, 3, 4, 5).

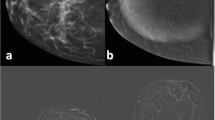
Sixty-seven-year-old patient with an inconclusive screening mammogram (BI-RADS 3) of her left breast (not shown). Dynamic breast MRI revealed a segmental enhancement pattern in the centre of the right breast. No microcalcifications were seen in the right breast with conventional mammography (not shown). MR-guided core biopsy (not shown) was performed and revealed extensive DCIS. The patient was treated by mastectomy. a Precontrast axial T1-weighted gradient echo image (repetition time TR/echo time TE/flip angle FA 260 ms/4.6 ms/90°) of the dynamic series. b Axial, postcontrast T1-weighted gradient echo image of the dynamic series (TE/TR/FA 4.6 ms/260 ms/90°). c Axial subtracted image of the dynamic series. Note the triangular shape (white arrow) of the enhancing area with clumped internal architecture.

Forty-year-old patient with familial breast cancer. Dynamic breast MRI showed a segmental enhancement pattern (white arrow) behind the left nipple with homogeneous internal architecture. No suspicious microcalcifications were visible on conventional mammograms (not shown). Excisional biopsy after MR-guided hook-wire placement (not shown) revealed fibrocystic breast disease. a Precontrast axial T1-weighted gradient echo image (TR/TE/FA 260 ms/4.6 ms/90°) of the dynamic series. b Axial, postcontrast T1-weighted gradient echo image of the dynamic series (TE/TR/FA 4.6 ms/260 ms/90°). c Axial subtracted image of the dynamic series. Note the almost triangular shape (arrow) of the enhancing area with homogeneous internal architecture.

Thirty-two-year-old patient who presented with bloody nipple discharge of her right breast. No microcalcifications were detectable on conventional mammograms (not shown). Breast MRI showed linear enhancement (long arrow) in the right breast. Note that the ducts still contain blood (open arrow). MR-guided hook-wire placement (not shown) revealed papilloma. a Precontrast axial T1-weighted gradient echo image (TR/TE/FA 260 ms/4.6 ms/90°) of the dynamic series. b Axial, postcontrast T1-weighted gradient echo image of the dynamic series (TE/TR/FA 4.6 ms/260 ms/90°). c Axial subtracted image of the dynamic series. Note the linear enhancement (long arrow) behind the nipple.

Fourty-four-year-old patient with a history of DCIS of her right breast. Follow-up breast MRI revealed linear enhancement in the centre of the right breast. X-ray mammography (not shown) did not show suspicious microcalcifications. MR-guided hook-wire placement (not shown) revealed recurrent DCIS. a Precontrast axial T1-weighted gradient echo image (TR/TE/FA 260 ms/4.6 ms/90°) of the dynamic series. b Axial, postcontrast T1-weighted gradient echo image of the dynamic series (TE/TR/FA:4.6 ms/260 ms/90°). c Axial subtracted image of the dynamic series. Note the linear enhancement (arrow) behind the nipple.
References
Kuhl CK (2000) MRI of breast tumors. Review article. Eur Radiol 10:46–58
Wasser K, Sinn HP, Fink C et al (2003) Accuracy of tumor size measurement in breast cancer using MRI is influenced by histological regression induced by neoadjuvant chemotherapy. Eur Radiol 13:1213–1223. Epub 2002 Nov 30
Kristofferson Wiberg M, Aspelin P, Sylvan M, Bone B (2003) Comparison of lesion size estimated by dynamic MR imaging, mammography and histopathology in neoplasms. Eur Radiol 13:1207–1212. Epub 2002 Nov 19
Dao TH, Rahmouni A, Campana F (1993) Tumor recurrence versus fibrosis in the irradiated breast: differentiation with dynamic gadolinium-enhanced MR imaging. Radiology 751:187
Fischer U, Kopka L, Grabbe E (1999) Breast carcinoma: effect of preoperative contrast-enhanced MR imaging on the therapeutic approach. Radiology 213:881–888
Liberman L, Morris EA, Kim CM, Kaplan JB, Abramson AF, Menell JH, Van Zee KJ, Dershaw DD (2003) MR imaging findings in the contralateral breast of women with recently diagnosed breast cancer. Am J Roentgenol 180:333–341
Lee SG, Orel SG, Woo IJ, Cruz-Jove E, Putt ME, Solin LJ, Czerniecki B, Schnall MD (2003) MR imaging screening of the contralateral breast in patients with newly diagnosed breast cancer: preliminary results. Radiology 226:773–778
Schelfout K, Van Goethem M, Kersschot E et al (2004) Preoperative breast MRI in patients with invasive lobular breast cancer. Eur Radiol 14:1209–1216. Epub 2004 Mar 18
Kuhl CK, Schmutzler RK, Leutner CK, Kempe A, Wardelmann E, Hocke A, Maringa M, Pfeifer U, Krebs D, Schild HH (2000) Breast MR imaging screening in 192 women proved or suspected to be carriers of a breast cancer susceptibility gene: preliminary results. Radiology 215:267–279
Gilles R, Zafrani B, Guinebretiere JM et al (1995) Ductal carcinoma in situ: MR-imaging–histopathologic correlation. Radiology 196:415–419
Heywang SH (1994) Contrast-enhanced magnetic resonance imaging of the breast. Invest Radiol 29:94–104
Harms SE, Flaming DP, Hesley KL et al (1993) MR imaging of the breast with rotating delivery of excitation off resonance: clinical experience with pathologic correlation. Radiology 187:493–501
Tesoro-Tess JD, Amusoro A, Rovini D et al (1995) Microcalcifications in clinically normal breasts: the value of high field, surface coil, Gd-DTPA-enhanced MRI. Eur Radiol 5:417–422
Sonderstrom CE, Harms SE, Copit DS et al (1996) Three-dimensional RODEO breast MR imaging of lesions containing ductal carcinoma in situ. Radiology 201:427–431
Neubauer H, Li M, Kuehne-Heid R, Schneider A, Kaiser WA (2003) High grade and non-high-grade ductal carcinoma in situ on dynamic MR mammography: characteristic findings for sign increase and morphological pattern of enhancement. Br J Radiol 76:3–12
Gilles R, Meunier M, Lucidarme O et al (1996) Clustered breast microcalcifications: evaluation by dynamic contrast-enhanced subtraction MRI. J Comput Assist Tomogr 20:9–14
Kuhl CK, Mielcarek P, Leutner CC, Schild HH. Diagnostic criteria of ductal carcinoma in situ (DCIS) in dynamic contrast-enhanced breast MRI: comparison with invasive breast cancer (IBC) and benign lesions. Proc. Int. Soc. Magn Reson Med 1998 p 93
Fischer U, Westerhof JP, Brinck U, Korabiowska M, Schauer A, Grabbe E (1996) The ductal carcinoma in situ in contrast enhanced dynamic MR mammography. RöFo 164:290–294
Westerhof JP, Fischer U, Mortiz JD, Oestmann JW (1998) MR imaging of mammographically detected clustered microcalcifications: is there any value? Radiology 207:675–681
Liberman L, Morris EA, Dershaw DD, Abramson AF, Tan LK (2003) Ductal enhancement on MR imaging of the breast. Am J Roentgenol 181(2):519–525
Orel S, Medonca MH, Reynolds C, Schnall M, Lawrence JS, Sullivan DC (1997) MR imaging of ductal carcinoma in situ. Radiology 202:413–420
Liberman L, Morris EA, Lee M, Kaplan JB, La Trenta LR, Menell JH, Abramson AF, Dashnow SM, Ballon DJ, Dershaw DD (2002) Breast lesions detected on MR imaging: features and positive predictive value. Am J Roentgenol 179:171–178
Van Goethem M, Schelfout K, Kersschot E et al (2004) Enhancing area surrounding breast carcinoma on MR mammography: comparison with pathological examination. Eur Radiol 14:1363–1370; Epub 2004 Mar 26
Kuhl CK, Mielcarek P, Klaschik S, Leutner C, Wardelmann E, Gieseke J, Schild HH (1999) Dynamic breast MR imaging: are signal intensity time course data useful for differential diagnosis of enhancing lesions? Radiology 211:101–110
Liberman L, Abramson AF, Squires FB, Glassman JR, Morris EA, Dershaw DD (1998) The breast imaging and reporting data system: positive predictive value of mammographic features and final assessment categories. Am J Roentgenol 171:35–40
Morakkabati N, Schmiedel A, Leutner C, Kuhl CK (2000) Diagnostic usefulness of ductal or segmental enhancement in dynamic breast MR imaging. Radiology 217(P):526–527
Gulsun M, Demirkazik FB, Ariyurek M (2003) Evaluation of breast microcalcifications according to breast imaging reporting and data system and Le Gal’s classification. Eur Radiol 32:227–231
Lehman CD, Aikawa T (2004) MR-guided vacuum-assisted breast biopsy: accuracy of targeting and success in sampling in a phantom model. Radiology. 232:911–914
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Morakkabati-Spitz, N., Leutner, C., Schild, H. et al. Diagnostic usefulness of segmental and linear enhancement in dynamic breast MRI. Eur Radiol 15, 2010–2017 (2005). https://doi.org/10.1007/s00330-005-2755-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-005-2755-4