
Abstract
The objective of the study was to evaluate MRI for visualization of acromioclavicular (ac) joint structures in cadaveric shoulders, asymptomatic volunteers and symptomatic patients with trauma of the ac-joint. Three cadaveric shoulders were examined to find adequate planes and sequences for MRI. Afterwards, MR images were correlated to corresponding anatomical sections. Six asymptomatic volunteers and 13 patients were scanned in a 1.5 T Magnetom Vision with three sequences in the following planes: (1) parallel to the clavicle; (2) orthogonal to the ac joint, each time a fat-suppressed proton density-weighted + T2-sequence (TR/TE 4,000/15 ms) was performed; (3) parallel to the clavicle, T1-SE (TR/TE 817/20 ms). The parameters were: slice thickness 3 mm, field-of-view 180 mm, matrix 210×256 pixels. Standard of reference in the patients was clinical examination and conventional X-rays. Classification was by Rockwood grades I–VI. MRI allowed excellent visualization and diagnoses of ac-joint structures in volunteers and patients (n=6 normal, n=1 Rockwood I, n=5 Rockwood II, n=3 Rockwood III, n=4 Rockwood V). On MRI, in one lesion type II and III each, a lower lesion type was suspected clinically and by X-ray. In one patient additional information by MRI led to surgery. MRI allows excellent anatomical display of ac-joint structures and can give clinically relevant information on type and extension of ac-joint trauma, which may influence therapy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acromioclavicular (ac) joint disruptions are very common and are caused by direct or indirect trauma, occurring in more than 10% of shoulder injuries. The lateral part of the clavicle is usually dislocated superiorly or, less frequently, posteriorly. The ac joint is stabilized by the joint capsule, the acromioclavicular ligament that enhances the cranial stability, and the coracoclavicular ligament, which is composed of the lateral trapezoid and the medial conoid part. The trapezoid ligament is the primary restraint against posterior clavicular displacement [1] and also provides resistance against superior, inferior, and anterior forces. The conoid ligament is the main restraint against anterior or superior displacement of the clavicle, but also against rotation of the bone anteriorly or posteriorly [2]. Two muscles are attached to the scapular spine and acromion: the trapezius and the deltoid muscle.
The current status in diagnosing acromioclavicular joint instability is based on clinical examination and plain radiography. Additionally, a weighted view is usually necessary. In a small number of cases an ultrasound of the shoulder is performed. The well-known grading of ac joint injuries is classified according to Rockwood et al. [3]. Their classification [3] includes three more rare types of ac joint derangements than the Tossy classification [4]. Diagnosis of the real extent of injuries of the coracoclavicular and acromioclavicular ligaments is very difficult with the established examination methods. For therapeutical planning an exact information about the injury type is absolutely necessary, especially for the differentiation between a Rockwood II and a Rockwood III injury. With diagnosis based on conventional methods, important information about the joint stability may be lost if it is not possible to distinguish between complete and incomplete acromioclavicular dislocations. Another problem for exact diagnosis with the conventional techniques is the large variability of the ac joint, especially concerning the ac joint distance, which varies from 5 mm in the general population to 6 mm or 7 mm in elderly patients.
It is still controversially discussed whether to choose conservative or operative treatment for Rockwood III and higher lesions. The current classification systems may be not exact enough to classify the pathoanatomy of the ac joint injuries and indicate the best individual treatment for the patient. In recent years MRI has developed as an alternative non-invasive diagnostic tool, and the use of MRI to diagnose shoulder joint lesions is well established.
The purpose of our study was first to evaluate MRI of cadaveric shoulders for detailed visualization of ac joint structures and find out the best planes and sequences. Secondly, volunteers and symptomatic patients with trauma of the ac joint were prospectively examined. The primary goal was to find out whether MRI can provide more information than conventional examination and thus improve the classification of these injuries and influence therapeutic strategies for a better clinical outcome.
Materials and methods
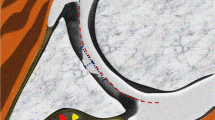
The study protocol was approved by the local ethics committee. Firstly, three thawed, freshly frozen normal cadaveric shoulders were examined by MRI in order to define the best imaging planes and sequences for visualization of the acromioclavicular and coracoclavicular ligaments. Imaging was done on a 1.5 T scanner (Magnetom Vision, Siemens, Erlangen, Germany) with a dedicated shoulder coil. The imaging protocol included three sequences in the following planes: (1) parallel to the clavicle; (2) orthogonal to the ac joint, each time a fat-suppressed (FS) proton density-weighted (PDw) + T2-weighted sequence (TR/TE 4,000/15 ms) was performed; (3) parallel to the clavicle when a T1 SE (TR/TE 817/20 ms) sequence was performed (cf. Fig. 1). Other imaging parameters were identical: slice thickness 3 mm, field of view (FOV) 180 mm, matrix 210×256 pixels. Acquisition time was 14 min for the entire protocol. Afterwards the cadaveric specimens were sectioned along the imaging planes using a bandsaw. The obtained MRI scans were then correlated with the anatomical sections to compare the accuracy and quality of visualizing the acromioclavicular and coracoclavicular ligaments by MRI.

Orientation for FS PDw + T2 TSE-sequence was parallel to the clavicle (a) and orthogonal to the ac joint (b). A T1-SE sequence was performed parallel to the clavicle. CP coracoid process, CA coracoacromial ligament, Tr trapezoid ligament, Co conoid ligament, AL acromioclavicular ligament
Six asymptomatic volunteers (mean age 29 years; range 25 years to 35 years) without any symptoms in the ac joint underwent our MRI protocol in order to confirm the applicability of the sequences and planes in a clinical setting. Thirteen patients (mean age 39 years; range 21 years to 55 years) with suspected ac joint injury were then included in our study within 18 consecutive months. All volunteers and patients signed written informed consent forms. Image packets were interpreted by two readers, a fellow (F.K.S., 4 years of musculoskeletal experience) and an experienced musculoskeletal radiologist (J.B., 15 years of musculoskeletal experience). Diagnosis was made by consensus. Standard of reference was clinical examination and plain radiographs of the injured and uninjured shoulders. MR findings were correlated with surgical results in all patients that went on to receive surgery.
According to the Rockwood [3] classification the patient’s injury was categorized from type I–VI. MR images demonstrating each type of Rockwood injury were presented in a pictorial essay by Antonio et al. in 2004 [5]. Rockwood I shows normal X-ray findings; the acromioclavicular ligaments are clinically sprained. There are no specific MRI signs for this type of injury because signal abnormalities are common in the ac joint in adult patients [5]. In Rockwood II, radiographic findings present ac joint widening; coracoclavicular interspace is normal or slightly enlarged. Injuries of the anatomic structures consist of disrupted acromioclavicular ligaments, sprained coracoclavicular ligaments, identified in MRI as oedema, whereas trapezoid and deltoid muscles are intact. In grade III lesions, X-ray findings show that ac joint dislocation and coracoclavicular interspace are increased by 25% to 100%. Clinically, the acromioclavicular and coracoclavicular ligaments are disrupted, and trapezoid and deltoid muscles are detached from the distal part of the clavicle. In MRI oedema, blood and fluid are seen in the coracoclavicular and acromioclavicular interspace. Rockwood IV lesions describe a situation where, clinically, in radiographic findings and in MRI, the coracoclavicular space may be widened or appears equal to the normal shoulder. In grade IV injury the acromioclavicular ligaments are disrupted, the ac joint is dislocated, the clavicle is displaced posteriorly in the trapezoid muscle, and the trapezius and deltoid muscles are detached from the distal part of the clavicle. Radiographic findings in grade V lesions represent dislocations of the ac joint, and coracoclavicular interspace is more than 100% greater than in the normal shoulder. Anatomically and in MRI findings, the acromioclavicular and coracoclavicular ligaments are disrupted and the trapezoid and deltoid muscles are detached from the lateral half of the clavicle. In type VI lesions, the ac joint is dislocated, and the clavicle is displaced inferiorly to the coracoid on plain films. Anatomically and in MRI the acromioclavicular and coracoclavicular ligaments are disrupted and the trapezoid and deltoid muscles are detached from the clavicle.
Results
The two planes chosen in the examination of three cadaveric shoulders for the study accurately depicted the normal anatomy of the ac joint capsule as well as the trapezoid and conoid ligaments. A precise definition of the origin and insertion of the acromioclavicular and coracoclavicular ligaments, as well as their complete delineation and an evaluation of the capsule of the ac joint, was possible. MR images obtained of the cadaveric shoulders and corresponding anatomical slices are shown in Fig. 2. Afterwards, the defined planes were applied in six healthy volunteers, with no symptoms in the ac joint, who underwent our developed MRI protocol. These six volunteers presented with normal ligaments and ac joints. In each case the structures of the ligaments and ac joint capsule were visualized excellently.

a Orientation is parallel to the clavicle in FS-PD-TSE and FS-T2-TSE corresponding slice of the cadaveric shoulder. GHJ glenohumeral joint, CP coracoid process. The arrow marks trapezoid ligament fibres. b Orientation parallel to the clavicle in a FS-PD-TSE sequence. The MR image shows the ac joint capsule with the hyperintense disc (arrow) and the intermediate signal of the acromioclavicular ligament. HH humerus head, AC acromion
On the T1-weighted SE images, the anatomy of the coracoclavicular ligaments without trauma was very well delineated due to the high signal-to-noise ratio. In the FS PD/T2-weighted images the ligamentous structures were not identified very easily in cases of no clinically suspected ac joint pathology, whereas oedematous fluid or blood provided better visualization of the ligamentous fibres in cases of injury. Contrarily, it was more difficult to evaluate the T1-weighted SE images of blood and fluid within the substance or surrounding mass of the ligaments.
In the 13 patients the following diagnoses were made based on MRI (Table 1): one patient had a Rockwood stage I lesion on MRI and correlating clinical/X-ray findings. Five patients were diagnosed with Rockwood II on MRI, clinically, and by plain radiographs; one lesion was underestimated as type I; in this case we found, on MRI, elongation and discrete oedema of the conoid and trapezoid ligaments and a partial rupture of the acromioclavicular ligament; the clinical and X-ray findings were suspicious for only a type I lesion with even unsuspicious X-ray findings in the weighted view. Three patients were diagnosed with Rockwood stage III lesions on MRI, whereas two cases were classified equally on clinical examination and radiography; in one case the clinical and X-ray findings of the lesion were underestimated as type II, for we saw in the injured shoulder only a slightly greater distance of the ac joint and a slightly superiorily displaced clavicle; on MRI we diagnosed a disrupted acromioclavicular ligament and a partial rupture of the coracoclavicular ligament, resulting in a more precise diagnosis than with conventional radiography (cf. Fig. 3). Four patients had a Rockwood V lesion, classified equally on clinical examination and radiography and MRI. All four patients with Rockwood V injury and two of three patients with Rockwood stage III lesions underwent surgical therapy. The surgeon could correlate the diagnosed lesions by MRI exactly in each case. The one patient with Rockwood II classification on clinical examination and on radiography and with Rockwood stage III on MRI was referred to surgical therapy with corresponding findings on surgery.

a Conventional plain radiograph of the injured right shoulder with discrete widening of ac joint (arrow) and slightly superior position of the clavicle, diagnosed as Rockwood II injury, and plain radiographs after surgical treatment with hook plate in a 28-year-old patient. b FS-PD-TSE MR images, orientated parallel to the clavicle, with dislocation of the ac joint and partial rupture and oedema (arrowhead) of the coracoclavicular ligament, classified as a Rockwood type III injury. c In the same orientation T1-SE images show the extent of the injury. HH humerus head, CP coracoid process
Discussion
Lesions of the ac joint are very common in shoulder injuries. Different classification systems according to Rockwood [3] and Tossy [4] are used to describe the pathoanatomical situation in the injured ac joint. In these classifications, the decision for surgical or non-surgical treatment is based on the integrity of the coracoclavicular ligaments. There is no dissent that Rockwood I and II lesions should be treated conservatively [6–9] and that Rockwood IV–VI lesions should be treated surgically. The discussion concerning the treatment of Rockwood III lesions is still controversial. Rockwood III lesions account for up to 40% of all ac joint injuries [9]. It is difficile to diagnose those lesions by clinical examination and on plain radiographs. MRI provides an excellent opportunity for non-invasive visualization of the ac joint and its ligaments [5].
Requirements for a well-defined musculoskeletal examination is a MRI protocol with a balanced combination of high sensitivity for visualization of free water molecules, high spatial resolution and short acquisition time. Most pathological findings in the musculoskeletal system show an accumulation of free water, for example in cases of joint effusion, inflammation, bone bruise, injury of ligaments, and joint capsule. Thus, high sensitivity in MRI sequences for free water-bound protons is necessary. Fat-suppressed MRI sequences offer the possibility of a higher contrast-to-noise ratio for oedematous pathological tissue-like injured ac joint ligaments by eliminating the signal of fat-bound protons. The fat-suppressed PD/T2w TSE sequences allow visualization of abnormal focal or diffuse increased signal in the acromioclavicular and coracoclavicular ligaments within the substance or surrounding mass, as the ligaments’ morphology then is altered by disruption of fibres or complete tear.
In recent years the use of fast spin-echo, also known as turbo spin-echo, sequences has become very popular. Fast spin-echo sequences have, meanwhile, replaced conventional SE sequences in many applications in the whole body. The advantages of TSE sequences are reduction of acquisition time and motion artefacts. The time saving allows higher patient throughput or performance of additional sequences. The TSE sequences provide images of comparable contrast and quality to standard SE sequences.
Aware of these important factors of an optimized MRI protocol for the examination of the ac joint, we suggest the use of slice orientations parallel to the clavicle and orthogonal to the ac joint, which we considered was the best for the ac joint in our examination of the three cadaveric shoulders. The protocol was confirmed by examination of six healthy volunteers. At a total acquisition time of 14 min our study protocol included orientations parallel to the clavicle and orthogonal to the ac joint, using a FS PD/T2 TSE sequence in both planes and a T1-weighted SE sequence parallel to the clavicle.
In the case of a Rockwood I lesion we found only discrete oedema in the ac joint capsule. However, this is not a specific finding because of the variation of signal abnormalities and appearance of ac joints depending on the patient’s age. In Rockwood II lesions we diagnosed ruptured acromioclavicular ligaments and, additionally, sprained and oedematous coracoclavicular ligaments, which were very well visualized on the FS PD/T2 TSE sequences. In one case of a Rockwood II lesion, MRI provided additional information compared to the clinical and X-ray examination, that resulted in underestimation as a type I lesion. Nevertheless, there was no influence on therapy. For Rockwood III lesions, which are usually caused by a strong force leading to ac joint dislocation, we could diagnose partially and completely ruptured trapezoid and coronoid ligaments. With the long TR time in the FS PD/T2 TSE sequence the fibres were easy to identify, even in the presence of oedema, fluid, and blood (cf. Fig. 4). In one case of only partial rupture of the coracoclavicular ligament in a young athlete, we classified the lesion as Rockwood type III on MRI, whereas it was underestimated as a type II lesion clinically and on plain radiographs. This patient underwent surgical therapy based on the additional information on MRI. The very rare Rockwood IV and VI lesions were not present in our patients, but they should certainly be detectable with the suggested MRI protocol. All four Rockwood V lesions were detected both on plain radiographs and MRI. In these patients acromioclavicular and coracoclavicular ligaments were disrupted, the ac joint was dislocated, and oedema and blood were seen in the trapezoid and deltoid muscles, which were detached from the lateral half of the clavicle (cf. Fig. 4).

a FS PD -TSE-sequence, parallel to the clavicle, shows the fibres of the ligaments, which are easy to identify, even when they are elongated and partially torn or there is oedema, fluid and blood (arrowhead). In this case we diagnosed a partial rupture of the coracoclavicular ligament and disruption of the acromioclavicular ligament (Rockwood stage II). b Plain radiographs where only soft tissue swelling is diagnosed in the ac joint. c A slightly larger distance is seen in the ac joint and discrete superior clavicle position in the injured right shoulder than in the uninjured left shoulder under weight bearing. HH humerus head, AC acromion, CP coracoid process
MRI of the ac joint is not practicable for use on a routine basis because of costs and local availability [10]. Nevertheless, MRI may support the radiologist in finding the correct diagnosis by offering important additional information about the soft tissue in the shoulder, especially if a Rockwood type III or more severe lesion is suspected. The final goal is to support the orthopaedic surgeon by giving detailed information about the extent of the injury to reduce pain, prevent ac joint degeneration and consequently mechanical problems in the shoulder girdle and to improve the range of motion. Surgically, various techniques are available and practicable to stabilize the clavicle using different forms of fixation or reconstruction of the ac joint. Currently, we suggest performing an additional MRI, if it remains unclear clinically and on plain radiographs whether to treat surgically, arthroscopically, or conservatively. Expecting minimal morbidity, we consider arthroscopy as treatment modality of choice, and, therefore, prior to surgery, exact information on the extent of the injury in the shoulder is necessary. The results of our study also show that MRI can play a decisive role in detecting slight differences with influence on the diagnosis classification. Thus, even in the Rockwood III subgroup, we could demonstrate a partial rupture of the coracoclavicular ligament and make a more precise diagnosis than with conventional techniques, where this case was underestimated.
In summary, MRI with our scan parameters and scan orientation is time saving and provides accurate information concerning the status of the ac joint ligaments, especially with regard to the essential role of the coracoclavicular ligament in maintaining the ac joint’s stability and function. We recommend this protocol in addition to a complete shoulder MRI protocol in the case of a complex shoulder trauma. A potential limitation is to be seen in the relatively small study population. Further, MRI is an imaging modality that allows direct classification of injury and offers an objective and reproducible method of diagnosis.
References
Lee KW, Debski RE, Chen CH, Woo SL, Fu FH (1997) Functional evaluation of the ligaments at the acromioclavicular joint during anteroposterior and superoinferior translation. Am J Sports Med 25:858–862
Fukuda K, Craig EV, An KN, Cofield RH, Chao EY (1986) Biomechanical study of ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am 68:434–440
Rockwood CA, Williams GR, Young DC (1996) Injuries to the acromioclavicular joint. In: Rockwood CA, Green DP, Buchholz RW, Heckman (eds) Fractures in adults, 4th edn. Lippincott-Raven, CD ROM, Philadelphia
Tossy JD, Mead NC, Sigmond HM (1963) Acromioclavicular separations: useful and practical classification for treatment. Clin Orthop 28:111–119
Antonio GE, Cho JH, Chung CB, Trudell DJ, Resnick D (2003) Pictorial essay. MR imaging appearance and classification of acromioclavicular joint injury. AJR Am J Roentgenol 180:1103–1110
Blazar PE, Iannotti JP, Williams GR (1998) Anteriorposterior instability of the distal clavicle after distal clavicle resection. Clin Orthop 348:114–120
Guy DK, Wirth MA, Griffin JL, Rockwood CA Jr (1998) Reconstruction of chronic and complete dislocations of the acromioclavicular joint. Clin Orthop 347:138–149
Lemos MJ (1998) The evaluation and treatment of the injured acromioclavicular joint in athletes. Am J Sports Med 26:137–144
Buckholz RW, Heckman JD (2001) Rockwood and Green’s fracture in adults, 5th edn. Lippincott Williams and Wilkins, Philadelphia, pp 1210–1244
Barnes CJ, Higgins LD, Major NM, Basamania CJ (2004) Magnetic resonance imaging of the coracoclavicular ligaments: its role in defining pathoanatomy at the acromioclavicular joint. J Surg Orthop Adv 13:69–75
Acknowledgements
We would like to thank Prof. Dr. B. Tillmann and R. Klaws, Department of Anatomy of the Christian-Albrechts University of Kiel, who further support this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schaefer, F.K., Schaefer, P.J., Brossmann, J. et al. Experimental and clinical evaluation of acromioclavicular joint structures with new scan orientations in MRI. Eur Radiol 16, 1488–1493 (2006). https://doi.org/10.1007/s00330-005-0093-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-005-0093-1