
Abstract
Objectives
To assess the accuracy of CT for the diagnosis of histologically confirmed adrenal adenoma and nonadenoma using CT numbers.
Materials and methods
Our study included 91 adrenal masses in 83 patients; histopathological diagnoses were 45 adenomas, 31 pheochromocytomas, 6 hyperplasias, 4 metastasis, and 5 miscellaneous lesions. Unenhanced CT in 46 patients and unenhanced and delayed contrast-enhanced (DCE) CT in 37 patients were retrospectively reviewed to examine the correlation between CT findings and those on pathological examination and to obtain diagnostic accuracy.
Results
Sensitivity, specificity, and accuracy for adenoma were 40% (18/45), 91% (42/46), and 66% (60/91) with unenhanced CT, and 96% (24/25), 61% (11/18), and 81% (35/43) with DCE CT. Adrenal masses falsely diagnosed as adenoma on unenhanced CT included three hyperplasias and one endothelial cyst, and those falsely diagnosed as adenoma on DCE CT were five pheochromocytomas, one oncocytic coritical tumor, and one primary pigmented nodular adrenocortical dysplasia. Twenty-five lipid-poor adenomas were falsely diagnosed as nonadenomas on unenhanced CT and one degenerated adenoma both on unenhanced CT and on DCE CT.
Conclusion
Diagnosing adenoma merely on CT numbers can lead to misdiagnosis. The lower specificity than expected is due to pheochromocytomas presenting as false positives.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Computed tomography (CT) has become the most commonly used modality in differentiating adrenal adenoma from nonadenoma. Boland et al. [1] reported that unenhanced CT shows low sensitivity and high specificity for adenoma using meta-analysis of threshold values from several studies. Delayed contrast-enhanced (DCE) CT yields both high sensitivity and high specificity in characterizing adrenal masses [2–5]. However, most of these studies have limitations as the final diagnosis was not based on pathological findings but largely on clinical or radiological findings. Without pathological diagnosis it may be difficult to obtain true sensitivity, specificity, or accuracy of commonly used diagnostic criteria for adrenal adenoma such as attenuation values less than 10 HU on unenhanced CT and rapid washout of enhancement on DCE CT. The purpose of this study was to assess the accuracy of CT for the diagnosis of histologically confirmed adrenal adenomas and nonadenomas including pheochromocytoma, metastasis, hyperplasia, and miscellaneous adrenal tumors using CT numbers.
Materials and methods
Patients
Our institutional review board approved our study which was carried out between June 1999 and May 2004 in 83 patients (33 men, 50 women; mean 45.4 years, range 19–68). There were 91 pathologically confirmed adrenal masses that were retrospectively searched from a computerized database; 86 underwent adrenalectomy and one excisional biopsy. CT-guided core biopsy was performed in one mass of the remaining four adrenal masses, which were detected in one patient with small cell carcinoma of the lung. All of adrenal masses in the patient with lung cancer showed rapid increase in size on the follow-up CT performed 3 months later. Pathological diagnoses of these masses included 45 cortical adenomas, 31 pheochromocytomas, 6 adrenal hyperplasia, 4 metastasis, and 5 miscellaneous lesions including one oncocytic cortical tumor, one primary pigmented nodular adrenocortical dysplasia, one ganglioneuroma, one endothelial cyst, and one pseudocyst. The surgical indications were as follows: clinically or biochemically functioning adrenal masses including 36 adenomas and 31 pheochromocytomas. The patients showed Cushing syndrome (n=23), Conn's syndrome (n=13), and elevated level of urine vanillylmandelic acid or urine/serum catecholamine (n=31). The remaining adrenal masses were surgically resected because of the presence of concurrent or previous cancer history (n=4), lesions that did not meet CT criteria for adenoma (n=4), and pressure symptom due to large adrenal masses (n=12).
Computed tomography
CT was performed with either a single detector unit (HiSpeed advantage, GE Medical Systems, Milwaukee, Wis., USA) or three multidetector units (LightSpeed QX/I, LightSpeed ultra8, LightSpeed ultra16; GE Medical Systems). Imaging parameters for unenhanced and contrast-enhanced CT included 2.5- or 5-mm collimation, 1:1 pitch for single detector, 0.75 or 0.875, 1 pitch for multidetector, 120 kVp, and 180–240 mA. Enhanced scans were obtained after intravenous administration of 120 ml iopromide (Ultravist 370, Schering, Germany), iomeprol (Iomeron, Ilsung, Seoul, Sourth Korea) and iohexol 300 (Omnipaque, Nycomed, New York, N.Y., USA) with a power injector at a rate of 3 ml/s.
Unenhanced and contrast-enhanced CT was performed in 46 patients with 48 adrenal masses 60 s and/or 3 min after intravenous administration of contrast material. These unenhanced CT images were evaluated, but these contrast-enhanced CT images were excluded in our study because DCE CT was not conducted. In 37 patients with 43 lesions unenhanced and contrast-enhanced CT was carried out 60 s (early contrast-enhanced) or 15 min (delayed contrast-enhanced) following intravenous administration of contrast material.
Imaging analysis
CT attenuation values were measured by using a round region of interest (ROI) on an imaging plane where the adrenal mass measures maximum transverse diameter. The ROI covered the solid area of the adrenal mass as large as possible, excluding cystic, necrotic or calcified regions except for cystic masses (n=2) or totally necrotic or cystic masses with thin wall (n=1). The peripheral areas of the adrenal mass were avoided to prevent partial volume averaging. The mean attenuation value was calculated from at least two measurements obtained for each mass at the same level through all phases. The absolute percentage enhancement washout values (PEWV) were calculated according to the following formula [5]: PEWV=(attenuation value at early enhanced CT-attenuation value at delayed enhanced CT)×100/(attenuation value at early enhanced CT-attenuation value at unenhanced CT). The diagnosis of adenoma was made if a mass had an attenuation value of 10 HU or less on unenhanced CT or an absolute PEWV of greater than 60% on DCE CT [2, 3, 5].
Adrenal masses were classified into adenomas and nonadenoma subgroups including pheochromocytoma, hyperplasia, metastasis, and miscellaneous lesions according to the pathological diagnosis. Their mean attenuation values and absolute PEWV were analyzed and compared between the two groups. However, CT number and absolute PEWV of miscellaneous lesions in the nonadenoma group were excluded from the comparison because of their heterogeneous composition of disease. CT-based diagnosis was correlated with that of pathological examination and the sensitivity, specificity, and positive and negative values, and overall accuracy for the diagnosis of adrenal adenoma were obtained. The adrenal lesions mimicking adenomas on unenhanced and/or DCE CT were analyzed and examined in relation to pathological findings.
Statistical analysis
The mean attenuation values on unenhanced CT and absolute PEWV on DCE CT were compared between adenoma and nonadenoma subgroups using one-way analysis of variance with post hoc multiple comparisons. Differences with a P value less than 0.05 were considered statistically significant.
Results
The mean attenuation values of adenoma, pheochromocytoma, metastaisis, and hyperplasia on unenhanced CT and absolute PEWVs on DCE CT are shown in Table 1. The mean attenuation value of adenomas was significantly lower than that of pheochromocytoma and metastasis (P<0.05) but was not significantly different from hyperplasia at unenhanced CT (P>0.05). However, the mean attenuation value of pheochromocytoma did not differ significantly from that of metastasis at unenhanced CT (P>0.05). Figure 1 graphically illustrates the comparison of the mean attenuation values between adenoma and nonadenoma subgroups at unenhanced CT. Pheochromocytoma and metastasis were higher in CT number than adenoma and hyperplasia at unenhanced CT.

Mean attenuation values (25th and 75th percentiles) on unenhanced CT. The box plots graphically illustrate the mean attenuation values of adenoma (Ade), pheochromocytoma (Phe), hyperplasia (Hyp), and metastasis (Met) on unenhanced CT. Adenoma is significantly lower in CT number than pheochromocytoma and hyperplasia (P<0.05) but is not significantly different from hyperplasia (P>0.05). Hyperplasia has two outliners in CT number (not shown)
The absolute PEWV of adenoma was significantly higher than that of pheochromocytoma and metastasis on DCE CT (P<0.05). Pheochromocytoma was significantly higher in PEWV than metastasis (P<0.05). Figure 2 graphically illustrates the comparison of absolute PEWVs between adenoma and nonadenoma subgroups including pheochromocytomas and metastasis at DCE CT. The descending order of absolute PEWVs of adenoma and nonadenoma subgroups was adenoma, pheochromocytoma, and metastasis.

Percentage enhancement washout values (PEWV) on delayed contrast-enhanced (DCE) CT. The box plots graphically illustrate PEWVs of adenoma (Ade), pheochromocytoma (Phe), and metastasis (Met) on DCE CT. Adenoma is significantly higher in PEWV than pheochromocytoma and metastasis (P<0.05). However, five pheochromocytomas had PEWVs of 60% or greater, similar to those of adenomas
Table 2 demonstrates the sensitivity, specificity, positive and negative predictive values, and accuracy of unenhanced CT and DCE CT for the diagnosis of adrenal adenoma using the mean attenuation value of 10 HU or less on unenhanced CT and absolute PEWV of greater than 60% on DCE CT. The sensitivity, specificity, and accuracy of unenhanced CT were 40%, 91%, and 66% while those of DCE CT were 96%, 61%, and 81%, respectively.
Four masses including three adrenal hyperplasias and one adrenal endothelial cyst were falsely diagnosed as adrenal adenoma on unenhanced CT (Fig. 3). The mean attenuation values of these lesions measured −8, 7.5, 8, and −1 HU, respectively. On DCE CT seven masses were falsely diagnosed as adrenal adenomas which included five pheochromocytomas, one oncocytic cortical tumor, and one primary pigmented nodular dysplasia (Fig. 4). The pheochromcytomas mimicking adenoma on DCE CT ranged from 62% to 82% (72.8±7.8) in absolute PEWV. The absolute PEWVs of the oncocytic cortical tumor and primary pigmented nodular dysplasia were 69.4% and 79.8%, respectively. Twenty-six masses including 25 lipid-poor adenomas and one degenerative adenoma were falsely diagnosed as nonadenomas on unenhanced CT. The degenerative adenoma which was diagnosed as nonadenoma on unenhanced CT was also misdiagnosed on DCE CT (Fig. 5).

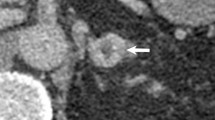
A 43-year-old man with macronodular adrenal hyperplasia. a The right adrenal mass (arrow) measured 8 HU in mean attenuation value on unenhanced CT. This lesion was a falsely diagnosed as lipid-rich adenoma before surgery. Left adrenal gland was not enlarged (not shown). b Microscopic examination demonstrates macronodular hyperplasia (asterisk) which do not show tumor capsule at the junction (arrows) between normal and hyperplastic tissue; hematoxylin-eosin, ×20. Several tiny small hyperplasic nodules (not shown) are found in the normal tissues although they are not seen by CT

A 48-year-old woman with pheochromocytoma. a–c The mean attenuation values of right adrenal mass (arrow) were 36, 173, and 70 HU on unenhanced, early contrast-enhanced, and delay contrast-enhanced CT, respectively. The PEWV of the lesion was calculated as 75.2%. This lesion was preoperatively diagnosed as lipid-poor adenoma on delayed contrast-enhanced CT but was pathologically confirmed as pheochromocytoma. d Microscopic examination confirmed the diagnosis of pheochromocytoma; hematoxylin-eosin staining, ×200. There were abundant capillaries (arrows) among nests of tumor cells, apparently related with rapid washout of contrast enhancement of the lesion on delayed contrast-enhanced CT

A 49-year-old woman with degenerated adenoma. a The mean attenuation value of left adrenal mass (arrow) was 55 HU on delayed contrast-enhanced CT while that on unenhanced and early contrast-enhanced CT was of the lesion is 29 HU and 59 HU, respectively. The PEWV of the lesion was calculated as 13%. This lesion was diagnosed as nonadenoma on delayed contrast-enhanced CT as well as on unenhanced CT. b Microscopic examination demonstrates old hemorrhage (H) surrounded by fibrous tissues (F) in the adenoma (A), indicating hemorrhagic degeneration, which probably occurred in the remote past; hematoxylin-eosin, ×100
Discussion
Intracytoplasmic lipid of adrenal adenoma is the primary cause of their low attenuation value on unenhanced CT [6]. For this reason several studies have reported that unenhanced CT can be a useful modality for characterization of incidentally detected adrenal masses [7–9]. However, considerable disagreement exists as to the precise cut off threshold to determine whether adrenal lesions are adenomas or nonadenomas. Boland et al. [1] showed that a threshold of 10 HU or less has a specificity of 98% but a sensitivity of 71% for adrenal adenoma. Lipid-poor adenomas with attenuation value of more than 10 HU account for 10–40% of adenomas and primarily reduce sensitivity for adenoma on unenhanced CT [1, 3, 4].
DCE CT has been reported to be helpful in distinguishing adenomas from nonadenomas with high sensitivity and specificity using more rapid washout property of adenomas than that of nonadenomas [2, 9, 10]. On DCE CT lipid-poor adenomas show enhancement characteristics nearly identical to those of lipid-rich adenomas and can be differentiated from nonadenomas with absolute PEWVs [3, 4]. Caoilli et al. [5] concluded from their study that the combination of unenhanced CT and DCE CT makes it possible to distinguish adenomas from nonadenomas mainly consisting of metastatic lesions with a sensitivity of 98% and a specificity of 92%.
In previous reports, however, a low proportion (5.7–37.8%) of adenomas were pathologically confirmed following surgery or percutaneous biopsy [2–5, 9, 10]. In most of cases the final diagnosis of adenoma was made by clinical or radiological findings on follow-up studies. Commonly used diagnostic criteria for adrenal adenoma include a mean attenuation value of 10 HU or less at unenhanced CT, absolute PEWV greater than 60% or relative PEWV greater than 40% at DCE CT and stability in size on a subsequent CT examination performed at least 6-months apart. Unlike in previous studies, our study included only pathologically confirmed cases.
Three of six cases with macronodular hyperplasias showed mean attenuation values of 10 HU or less on unenhanced CT and one of these lesions was biochemically hyperactive. Patients with ACTH-dependent Cushing syndrome or Conn's syndrome can manifest as macronodular adrenal hyperplasia [11–14]. However, no radiological study has reported whether these lesions can show as low an attenuation as lipid-rich adenomas on unenhanced CT. The pathological examinations in our study demonstrated that the adrenal hyperplastic nodule measuring 10 HU or less on noncontrast CT contains hyperplastic cells with abundant intracytoplasmic lipid but no capsule between normal and hyperplastic tissue. In addition to this nodule, multiple hyperplastic micronodules were found in the normal cortical tissue, all of which were not demonstrated by CT. One endothelial cyst also met CT criteria for adenoma on unenhanced CT, but the diagnosis was not difficult on contrast-enhanced CT as it was easily identified as a cystic lesion after intravenous administration of contrast material.
Lipid-poor adenomas were falsely diagnosed as nonadenomas on unenhanced CT in our study. However, as all of these lesions showed early washout of contrast enhancement on DCE CT, they could be correctly categorized as adenomas, which agrees with the description of the previous studies [1, 3, 4].
Szolar et al. [15] reported that in their study absolute PEWVs of pheochromocytoma were significantly lower than those of adenomas, and none of the pheochromocytomas were falsely diagnosed as adenoma. In our study, however, five of 31 pheochromocytomas (16%) showed absolute PEWVs of greater than 60% on DCE CT. Pheochromocytoma proved to be the most common mimicker of adenoma on DCE CT. On pathological examination these pheochromocytomas with high absolute PEWVs were hypervascular than other pheochromocytomas with low absolute PEWVs. In addition, Caoili et al. [5] also reported in their series that a pheochromocytoma was one of mimickers of adenoma on DCE CT. Although most pheochromocytomas are clinically diagnosed prior to surgery because they are biochemically active, 9% of incidentally detected adrenal masses were reported to be pheochromocytoma and needed to be differentiated from adenomas [16]. All of five pheochromocytomas with absolute PEWV of greater than 60% on DCT increased in amount of urine or plasma catecholamine. However, one pheochromocytoma of these lesions was clinically asymptomatic and thus was incidentally detected on abdominal CT.
Other mimickers in our study include one oncocytic cortical tumor and one primary pigmented nodular adrenocortical dysplasia, both of which also pathologically revealed hypervascularity. Adrenal metastasis from renal cell carcinomas can be a mimicker of adenoma at DCE CT because it tends to have a rapid loss of attenuation soon after enhancement with intravenous contrast material [5].
Our study has several limitations. First, it was carried out retrospectively in pathologically confirmed adrenal masses. Case selection bias can occur because all cases included in this study were indicated for surgical intervention. However, this study may overcome critical limitations of previous studies in which the diagnosis of adenoma was not histologically confirmed in many cases, and no long-term follow-up CT was performed. One adrenal mass in a patient who underwent nephrectomy for renal cell carcinoma grew to double the volume on the original CT performed 1 year earlier. The lesion was surgically removed to rule out metastasis although it had an absolute PEWV of greater than 60% but was histologically confirmed as adenoma. This case suggests that in rare incidences the adrenal adenoma can increase in size at the follow-up examination, which is supported by the findings of Baron et al. [17]. Second, measurement of CT number in the small lesions could have caused partial volume averaging errors. To minimize this error ROI was not placed in the peripheral area of the lesion. Third, only less than a one-half the adrenal masses were evaluated with both unenhanced and DCE CT. For further investigation of the role of DCE CT a well-designed prospective study with a large number of cases may be needed in the future. Fourth, this study has quite a high incidence of pheochromocytomas in our nonadenoma group relative to metastasis. All the previous studies have a substantially higher incidence of metastasis relative to pheochromocytomas [2–6, 10]. The true incidence of pheochromocytomas is not so high as that of adrenal metastasis in the general population [16].
In conclusion, diagnostic accuracy for adenoma on unenhanced and DCE CT scan is not as high as that reported by previous studies when pathological correlation is performed. Diagnosing adenoma only on CT characteristics/values can lead to misdiagnosis. In our study, the lower specificity than expected was due to pheochromocytomas presenting as false positives. The diagnostic performance is improved if biochemical findings are taken into account.
References
Boland GW, Lee MJ, Gazelle GS, Halpern EF, McNicholas MM, Mueller PR (1998) Characterization of adrenal masses using unenhanced CT: an analysis of the CT literature. AJR Am J Roentgenol 171:201–204
Korobkin M, Brodeur FJ, Francis IR, Quint LE, Dunnick NR, Londy F (1998) CT time-attenuation washout curves of adrenal adenomas and nonadenomas. AJR Am J Roentgenol 170:747–752
Caoili EM, Korobkin M, Francis IR, Cohan RH, Dunnick NR (2000) Delayed enhanced CT of lipid-poor adrenal adenomas. AJR Am J Roentgenol 175:1411–1415
Pena CS, Boland GW, Hahn PF, Lee MJ, Mueller PR (2000) Characterization of indeterminate (lipid-poor) adrenal masses: use of washout characteristics at contrast-enhanced CT. Radiology 217:798–802
Caoili EM, Korobkin M, Francis IR, Cohan RH, Platt JF, Dunnick NR, Raghupathi KI (2002) Adrenal masses: characterization with combined unenhanced and delayed enhanced CT. Radiology 222:629–633
Korobkin M, Giordano TJ, Brodeur FJ, Francis IR, Siegelman ES, Quint LE, Dunnick NR, Heiken JP, Wang HH (1996) Adrenal adenomas: relationship between histologic lipid and CT and MR findings. Radiology 200:743–747
van Erkel AR, van Gils AP, Lequin M, Kruitwagen C, Bloem JL, Falke TH (1994) CT and MR distinction of adenomas and nonadenomas of the adrenal gland. J Comput Assist Tomogr 18:432–438
McNicholas MM, Lee MJ, Mayo-Smith WW, Hahn PF, Boland GW, Mueller PR (1995) An imaging algorithm for the differential diagnosis of adrenal adenomas and metastases. AJR Am J Roentgenol 165:1453–1459
Boland GW, Hahn PF, Pena C, Mueller PR (1997) Adrenal masses: characterization with delayed contrast-enhanced CT. Radiology 202:693–696
Szolar DH, Kammerhuber FH (1998) Adrenal adenomas and nonadenomas: assessment of washout at delayed contrast-enhanced CT. Radiology 207:369–375
Sohaib SA, Hanson JA, Newell-Price JD, Trainer PJ, Monson JP, Grossman AB, Besser GM, Reznek RH (1999) CT appearance of the adrenal glands in adrenocorticotrophic hormone-dependent Cushing's syndrome. AJR Am J Roentgenol 172:997–1002
Imaki T, Naruse M, Takano K (2004) Adrenocortical hyperplasia associated with ACTH-dependent Cushing's syndrome: comparison of the size of adrenal glands with clinical and endocrinological data. Endocr J 51:89–95
Lingam RK, Sohaib SA, Vlahos I, Rockall AG, Isidori AM, Monson JP, Grossman A, Reznek RH (2003) CT of primary hyperaldosteronism (Conn's syndrome): the value of measuring the adrenal gland. AJR Am J Roentgenol 181:843–849
Lingam RK, Sohaib SA, Rockall AG, Isidori AM, Chew S, Monson JP, Grossman A, Besser GM, Reznek RH (2004) Diagnostic performance of CT versus MR in detecting aldosterone-producing adenoma in primary hyperaldosteronism (Conn's syndrome). Eur Radiol 14:1787–1792
Szolar DH, Korobkin M, Reittner P, Berghold A, Bauernhofer T, Trummer H, Schoellnast H, Preidler KW, Samonigg H (2005) Adrenocortical carcinomas and adrenal pheochromocytomas: mass and enhancement loss evaluation at delayed contrast-enhanced CT. Radiology 234:479–485
Cook DM, Loriaux DL (1996) The incidental adrenal mass. Am J Med 101:88–94
Barzon L, Scaroni C, Sonino N, Fallo F, Paoletta A, Boscaro M (1999) Risk factors and long-term follow-up of adrenal incidentalomas. J Clin Endocrinol Metab 84:520–526
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s00330-005-0065-5
Rights and permissions
About this article
Cite this article
Park, B.K., Kim, B., Ko, K. et al. Adrenal masses falsely diagnosed as adenomas on unenhanced and delayed contrast-enhanced computed tomography: Pathological correlation. Eur Radiol 16, 642–647 (2006). https://doi.org/10.1007/s00330-005-0017-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-005-0017-0