
Abstract
The purpose of this study was to demonstrate the macroscopic and MRI anatomy of the fasciculus obliquus, otherwise known as the ligamentum glenohumerale spirale or spiral GHL of the anterior shoulder joint capsule. Conventional and MR arthrography (1.5-T device Somatom Symphony, Siemens with shoulder coil) images in standard planes were compared with gross anatomic dissection findings in six fresh shoulder specimens from three cadavers. The MR imaging protocol included T1, PD and DESS 3D WI sequences. The macroscopically recognisable band—the spiral GHL—was identified by anatomic dissection and MRI in all the specimens. It was best visualised by MR arthrography on axial and oblique sagittal planes (T1; PD WI) and appeared as a low signal intensity stripe within the superficial layer of the anterior joint capsule. The absence of the variable middle glenohumeral ligament did not influence the anatomic properties and the MR imaging of the spiral GHL. Diagnostic visualisation of the normal anatomic structures is a prerequisite to distinguish between normal and pathologic conditions. Anatomy of the spiral GHL can be used by radiologists for more detailed interpretation of the anterior shoulder joint capsule ligaments on MR images.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Anterior shoulder instability is a common clinical problem in orthopaedic practice. Since an aim of the orthopaedic operation is to restore the anatomy of the joint or to reinforce the injured joint structures, a preliminary detailed anatomy-based diagnosis is required [1–8].
In the official Terminologia Anatomica, the three ligaments of the anterior shoulder joint capsule are mentioned together as Ligg. glenohumeralia [9]. As such, contemporary anatomy textbooks and atlases do not demonstrate the detailed anatomy of these ligaments [10–12].
In the clinical literature, the three anterior capsular ligaments classically have been described as the superior, middle and inferior glenohumeral ligaments (SGHL, MGHL and IGHL) [13]. The IGHL has been divided into three parts—an anterior band, a posterior band and an interposed axillary pouch [14]. In addition to the SGHL, MGHL and IGHL, a bundle of fibres historically called the fasciculus obliquus or “longitudinal oblique system” has been described in the superficial layer of the anterior shoulder joint capsule [15–17].
A recent anatomic study on embalmed shoulder joints revealed more detailed anatomy of the fasciculus obliquus that made it possible to recognise it as a distinct anterior capsular ligament. Because of its macroscopic appearance during external rotation and abduction, it was named the Ligg. glenohumerale spirale (Fig. 1). Despite the tight connection with the MGHL and IGHL, its significance in the shoulder joint biomechanics and involvement in different pathologic conditions has not been investigated [18].

Schematic drawing of the anterior capsular ligaments. H humerus, PC processus coracoideus, SC scapula, SGHL superior glenohumeral ligament, MGHL middle glenohumeral ligament, IGHL inferior glenohumeral ligament with projection of the anterior band; spiral GHL spiral glenohumeral ligament (fasciculus obliquus)
MR imaging has proved to be a valuable method in identifying the normal anatomy of the shoulder joint and in the diagnostic evaluation of labrum and glenohumeral ligaments [19–24]. The aim of this study was to repeat the previous anatomic dissections on fresh shoulder joint specimens and to attempt to visualise the fasciculus obliquus, or Ligg. glenohumerale spirale (spiral GHL), on conventional and contrast-enhanced MR images.
Material and methods
Six fresh shoulder joints (three right and three left) from three cadavers (two male and one female; ages 73, 81 and 91 years) were investigated by MR imaging and subsequent gross anatomic dissection.
MR imaging of the shoulder specimens
Shoulder specimens were examined by MRI on a 1.5 Tesla device [Somatom Symphony (R), Siemens, Erlangen, Germany]. The shoulder coil was used in all cases. Three shoulders were investigated without contrast medium. MR arthrography was performed on all the six shoulder specimens. The MR arthrography was done under fluoroscopic control with injection of 15–20 ml of a contrast solution (1 ml of Omniscan in 100 ml of saline). We used standard axial, oblique sagittal and oblique coronal fat saturated views PDW WI [TR 3,000 ms, TE 36 ms, SL 3 mm, Matrix (M) 224×512, number of acquisitions (NA) 2, TA (min) axial 3.18, oblique sagittal/coronal 3.54], axial and oblique sagittal T1 W1 [TR 632 ms, TE 14 ms, SL 3 mm, M 256×512, NA 3, TA (min) axial 4.32, oblique sagittal 3.46] and DESS 3D W1 [TR 21.5 ms, TE 6.5 ms, SL 1.5 mm, M 217×256, NA 1, TA (min) 5.14].
Gross anatomic dissection
After MRI examination, the soft tissues, clavicle and shoulder girdle muscles were removed from the shoulder specimens. The extra-articular part of the long head biceps tendon within the intertubercular groove was preserved. The acromion was separated from the scapular spine and turned anteriorly together with the acromioclavicular ligament. Muscles and tendons of the rotator cuff were cleaned from the rests of the subacromial bursa and separated from the joint capsule. The ligaments of the anterior joint capsule were identified by fine dissection according to the direction of the bundles of collagen fibres. The subscapularis bursa was opened to visualise the glenoid labrum and its relation to the capsular ligaments. To avoid confusing recognition of capsular folds as ligaments, the anatomically identified structures were examined through the total range of shoulder joint motions.
Comparison of the MR images with gross anatomic specimens
On MR images we specifically evaluated the MGHL, the spiral GHL and the anterior band as well as the axillary part of the IGHL complex. Because of the separate position of the SGHL and posterior band of the IGHL complex from the spiral GHL, these structures were not evaluated in MR images and during gross anatomic dissection of the shoulder joints.
Since the spiral GHL has not been previously described in the radiology literature, two experienced specialists in musculoskeletal radiology read the first two MR images after they saw the cadaver specimens and learned the pertinent anatomy. Having become familiar with the expected location of the spiral GHL, the remaining four shoulder MR images were interpreted prior to the anatomic dissection. Different evaluations were resolved by consensus.
Results
Gross anatomic dissection
The glenohumeral ligaments of the anterior shoulder joint capsule were clearly recognisable structures (Figs. 2d–f, 3c). The spiral GHL was present in all the six dissected shoulder joint specimens. It arose from the region of the infraglenoid tubercle and the long head of the triceps muscle as a separate band (Fig. 2e,f). The ligament coursed cranially in the superficial layer of the anterior shoulder joint capsule, crossing and fusing with the underlying IGHL. After establishing a tight connection with the MGHL, it fused with the postero-cranial surface of the subscapularis tendon. The ligament and the tendon inserted together on the lesser tubercle of the humerus (Figs. 2d,e, 3c). The spiral appearance of the oblique, ascending capsular ligament was clearly visible with the humerus in abduction and external rotation (Fig. 2e).

a–c MR arthrograms of a left shoulder with MGHL. PD-WI fat-saturated (fs); TR/TE=3,000/36 ms. a Oblique coronal image shows the MGHL (black arrow), an anterior capsular folding corresponding to the location of the spiral GHL (white arrow) and the axillary part of the IGHL (dotted white arrow). b,c Subsequent oblique sagittal images show anterosuperior labrum (dotted black arrow), the MGHL (black arrow), the anterior capsular section with spiral GHL (white arrow) and the anterior band of the IGHL (dotted white arrow). d–f Photograph of an anatomic dissection of a left shoulder specimen with MGHL. d, e The MGHL (black arrow) and visible capsular thickening—the spiral GHL (white arrow)—fuse with the anterior capsule, which has been separated from the subscapularis muscle (SSC). The IGHL (dotted white arrows) pass deep to the spiral GHL. A normal variation of the anterosuperior labrum (dotted black arrow) with sublabral foramen (asterisk) is noted. e In abduction and external rotation, the anterior capsular structures come under tension. The course of the spiral GHL and its fusion with MGHL is clearly demonstrated. f Photograph of an axillary view of a right shoulder specimen in abduction demonstrates the spiral GHL (white arrow) origin from the infraglenoid tubercle and its superficial course over the taut IGHL (dotted white arrows). PC processus coracoideus, CH caput humeri, SSC subscapularis muscle, SC scapula, H humerus, IT infraglenoid tubercle, TB tendon of the triceps brachii muscle

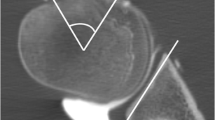
MR arthrograms of a left shoulder without MGHL. a Oblique sagittal PD-WI; fs; TR/TE=3,000/36 MR arthrogram of a left shoulder demonstrates the anterior band of the IGHL (dotted white arrow) in the deep layer and the spiral GHL (white arrow) in the superficial layer of the shoulder joint capsule. b Axial T1-WI; fs; TR/TE=632/14 ms scan—the spiral GHL runs perpendicular to the plane of imaging and is seen as a low signal intensity stripe (white arrow) within the anterior capsule. The MGHL is absent on both images. c Photograph of a right shoulder specimen without the MGHL. The IGHL complex (dotted white arrows) is visible together with the spiral GHL (white arrow). PC processus coracoideus, CH caput humeri, SSC subscapularis muscle, SC scapula, H humerus, IT infraglenoid tubercle, TB tendon of the triceps brachii muscle
The MGHL originated from the superior neck of scapula and was connected to the antero-superior labrum. It coursed in a caudal direction under the subscapularis tendon and crossed with the ascending fibres of the spiral GHL. With the humerus in abduction and external rotation, the spiral GHL tensed and turned the MGHL from the vertical to a nearly horizontal position (Fig. 2d,e). After the crossing with the spiral GHL, the MGHL fused with the lateral joint capsule, and its course towards the lesser tubercle of the humerus was not clearly detectable macroscopically. The MGHL was absent in two glenohumeral joints. The absence of the MGHL in two glenohumeral specimens did not influence the anatomic position or the main course of fibres of the spiral GHL (Fig. 3c).
The IGHL complex was present in all the six investigated shoulders. It originated from the antero-inferior neck of the scapula, coursed under the spiral GHL in the latero-caudal direction and inserted on the anatomic neck of the humerus. The anterior thickening of the IGHL complex was not recognisable on the extra-articular side of the joint capsule (Figs. 2d–f, 3c).
In addition, we observed the sublabral foramen as a complete separation between the antero-superior labrum and the underlying glenoid rim in two specimens. Its anatomical appearance depended on the position of the MGHL (Fig. 2d,e).
MRI findings
The ligaments of the anterior shoulder joint capsule were best seen on axial (T1 WI, PDW WI, DESS) and oblique sagittal (T1 WI and PDW WI) oriented images after MR arthrography (Figs. 2b,c, 3a,b). In one of six shoulders, the oblique coronal sections were useful for detecting MGHL and spiral GHL (Fig. 2a).
The spiral GHL was detectable as a low signal intensity stripe on MR images along its course within the anterior joint capsule in all the six specimens (Figs. 2a–c, 3a,b). The ligament could not be detected in two of three shoulder MR images without arthrography.
The MGHL was absent on MR images in two shoulder specimens. This was confirmed during the anatomic dissections.
The IGHL was seen on all MR arthrograms as a continuous low signal intensity band with an origin on the anterior and inferior parts of the scapular neck and an insertion on the neck of humerus. On the oblique sagittal plane images, the anterior band of the IGHL complex became clearly recognisable (Figs. 2b,c, 3a).
Discussion
The results of the present investigation confirm the existence of an additional glenohumeral ligament within the superficial layer of the anterior shoulder joint capsule. Its oblique course through the midline of the anterior joint capsule was recognisable in all the investigated fresh cadaver shoulder joint specimens and on MR images with arthrography.
A superficial oblique course of collagen fibres within the superficial layer of the anterior shoulder joint capsule, the fasciculus obliquus, was first described by Delorme in 1910. This finding was confirmed by Landsmeer and Meyers in 1959. According to their description, the inferior superficial capsular layer formed a bundle of fibres that was recognised as a part of the M. subscapularis fascia. This fasciculus obliquus intermingled cranio-laterally with the MGHL and the subscapularis tendon, lost its macroscopic appearance and fused with the superior part of the anterior joint capsule. Later anatomic investigations have confirmed the existence of the fasciculus obliquus with no additional gross anatomic description of this capsular structure [13, 17, 25].
Our findings on six fresh shoulder joint specimens support the previous, more detailed macroscopic description that rediscovered the existence of the oblique capsular fibres in the form of a separate ligament—the Ligg. glenohumerale spirale [18]. The spiral GHL originates from the infraglenoid tubercle and the long head triceps tendon and is tightly connected with the IGHL and MGHL. Cranially, it fuses with the subscapularis tendon and inserts together with it on the lesser tubercle of the humerus, which has not been found in the previous investigations describing the fasciculus obliquus of the anterior shoulder joint capsule [15, 16].
The anatomic knowledge of the existence of the spiral GHL and its connection with the MGHL could be used during the interpretation of the MR images. Because the fibres of the spiral and MGHL ligaments are close to the oblique coronal plane, the partial volume effect within the anterior joint capsule interferes with visualisation of these ligaments. Despite this, these structures can be identified on oblique coronal images (Fig. 2a). In the oblique sagittal plane, a nearly vertical position of the spiral GHL and the MGHL is visualised as one or two low signal intensity vertical stripes (Fig. 2b,c). In those cases when the MGHL exists, one could follow its course to identify the spiral GHL at the point of fusion (Fig. 2b). However, the MGHL can be absent in 12–27% of cases [26–28]. In our series, it was not found in two of six specimens (both shoulders in one cadaver), which confirms the previous results concerning the variability of the MGHL. When the MGHL is absent, the low signal intensity stripe of the spiral GHL is detectable on the posterior, articular side of the subscapularis muscle (Fig. 3a). The clear visualisation of the spiral GHL on axial MR images might be explained with the cross-sectional view of the separate anatomic structure (Fig. 3b).
The anatomic and MRI appearance of the IGHL complex and the absence of the anterior band on the extra-articular side of the shoulder joint capsule (Figs. 2c–f, 3c) are consistent with previous anatomic findings [14, 18, 27] and MR arthrography results [20, 21, 23].
Direct MR arthrography has proven to be a useful method in the evaluation of the normal anatomy as well as pathologies of the shoulder joint [22, 23, 29–31]. The enhanced soft tissue contrast and controlled distension of the joint cavity provides better delineation and assessment of the glenohumeral intra-articular structures. Our results support the positive experience of the previous studies. Without injection of the contrast medium, the spiral GHL could be recognised only in one of the three shoulder joints.
The small number and old age of the investigated shoulder specimens limited the present study. We obtained the MR images with the shoulder in the neutral position, but the anatomic dissection showed that the spiral GHL is the best visualised with the shoulder in abduction and external rotation. Therefore, MR imaging of the spiral GHL may be improved if the shoulder is placed within the coil with the spiral GHL in the tensioned position.
The macroscopic appearance of the spiral GHL and its tension during abduction and external rotation suggests that its role in shoulder joint function might be underestimated. During motion, the spiral GHL influences the position of the MGHL that plays an important role in maintaining the shoulder joint stability. As the diagnostic visualisation of the normal anatomic structures is a prerequisite to distinguish between normal and pathologic conditions, MRI anatomy of the spiral GHL can be used by the radiologist for more detailed interpretation of the anterior shoulder joint capsule ligaments on MR images.
References
Bankart ASB (1938) The pathology and treatment of recurrent dislocation of the shoulder-joint. Br J Surg 26:23–29
Rowe CR, Patel D, Southmayd WW (1978) The Bankart procedure. A long-term end-result study. J Bone Joint Surg (Am) 60:1–16
Jobe FW, Giangarra CE, Kvitne RS, Glousman RE (1991) Anterior capsulolabral reconstruction of the shoulder in athletes in overhand sports. Am J Sport Med 19:428–434
Wirth MA, Blatter G, Rockwood Jr. CA (1996) The capsular imbrication procedure for recurrent anterior instability of the shoulder. J Bone Joint Surg (Am) 78:246–259
Cole BJ, Warner, JJP (2000) Arthroscopic versus open Bankart repair for traumatic anterior shoulder instability. Clin Sports Med 19:19–48
Gartsman GM, Roddey TS, Hammerman SM (2000) Arthroscopic treatment of anterior-inferior glenohumeral instability. Two to five-year follow-up. J Bone Joint Surg (Am) 82:991–1003
Weiss KS, Savoie FH III (2002) Recent advances in arthroscopic repair of traumatic anterior glenohumeral instability. Clin Orthop 400:117–122
Pagnani MJ, Dome DC (2002) Surgical treatment of traumatic anterior shoulder instability in American football players. J Bone Joint Surg (Am) 84:711–715
Terminologia Anatomica (1998) Thieme, Stuttgart
Agur AMR (1991) Grant’s atlas of anatomy, 9th edn. Williams & Wilkins, Baltimore
Moore LM (1992) Clinically oriented anatomy. Williams & Wilkins, Baltimore
Tillmann B, Töndury G (1987) Obere Extremität. In: Leonhardt H, Tillmann B, Töndury G, Zilles K (eds) Rauber/Kopsch: Lehrbuch und Atlas der Anatomie des Menschen. Bd 1, Bewegungsapparat. Thieme, Stuttgart
Moseley HF, Övergaard B (1962) The anterior capsular mechanism in recurrent anterior dislocation of the shoulder. J Bone Joint Surg (Br) 44:913–927
O’Brien SJ, Neves MC, Arnoczky SP, Rozbruk SR, Dicarlo EF, Warren RF, Schwartz R, Wickiewicz TL (1990) The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. Am J Sport Med 18:449–456
Delorme (1910) Die Hemmungsbänder des Schultergelenks und ihre Bedeutung für die Schulterluxationen. Arch Klin Chir 92:79–101
Landsmeer JMF, Meyers KAE (1959) The shoulder region exposed by anatomical dissection. Arch Chir Neerlandicum 11:274–296
Gohlke F (1994) The pattern of the collagen fiber bundles of the capsule of the glenohumeral joint. J Shoulder Elbow Surg 3:111–128
Kolts I, Busch LC, Tomusk H, Rajavee E, Eller A, Russlies M, Kühnel W (2001) Anatomical composition of the anterior shoulder joint capsule. A cadaver study on 12 glenohumeral joints. Ann Anat 183:53–59
Flannigan B, Kursunoglu-Brahme S, Snyder S, Karzel R, Del Pizzo W, Resnick D (1990) MR arthrography of the shoulder: comparison with conventional MR imaging. Am J Roentgenol 155:829–832
Palmer WE, Brown JH, Rosenthal DI (1994) Labral-ligamentous complex of the shoulder: evaluation with MR arthrography. Radiology 190:645–651
Chandnani VP, Gagliardi JA, Murnane TG, Bradley YS, DeBerardino TA, Spaeth J, Hansen MF (1995) Glenohumeral ligaments and shoulder capsular mechanism: evaluation with MR arthrography. Radiology 196:27–32
Zanetti M, Carstensen T, Weishaupt D, Jost B, Hodler J (2001) MR arthrographic variability of the arthroscopically normal glenoid labrum: qualitative and quantitative assessment. Eur Radiol 4:559–566
Yeh L, Kwak S, Kim YS, Pedowitz R, Trudell D, Muhle C, Resnick D (1998) Anterior labroligamentous structures of the glenohumeral joint: correlation of the MR arthrography and anatomic dissection in cadavers. Am J Roentgenol 171:1229–1236
Vahlensieck M (2000) MRI of the shoulder. Eur Radiol 10:242–249
Turkel SJ, Panio MW, Marshall JL Girgis FG (1981) Stabilizing mechanisms preventing anterior dislocation of the glenohumeral joint. J Bone Joint Surg (Am) 63:1208–1217
DePalma AF, Gallery G, Bennet GA (1949) Variational anatomy and degenerative lesions of the shoulder joint. Instr Course Lect 6:255–281
Steinbeck J, Liljenqvist U, Jerosch J (1998) The anatomy of the glenohumeral ligamentous complex and its contribution to anterior shoulder stability. J Shoulder Elbow Surg 7:122–126
O’Brien SJ, Warren RF, Schwartz E (1987) Anterior shoulder instability. Orthop Clin North Am 18:395–408
Connell D, Padmanabhan R, Buchbinder R (2002) Adhesive capsulitis: role of MR imaging in differential diagnosis. Eur Radiol 12:2100–2106
Blum A, Coudane H, Mole D (2000) Gleno-humeral instabilities. Eur Radiol 10:63–82
Beltran J, Bencardino J, Mellado J, Rosenberg ZS, Irish RD (1997) MR arthrography of the shoulder: variants and pitfalls. RadioGraphics 17:1403–1412
Acknowledgements
This work is part of the project supported by the Estonian Science Foundation Grants No 5210 and 4367. The authors wish to thank Mr. Agu Raudheiding from the Institute of Anatomy of the University of Tartu for valuable technical assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Merila, M., Leibecke, T., Gehl, HB. et al. The anterior glenohumeral joint capsule: macroscopic and MRI anatomy of the fasciculus obliquus or so-called ligamentum glenohumerale spirale . Eur Radiol 14, 1421–1426 (2004). https://doi.org/10.1007/s00330-004-2296-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-004-2296-2