
Abstract
The purpose of the present study was to assess incidence, fracture type, and location of spine fractures due to falls. All emergency room CT requests during a time period of 26 months were reviewed retrospectively. Patients who had fallen or jumped and were initially examined with multidetector CT (MDCT) were included. The MDCT studies were evaluated by two radiologists for trauma location, fracture type, and multiple level involvement. A total of 237 patients (184 males, 53 female, age range 16–86 years, mean age 42 years) met the inclusion criteria. A total of 203 vertebral fractures were seen in 127 patients. Burst fracture (n=78) was the most frequent type of trauma, usually located in the thoracolumbar junction (50%). Also, compression fracture (n=52) was most common in the thoracolumbar junction (39%). Posterior column fracture (n=52) was most frequently detected in the cervical spine (40%). Multiple-level spine fractures were seen in 41 (32%) of the injured patients, of which 12 (29%) had fractures at noncontinuous levels. With increasing height the overall incidence of fractures increased, and burst fractures and multiple level spine fractures became more frequent. Age had no effect on fracture type or location. Spine fractures due to falls are common. Burst fracture is the most common fracture type and most frequently seen in the thoracolumbar junction. Multiple-level fractures were seen in 32% of the cases, of which 29% were seen at noncontinuous levels. Serious spine fractures are seen in all falling height and age groups.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Spine injuries are potentially dangerous and may cause permanent damage or even death [1, 2]. They are frequently seen in level-one trauma center patients with serious accidents such as traffic, falling, and sports accidents [2, 3, 4, 5, 6]. The annual incidence of spinal cord injuries is approximately 15–40 per million with a male predominance (80–85%), with two-thirds of spinal cord injuries occurring in patients less than 30 years of age [4]. More than 50% of patients with a spinal cord injury die prior to hospitalization [4]. The higher the level of injury in the cervical spine, the higher is the pre- and in-hospital mortality. The diagnosis of spine fractures is based on clinical examination and radiological findings [3, 7]. In emergency imaging, CT has replaced conventional radiography as the primary imaging modality of severely traumatized patients due to its higher diagnostic accuracy and cost-effectiveness [2, 8, 9, 10], although conventional radiography has been reported to be sufficient in conscious, non-intoxicated patients without clinical symptoms of spinal injury [3].
In level-one trauma centers CT is routinely used for screening seriously injured patients [2, 11, 12], although conventional radiography has been reported sufficient in conscious, non-intoxicated patients without clinical symptoms of spinal injury [3]. Due to technical breakthroughs, multidetector CT (MDCT) is faster and has better temporal, spatial, and contrast resolution due to smaller isotropic voxels compared with conventional helical CT [13]. Also, the two-dimensional (2D) reformats (multiplanar reconstructions, MPR) and three-dimensional (3D) surface renderings, although 3D surface renderings are rarely used for interpretation because they are time-consuming and provide only occasionally additional information [14], are of excellent quality, and due to the fast image processing, they can be made almost on-line; therefore, where available, MDCT has become the imaging method of choice in severe emergency trauma.
Due to more effective and successful first aid during the “golden hour” on the trauma site and during the transportation to hospital, the number of more seriously injured trauma patients surviving at least until admission to the emergency room has increased during the past 60 years, being almost three times as high in the 1980s (50 per million) than in the 1940s (17 per million) [4]; therefore, to be able to detect an injury and recommend the appropriate imaging modality, it is imperative for the radiologist-on-call to know the most common locations and injury patterns of spine fractures in different types of trauma, such as falling accidents. The purpose of the present study was to assess the acute phase MDCT spine findings in patients referred to a level-one trauma center due to a falling accident.
Materials and methods
This retrospective study took place in Töölö Hospital Trauma Center, Helsinki, Finland. It is the only level-one trauma center for a population of 1.4 million people. Also, the most difficult orthopedic and neurosurgical trauma patients are submitted to this hospital from other parts of Finland.
Using picture archiving and communications system (PACS), we retrieved all emergency room CT requests since the installation of the MDCT in August 2000 to the end of September 2002. A total of 4812 MDCT examinations were performed during these 26 months by the request of the emergency room physicians. All patients with a falling accident fulfilling the emergency room triage criteria and whose spine was initially examined with MDCT were included in this study. Pediatric patients, usually under the age of 16 years, were not included as they are generally taken to the Children’s Hospital.
All patients underwent routine cervical and body MDCT on a four-section multi-slice scanner (LightSpeed QX/i, GE Medical Systems, Milwaukee, Wis.). For the cervical spine, the high-resolution scanning parameters were as follows: 4×1.25-mm collimation; gantry rotation time 1.0 s; pitch 3; table feed 3.75 mm; 120/140 kV (upper/lower part of the c-spine); 280/330 mA; and approximate total exposure time 35 s. In sagittal and coronal MPR slice thickness was 1.5 mm and reconstruction increment 1.5 mm. Routine body MDCT with intravenous contrast agent was as follows: 4×2.5 mm collimation; gantry rotation time 0.8 s; pitch 6; table feed 15 mm; 140 kV; 280/330 mA (thorax/abdomen); and approximate total exposure time 30 s. Also, MPR of the spine was done in sagittal and coronal planes routinely with 2.5-mm slice thickness and 2.5-mm reconstruction increment.
Two radiologists interpreted MDCT studies by consensus. The studies were evaluated by trauma location, fracture type, and whether the fractures were at multiple levels. The spine was divided into four functional units: (a) C0 to Th1 (cervical spine); (b) Th2 to Th11 (thoracic spine); (c) Th12 to L1 (thoracolumbar junction); and (d) L2 to S1 (lumbar spine). The fracture types were also divided into four categories: (a) burst fracture [15]; (b) compression fracture [15]; (c) posterior column fracture [15]; and (d) other fractures. Falling height and whether the subject had jumped or accidentally fallen was retrieved from each patient’s file.
Results
We found 237 patients (184 males, 78%; 53 females, 22%; age range 16–86 years, mean age 42 years) who met the inclusion criteria. A total of 211 patients (89%) had fallen accidentally, 19 (8%) had jumped, and in 7 cases (3%) the circumstances were unclear. A total of 203 vertebral fractures (Fig. 1) were seen in 127 patients (54%), of which 71 (56%) required surgical treatment. Multiple-level spine fractures were seen in 41 patients (32%), of which 22 (54%) required surgical treatment. In 12 of the 41 patients (29%) the fractures were seen at noncontinuous levels. In 110 patients (46%) the initial MDCT of the spine was normal.

Distribution of fractures in a the cervical spine and b the thoracolumbar spine. The numbers next to the vertebral bodies represent the absolute number of fractures
Burst fracture (n=78, 38%; Fig. 2) was the most common fracture type and was most frequently seen in the thoracolumbar junction (n=39, 50%), whereas only 10% (n=8) of burst fractures were seen in the cervical spine (Table 1). Seventy-one (56%) of the 127 injured patients had one or more burst fractures.

Burst fracture of L1 in a 40-year-old man. a Axial and b sagittal view with typical retropulsed fragment. Anterior and middle columns are fractured, the posterior column remains intact
Compression fracture (n=52, 26%; Fig. 3) was also most commonly seen in the thoracolumbar junction (n=20, 39%), and least commonly in the cervical spine (n=1, 2%). Posterior column fracture (n=52, 26%; Fig. 4), on the other hand, was most frequently detected in the cervical spine (n=21, 40%), and was least common in the thoracolumbar junction (n=2, 4%; Table 1).

Compression fracture of Th11 in a 31-year-old man. a Axial view shows the left anterior compression with fracture lines (arrowheads). b Sagittal view. The anterior column is fractured, resulting in a wedge-shaped vertebral body. c Coronal view reveals lateral compression (arrow)

Isolated fracture of the spinous process of CII in a 50-year-old man. a Axial and b sagittal views demonstrate the fracture line (arrows)
Other fractures (n=21, 10%) occurred almost exclusively in the cervical spine (n=19, 91%); ten fracture dislocations (48%), one extension teardrop fracture (5%), one type-II odontoid process fracture (5%), one atlanto-occipital dissociation (5%), one isolated anterior longitudinal ligament rupture (5%), fracture of C1 lateral mass in 2 patients (10%) and three bamboo spine fractures (14%) in 2 patients with ankylosing spondylitis. In addition, there was one Chance fracture (5%) in Th11, and one linear fracture (sagittal split; 5%) in L2 (Table 1). Nineteen (90%) of the 21 other fractures were considered unstable.
The mean falling height (6.2 m) of patients who had jumped was higher than in patients who had accidentally fallen (3.7 m). Spine fractures, however, did not appear to occur more frequently. There seemed to be no difference in fracture type or location between patients who had jumped or fallen. The limited number of patients who had jumped, however, does not allow statistical comparison.
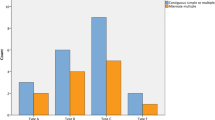
With increasing height the overall incidence of fractures increased (p=0.0182, confidential interval (CI)=5.21–20.15, simple linear regression) and burst fractures became more frequent (Table 2). In contrast, posterior column and other fractures decreased, whereas the proportion of compression fractures was constant. As the falling height increased, the proportion of thoracic spine fractures also increased (Table 2). This tendency was not observed in the thoracolumbar junction and lumbar spine fractures. The cervical fractures appeared to become less frequent as the falling height increased, and the proportion of normal cervical examinations increased. Multiple-level spine fractures occurred more frequently with increasing height (Table 2).
The ratio between patients with and without spine fractures seemed to be neither dependent on height nor on age (Table 2, 3). Falling height was reciprocally proportional to age, but the incidence of spine fractures did not decrease with age (p=0.0328, CI=−197.23 to −16.51, simple linear regression; Table 3). The proportion of posterior column fractures increased with age, but burst and compression fractures as well as the other fracture types and multiple-level fractures occurred independently of age (Table 3). Also, age had no effect on the fracture location, type, or on the amount of normal examinations (Table 3).
Discussion
Severe falling accidents are relatively common. During the 26-month period covered by this study, a total of 237 patients were taken initially to our hospital after falling accidents, which means such an accident every third day on average. In our hospital, if a patient has had a falling accident, a whole-body MDCT including cervical spine is requested; therefore, it is justifiable to say that our material gives a reliable and representative picture of adult spine fractures in falling accidents. The radiation dose the patient is exposed to is considered acceptable compared with the possible extreme consequences of a missed spinal injury [2].
To our knowledge, no studies concerning fracture-type incidences and patterns in falling accidents have been published previously. A limitation of the present study is the small number of cases in some of the subgroups, which makes statistical analysis impossible.
Spinal fractures have been classified according to Denis’ three-column theory [15]. Other approaches, such as Magerl et al.’s, for example [16], could not have been utilized in the present study due to the study’s retrospective nature. Magerl et al.’s. classification [16] provides excellent information in the clinical evaluation of spinal fractures, as it is based on main injury mechanism and pathomorphological uniformity, in consideration of prognostic aspects regarding healing potential. This, however, is data which is not always available in a retrospective study. Furthermore, the subgroups are too numerous for the purpose of this study. Also, due to the retrospective nature of this study, the well-known clinical risk factors for spinal fractures [2] could not be reliably determined.
The most common spine fracture was the burst fracture, located most frequently in the thoracolumbar junction. This is in agreement with previous studies [15]. Compression as well as posterior column fractures were less frequently seen than the more serious burst fractures. The most common location for compression fractures was the same as for burst fractures, i.e., the thoracolumbar junction; therefore, as conventional radiography has only a limited capacity to reveal all details of a more complex injury, CT should be used to differentiate these two fracture types, as the correct diagnosis might be crucial for the outcome.
In the present study, the incidence of burst and compression fractures increased with height, which may indicate the injury mechanism. From lower heights the patients probably hit the ground head first, resulting in hyperflexion or extension injury due to the high mobility of the cervical spine [17], whereas falling from greater heights the part of the body that absorbs the first impact is a matter of chance. This could, at least partly, explain the increase of burst and compression fracture incidence with height.
Posterior column fractures were most common in the cervical spine. These fractures are mostly hyperflexion injuries [18]. In our study, the proportion of the cervical fractures decreased with height, probably due to the fact that increasing falling height results in more severe head and neck injuries if a subject hits the ground head first, causing a higher pre-hospitalization mortality. This might be why there were fewer upper cervical spine injuries in our study than in the NEXUS (National Emergency X-Radiography Utilization Study) cervical spine injury cohort [7]. It is not known how many of the accidentally fallen patients had in fact jumped on purpose, but those who had intentionally jumped seemed to have had a greater falling height.
Falling height was reciprocally proportional to age; however, that does not seem to affect the incidence of spine fractures, which did not decrease with increasing age. This might be because of the more rigid and weakened bone structure causing a lesser ability to absorb and withstand impact forces, which makes the occurrence of a fracture more likely regardless of the falling height [19].
The ratio of all MDCT examinations with pathological findings to those without pathological findings was approximately constant regardless of falling height or age. Only the amount of normal cervical MDCT examinations increased with falling height. This is because in our hospital, if patients have had high-energy accidents, cervical MDCT is routinely performed with head and body MDCT to rule out cervical fractures. In our hospital, as in many other major trauma centers, conventional lateral cervical radiography is no longer included in the trauma series of seriously traumatized patients [8, 20]. The low number of normal thoracolumbar MDCT examinations is due to the fact that this region is already scanned in the body MDCT.
Multiple-level spine fractures were seen in 41 (32%) patients, of which in 12 patients (29%) the fractures were at noncontinuous levels. This should be kept in mind when scanning the patient [21]. Radiographs are of limited sensitivity, and also, if a too limited scan area is used in CT, these fractures can be easily missed. When using the so-called retro-reconstruction technique in MDCT, where the reformats are, for example, calculated from the imaging data acquired in body MDCT scan, this pitfall can be avoided.
Multidetector CT is fast, has fewer motion artifacts, reduced partial-volume effects, decreased image noise, better i.v. contrast material opacification of blood vessels, and increased enhancement of parenchymal organs, high-quality multiplanar reformation (MPR), and isotropic viewing, all of which increases the diagnostic power of this imaging modality, benefiting the emergency trauma patients [8, 11, 13]. Although replacing the four-section MDCT systems with 8-, 16-, or even 32-section MDCT systems should speed up the imaging process and decrease artifacts, the occupied scanner room time per patient will not significantly decrease in the future, as the actual scanning time takes up only a minor part of the occupied scanner room time. The greater part of the occupied scanner room time is spent with patient preparation, injector setup, and the programming of the scanner. This is especially the case in seriously injured trauma patients, whose vital signs are continuously being monitored by emergency room staff and, if necessary, life-saving therapies are administered while the patient is in the CT scanner room. Since sagittal and coronal reformations are considered standard in spine CT [8], they are also routinely included in our institution. In some cases of spine fracture, 3D surface renderings may give additional information in the diagnostic interpretation [14]. On the other hand, MDCT technique produces a large number of images, and, therefore, in emergency trauma cases at our hospital, the radiologist-on-call reads the CT images on-line by the scanner console, and the surgeon is given an immediate preliminary report, followed by a written report within the next 30 min.
Conclusion
Spine fractures due to falling accidents are common. Burst fracture is the most common fracture type and is most frequently seen in the thoracolumbar junction. Multiple-level fractures were seen in 32% of the cases, of which 29% were located at noncontinuous levels. Serious spine fractures were seen in all falling height and age groups.
References
Harris JH Jr (2000) Spine, including soft tissues of the pharynx and neck. In: Harris JH Jr, Harris WH (eds) The radiology of emergency medicine. Lippincott Williams and Wilkins, Philadelphia, pp 137–298
Jelly LM, Evans DR, Easty MJ, Coats TJ, Chan O (2000) Radiography vs spiral CT in the evaluation of cervicothoracic junction injuries in polytrauma patients who have undergone intubation. Radiographics 20:251–259
Edwards MJ, Frankema SP, Kruit MC, Bode PJ, Breslau PJ, van Vugt AB (2001) Routine cervical spine radiography for trauma victims: Does everybody need it? J Trauma 50:529–534
Lali HS, Fehlings MG (2001) Epidemiology, demographics, and pathophysiology of acute spinal cord injury. Spine 26:2–12
Ghanta MK, Smith LM, Polin RS, Marr AB, Spires WV (2002) An analysis of eastern association for the surgery of trauma practice guidelines for cervical spine evaluation in a series of patients with multiple imaging techniques. Am Surg 68:563–568
Floyd T (2001) Alpine skiing, snowboarding, and spinal trauma. Arch Orthop Trauma Surg 121:433–436
Goldberg W, Mueller C, Panacek E, Tigges S, Hoffman JR, Mower WR (2001) Distribution and patterns of blunt traumatic cervical spine injury. Ann Emerg Med 38:17–21
Novelline RA, Rhea JT, Rao PM, Stuk JL (1999) Helical CT in emergency radiology. Radiology 213:321–339
Blackmore CC, Mann FA, Wilson AJ (2000) Helical CT in the primary trauma evaluation of the cervical spine: an evidence-based approach. Skeletal Radiol 29:632–639
Borock EC, Gabram SG, Jacobs LM, Murphy MA (1991) A prospective analysis of a two year experience using computed tomography as an adjunct for cervical spine clearance. J Trauma 31:1001–1005
Linsenmaier U et al. (2002) Whole-body computed tomography in polytrauma: techniques and management. Eur Radiol 12:1728–1740
Leidner B, Beckman MO (2001) Standardized whole-body computed tomography as screening tool in blunt multitrauma patients. Emerg Radiol 8:20–28
Rydberg J, Buckwalter KA, Caldemeyer KS et al. (2000) Multisection CT: scanning techniques and clinical applications. Radiographics 20:1787–1806
Kösling S, Dietrich K, Steinecke R, Klöppel R, Schulz HG (1997) Diagnostic value of 3D CT surface reconstruction in spinal fractures. Eur Radiol 7:61–64
Denis F (1984) Spinal instability as defined by the three-column spine concept in acute spinal trauma. Clin Orthop 189:65–76
Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S (1994) A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 3:184–201
Daffner RH, Daffner SD (2002) Vertebral injuries: detection and implications. Eur J Radiol 42:100–116
Allen BL Jr, Ferguson RL, Lehmann TL, O’Brien RP (1982) A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 7:1–27
Mann FA, Lomoschitz FM (2002) Improving the imaging diagnosis of cervical spine injury in the very elderly: implications from the epidemiology of injury. American Society Of Emergency Radiology (ASER) Scientific program, pp 80–83
Nunez DB et al. (1994) Clearing the cervical spine in multiple-trauma victims: a time-effective protocol using helical computed tomography. Emerg Radiol 1:273–278
Keenen TL, Antony J, Benson DR (1990) Non-contiguous spinal fractures. J Trauma 30:489–501
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bensch, F.V., Kiuru, M.J., Koivikko, M.P. et al. Spine fractures in falling accidents: analysis of multidetector CT findings. Eur Radiol 14, 618–624 (2004). https://doi.org/10.1007/s00330-003-2090-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-003-2090-6