
Abstract
The aim of this study was to describe the MRI findings and clinical observations in a fatigue stress fracture of the sacrum. In this retrospective study, 380 conscripts (53 women, 327 men; age range 18–29 years, mean age 20.7 years) who suffered from stress-related hip pain were studied with MRI of the pelvis. The findings of MRI were evaluated with regard to stress fracture of the sacrum. Thirty-one (8%) patients had MRI changes in signal intensity of the cranial part of the sacrum, extending to the first and second sacral foramina. The MRI changes in signal intensity were intermediate on T1-weighted images, and high on short tau inversion recovery or T2-weighted fat-suppressed images. A linear signal void fracture line was also seen. Multiple stress injuries to the pelvic bones were also seen in 7 of 31 (23%) patients. Five patients (16%) had bilateral sacral stress fracture. Fatigue sacral stress fractures appeared more commonly in women than in men (p<0.001). During recovery time 20 of the 31 patients underwent control MRI, and fatty marrow conversion was seen in 8 (40%) cases as high signal intensity on T1-weighted images, which disappeared 5–6 months after the onset of symptoms. Fatigue sacral stress fractures are associated with stress-related hip pain. These fractures were more common in women than in men. Other stress injuries of the pelvis may be seen simultaneously with sacral stress fractures. Signal intensity of the sacrum was normal after 5–6 months.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Stress fractures of the sacrum can be subgrouped into insufficiency and fatigue stress fractures. Insufficiency stress fractures occur in elderly, osteoporotic patients or in patients having undergone radiation therapy for pelvic malignancy [1, 2]. Fatigue stress fractures of the sacrum are very rare and appear in physically active people, and only case reports have been published on the topic [3, 4, 5, 6, 7]. The main symptoms include buttock pain or low-back pain mimicking sciatica. Radiography is often false negative in stress fractures of the sacrum; therefore, verification of diagnosis of sacral stress fractures has been based on CT, bone scintigraphy, or MR imaging [1, 3].
The purpose of the present article is to describe the MRI findings and clinical observations in a fatigue stress fracture of the sacrum.
Materials and methods
This retrospective study took place in the Central Military Hospital, Helsinki, Finland, and the study was approved by the Medical Ethics Committee of the Central Military Hospital. Inclusion criteria were stress-related pain, MRI of the pelvis, and a fatigue bone stress fracture of the sacrum during the period from April 1997 to October 2001. Altogether 380 patients (53 women, 327 men; age range 18–29 years, mean age 20.7 years) were studied with MRI of the pelvis. After clinical examination, which included a careful history, the patients were primarily suspected of having stress fracture of the femoral neck, which is not uncommon in military recruits.
Conventional plain-film radiographs were taken in standard anteroposterior projection from the pelvis in all patients. The pelvis radiographs were taken on average 10 days (range 0–17 days) before MRI.
To exclude stress fracture of the femoral neck all patients underwent MRI using a 1.0-T scanner (GE Signa, Millwaukee, Wis.). Following delay in diagnosis of sacral stress fracture using only a local surface coil of the hip in our first patient, the MRI protocol was extended to cover the pelvis, using a body coil. Routine coronal T1-weighted spin-echo (SE) sequence images (TR/TE=600 ms/19 ms, with two signals averaged, and a 256×224 matrix) were obtained, followed by coronal and axial T2-weighted fast-spin-echo (FSE) sequences with fat suppression (TR/TE=3000–6200 ms/75–80 ms, with two signals averaged and a 512–256×224 matrix). A coronal short tau inversion recovery (STIR) sequence was also used [TR/TE=5400 ms/17 ms, inversion time (TI)=140 ms, with two signals averaged and a 256×224 matrix]. The field of view (FOV) was 32–48×24–48 cm, and the slice thickness was 4.0–5.0 mm, with a 0.5- to 1.0-mm intersection gap. In some cases of abnormal findings in the sacrum, this MR protocol was followed by oblique coronal (assessed along the longitudinal axis of sacrum determined in the sagittal scout plane) T1-weighted SE images (TR/TE=400–500 ms/20 ms, with two signals averaged), and T2-weighted FSE images using fat suppression (TR/TE=4000–4600 ms/80–100 ms, with two signals averaged). The FOV was 30 cm and a matrix of 256×224 was used.
Before the continuation of their more advanced military training program, 20 patients underwent a control MRI examination after 6 weeks to secure healing of the fracture. Because of abnormal MRI of the sacrum, 8 of these 20 patients had another control MRI examination 5–6 months after the primary MRI.
In 5 patients two-phase bone scintigraphy was performed on a Siemens Multispect 2 Dual Detector Gamma Camera System (Siemens Medical Engineering Group, Erlangen Germany). An average dose of 590 MBq TechneScan HDP (oxidronate; Mallinckrodt, Petten, The Netherlands) was injected into an antecubital vein. A high-resolution collimator was used. Blood-pool images were obtained within 5 min of the injection and delayed-phase images 3 h after the injection. The diagnosis of an acute stress injury to bone was based on the presence of a focal, cortical, and medullary zone of increased radionuclide uptake in both phases of bone scintigraphy.
Statistical analysis was performed to see whether there were any differences in appearance of stress fracture of the sacrum between women and men. Statistical analysis was performed using a commercially available software package (Arcus QuickStat Biomedical version 1.1, 1997; Addison-Wesley-Longman Ltd., Cambridge, U.K.). The proportion test was used, and in the statistical analysis, two-sided p values were calculated. Significance was assumed if a p value was less than 5%.
Results
Between April 1997 and October 2001, 31 (8%) patients of the 380 patients studied with MRI of the pelvis revealed a stress fracture of the sacrum related to increased physical activity. There were 18 men and 13 women (age range 18–26 years, mean age 20 years). All patients with a sacral stress fracture suffered from unilateral hip pain appearing during their military training. The duration of symptoms lasted 7–90 days (mean 26 days). On clinical examination, the diagnosis of stress fracture of the femoral neck could not be excluded, and in all 31 patients the radiography of the pelvis and hip was normal.
On MRI all patients revealed changes in signal intensity in the upper part of the sacrum, medial to the sacroiliac joint. On T1-weighted images, an area of low signal intensity could be seen. On STIR and T2-weighted fat-suppressed images, high signal intensity was seen in the corresponding area. The images also revealed an oblique, linear signal void line that extended to the upper first and second sacral foramina (Figs. 1, 2, 3). In all 5 patients having undergone two-phase bone scintigraphy, the MRI findings corresponded to the site of uptake of the tracer in bone scintigraphy (Fig. 1).

A 21-year-old female conscript suffering from left hip pain for 28 days. a Negative radiography of the left side of the pelvis. b Bone scintigraphy of pelvis. Anteroposterior view shows increased uptake of tracer in the left sacrum. c Corresponding oblique coronal T1-weighted spin-echo image (TR/TE: 600 ms/19 ms) reveals a left-sided sacral fracture line of low signal intensity (arrow), surrounded by endosteal edema of low signal intensity (arrowheads). d Coronal short tau inversion recovery (STIR) image (TR/TE/TI: 5400 ms/17 ms/140 ms) also reveals sacral fracture line of low signal intensity (arrow), surrounded by endosteal edema of high signal intensity (arrowheads). e Control MRI 6 weeks later. Oblique coronal T1-weighted spin-echo image (TR/TE: 600 ms/19 ms) demonstrates high signal intensity in sacral stress fracture (arrowheads). Disappearing fracture line (arrow) is surrounded by high signal intensity in the left sacrum

A 19-year-old female conscript with left hip pain for 35 days. a Coronal T2-weighted fat-saturated fast spin-echo image (TR/TE: 5620 ms/78 ms) reveals bilateral sacral stress fracture. Low signal fracture lines (arrows) are surrounded by edema of high signal intensity (arrowheads). b Coronal T2-weighted fat-saturated fast spin-echo image (TR/TE: 5620 ms/78 ms) of the anterior pelvis bone shows a stress fracture of the femoral neck associated with bilateral sacral stress fracture. Low signal fracture line (arrow) of the medial femoral neck is surrounded by endosteal edema of high signal intensity (arrowheads)

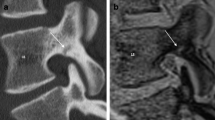
A 20-year-old male conscript with right hip pain for 32 days. a Coronal T2-weighted fat-saturated fast spin-echo image (TR/TE: 6200 ms/78 ms) reveals a right-sided sacral fracture line of low signal intensity (arrow), surrounded by endosteal edema, high signal intensity (arrowheads). b Corresponding coronal T1-weighted spin-echo image (TR/TE: 600 ms/19 ms) reveals a right-sided sacral fracture line of low signal intensity (arrow), surrounded by endosteal edema, high signal intensity (arrowheads). c Control MRI 6 weeks later. Oblique coronal T1-weighted spin-echo image (TR/TE: 640 ms/19 ms) demonstrates high signal intensity in sacral stress fracture (arrowheads). Disappearing fracture line (arrow) is surrounded by high signal intensity in the right sacrum
Table 1 shows the distribution of the stress fractures in 31 patients. Multiple stress injuries to the pelvic bones were also seen in 7 (23%) patients of 31 patients, 5 (16%) of whose stress fractures were bilateral (Fig. 2).
In relation to the number of women (2102) and men (142,654) serving in the Finnish Defense Forces from April 1997 to October 2001, women had a sacral stress fracture more frequently than men (p<0.0001).
During recovery time 20 of the 31 patients underwent control MRI, and fatty marrow conversion was seen in 8 (40%) cases as high signal intensity on T1-weighted images, which disappeared 5–6 months after the onset of symptoms.
In all patients the physical program in military training was interrupted for 6 weeks. Twenty of the 31 patients underwent control MRI. In those 12 (60%) patients with minor findings, mainly endosteal edema, seen in the primary MRI, showed no traces of the bone stress injury at the 6-week control MRI. In those 8 (40%) cases of more advanced bone stress injury, fracture line, at the primary MRI there was on T1-weighted images an area of high signal intensity at the 6-week control MRI (Figs. 1, 3). At this point, STIR and T2-weighted fat-suppressed images showed normal signal intensity in the sacrum. The fracture line was seen less clearly and disappearing on T1-weighted, STIR, and T2-weighted fat-suppressed images during the follow-up (Figs. 1, 3). The symptoms disappeared during the 6-week recovery period. On the 5- to 6-month control MRI the high signal intensity changes on the T1-weighted images disappeared in all 8 patients.
Discussion
Insufficiency stress fractures occur when a normal load is exerted on abnormal bone. Insufficiency fractures of the sacrum appear in postmenopausal women suffering from severe osteoporosis and in patients having undergone radiation therapy of the pelvis [1, 2]. They are also seen in patients suffering from rheumatoid arthritis, fibrous dysplasia, Paget’s disease, osteogenesis imperfecta, osteopetrosis, osteomalacia, and hyperpararthyroidism [1, 8, 9, 10].
In contrast to insufficiency stress fractures, fatigue stress fractures appear when an abnormally large load is exerted on normal bone. Fatigue stress fractures of the sacrum are very rare, occurring in healthy, physically active people. Only case reports have been published on fatigue stress fractures of the sacrum, e.g., they have been recorded in long-distance runners [3, 4, 5, 6]. Military recruits may also develop stress fracture of the sacral wing during rigorous basic training [7]. Children may also show stress fractures of the sacrum [11], but in these patients the differential diagnoses may also include bone tumors and osteitis [12]. Pregnant women may also develop sacral stress fractures, although it is a matter of opinion whether this represents insufficiency stress fractures related to osteoporosis of the sacrum in association with pregnancy or fatigue stress fractures due to unaccustomed stress related to rapid and excessive weight gain in the last trimester of pregnancy [13].
Whether it concerns insufficiency or fatigue stress fractures, symptoms of low-back pain may lead to examinations of the lumbar spine and, subsequently, to delay in correct diagnosis [3]. Correct diagnosis of insufficiency stress fracture of the sacrum can be assessed in elderly and osteoporotic patients, as well as in those patients whose chronic diseases are known to relate to insufficiency stress fracture of the sacrum. The symptoms may also appear along with hip pain, which may also simulate stress fracture of the femoral neck. Typically, pain related to stress fractures becomes worse during or after exercise, as has appeared in the present conscripts.
Stress fractures may be nutritionally based [3, 14]. In female long-distance runners amenorrhea is common; in the present patients women were numerous but did not suffer from amenorrhea. Compared with men, women had to carry the same type of military equipment on their backs. Since the women were smaller, these weights and the resulting vertical loads on the axial skeleton were larger than those carried by men. This is apparently the main reason for the more numerous stress fracture cases shown by women in the present series.
Since sacral fatigue stress fractures are rarely encountered, their diagnosis in healthy patients is often delayed. In military recruits, sacral fatigue stress fractures have seldom been reported [7]; however, in the military population fatigue stress fractures of the femoral neck are not uncommon [15]. Hip pain is the most typical complaint associated with stress fracture of the femoral neck. Since these stress fractures may progress to displaced fractures, special interest has been focused on their early diagnosis in order to prevent complicated fractures. Based on clinical examination, we also found sacral stress fractures in 31 patients in whom hip pain was the main complaint and, accordingly, these cases were at clinical examination primarily diagnosed as fatigue stress fracture of the femoral neck. In the first patient, the results of clinical examination hidden by the MRI protocols typically used in the study of fatigue stress fractures of the femoral neck, and consequently, the final diagnosis of sacral fatigue stress fracture, was delayed. For this reason our MRI protocol was extended to examine the entire pelvis in patients suffering from hip pain related to increased physical activity.
Plain films are helpful in excluding sacral tumors [3]. Stress fractures of the sacrum may not be identified, due to overlying bowel gas and the geometry of the sacrum [1, 3]. In addition, sacral stress fractures tend not to produce callus and are thus more difficult to visualize [3].
In addition to patient history of a renewed physical exercise associated with pain, diagnosis of the fatigue stress fractures of the sacrum has been based on findings in bone scintigraphy, CT, and MR imaging. In all these imaging techniques findings of sacral stress fracture are seen in the alae of the sacrum. The fracture line, verified with CT and MRI, is parallel to the sacroiliac joint. In insufficiency stress fractures of the sacrum the findings are most often bilateral, presenting a typical butterfly sign or H-shaped sign, although a unilateral appearance has also been seen [1, 16]. In contrast to insufficiency fracture of the sacrum, sacral fatigue stress fracture most commonly appears unilaterally; however, bilateral appearances of sacral fatigue stress fracture may be seen in long-distance runners [3]. In the present military population 16% of patients with fatigue stress fractures showed a marked bilateral appearance.
Bone scintigraphy is a very sensitive imaging modality often used to reveal stress fracture of the sacrum if the fracture appears as a typical butterfly configuration [1]; however, in cases of atypical appearance bone malignancies and infection can be included in differential diagnosis. Although MRI is as sensitive as bone scintigraphy in the assessment of sacral stress fracture, signal changes in the bone marrow may be nonspecific or confusing and need further evaluation with CT [12]. In the present study, MRI very readily revealed a fracture line. Although CT has been considered to be the most reliable tool in the determination of sacral stress fracture, since it reveals the fracture line and associated sclerosis along the fracture line [1, 12], we believe that a positive finding of sacral stress fracture with a fracture line need not be verified with CT. This is in accordance with Major and Helms [3], who considered that the findings of sacral stress fracture in CT and MRI were characteristic signs of sacral stress fracture. The linear appearance in both imaging techniques is consistent with the presence of this type of fracture.
Magnetic resonance imaging findings of stress fractures or stress injuries to bone are widely accepted [17, 18, 19]. In stress injuries to bone T1-weighted images show areas of low signal intensity, which on T2-weighted images or STIR images are of high signal intensity, these changes in MRI signal intensity represent edema of bone. A signal void fracture line is seen in advanced stress injuries, or stress fractures in all MRI sequences [3, 20]. These findings were also noted on the MR images of the present patients with sacral fatigue stress fracture. In the present study the edema and the fracture line in the fatigue fractures of the sacrum was seen in the uppermost part of the alae of the sacrum, extending to the first and second sacral foramina. Insufficiency fractures of the sacrum, however, show a different kind of pattern, revealing edema and the fracture line parallel to the sacroiliac joint [21]. Although fluid has been depicted as a new diagnostic sign of insufficiency fractures of the sacrum [22], this sign was not found in any of our patients with fatigue stress fractures of the sacrum.
Stress fractures may be multiple, and some are asymptomatic. In insufficiency stress fractures of the sacrum, associated stress fractures are often seen in the pubic arches, acetabulum, or symphysis pubis [1]. In addition to fatigue stress fracture of the sacrum, 4 of our patients had simultaneous stress fractures of the femoral neck, iliac bone, or inferior pubic ramus. All our patients complained of unilateral pain; thus, any stress fracture on the contralateral side in the bony pelvis was asymptomatic.
Sacral fatigue stress fractures are treated with prolonged rest, in which no physical activity is permitted. Healing of sacral fatigue stress fractures can be followed up with MRI. Six weeks after onset of treatment, MRI often reveals a higher signal intensity at the site of the fatigue stress fracture on T1-weighted images, whereas STIR and T2-weighted fat-suppressed images appear to be normal. A fracture line is less distinctly seen and disappears on all MR images. The same findings have been seen in cases of stress fractures of the femoral neck [23]. This is indicative of fatty marrow conversion and is a normal appearance associated with healing. At this time the patients are asymptomatic. This finding seen on T1-weighted images is crucial for the diagnosis of possible recurrent symptoms and whether the patient will be followed up with MRI. The high signal intensity on T1-weighted images disappeared by time, in 5–6 months in our study.
Conclusion
Fatigue stress fractures of the sacrum appear to be underreported. They are, however, seen in patients having undergone vigorous physical training, more commonly in women than in men. Hip pain associated with a history of increased or changed physical activity may be due to fatigue stress fracture of the femoral neck as well as that of the sacrum. The MRI of the pelvis is needed to confirm these diagnoses. Typically, edema and the fracture line in the fatigue fractures of the sacrum are seen in the uppermost part of the alae of the sacrum, extending to the first and second sacral foramina. Five to 6 months after the onset of symptoms of fatigue sacral stress fractures, the signal intensity in MRI of this anatomical region is normal.
References
Peh WC, Khong PL, Ho WY, Yeung HW, Luk KD (1995) Sacral insufficiency fractures: spectrum of radiological features. Clin Imaging 19:92–101
Parikh VA, Edlund JW (1998) Sacral insufficiency fractures: rare complication of pelvic radiation for rectal carcinoma: report of a case. Dis Colon Rectum 41:254–257
Major NM, Helms CA (2000) Sacral stress fractures in long-distance runners. Am J Roentgenol 174:727–729
Eller DJ, Katz DS, Bergman AG, Fredericson M, Beaulieu CF (1997) Sacral stress fractures in long-distance runners. Clin J Sports Med 7:222–225
Czarnecki DJ, Till EW, Minikel JL (1988) Unique sacral stress fracture in a runner. Am J Roentgenol 151:1255
Bottomley MB (1990) Sacral stress fracture in a runner. Br J Sports Med 24:243–244
Volpin G, Milgrom C, Goldsher D, Stein H (1989) Stress fractures of the sacrum following strenuous activity. Clin Orthop:184–188
Lam KS, Moulton A (2001) Stress fracture of the sacrum in a child. Ann Rheum Dis 60:87–88
West SG, Troutner JL, Baker MR, Place HM (1994) Sacral insufficiency fractures in rheumatoid arthritis. Spine 19:2117–2121
Weber M, Hasler P, Gerber H (1993) Insufficiency fractures of the sacrum: twenty cases and review of the literature. Spine 18:2507–2512
Grier D, Wardell S, Sarwark J, Poznanski AK (1993) Fatigue fractures of the sacrum in children: two case reports and a review of the literature. Skeletal Radiol 22:515–518
Martin J, Brandser EA, Shin MJ, Buckwalter JA (1995) Fatigue fracture of the sacrum in a child. Can Assoc Radiol J 46:468–470
Thienpont E, Simon JP, Fabry G (1999) Sacral stress fracture during pregnancy: a case report. Acta Orthop Scand 70:525–526
Johnson AW, Weiss CB Jr, Stento K, Wheeler DL (2001) Stress fractures of the sacrum: an atypical cause of low back pain in the female athlete. Am J Sports Med 29:498–508
Milgrom C, Giladi M, Stein M et al. (1985) Stress fractures in military recruits: a prospective study showing an unusually high incidence. J Bone Joint Surg (Br) 67:732–735
Brahme SK, Cervilla V, Vint V, Cooper K, Kortman K, Resnick D (1990) Magnetic resonance appearance of sacral insufficiency fractures. Skeletal Radiol 19:489–493
Yao L, Johnson C, Gentili A, Lee JK, Seeger LL (1998) Stress injuries of bone: analysis of MR imaging staging criteria. Acad Radiol 5:34–40
Daffner RH, Pavlov H (1992) Stress fractures: current concepts. Am J Roentgenol 159:245–252
Weishaupt D, Schweitzer ME (2002) MR imaging of the foot and ankle: patterns of bone marrow signal abnormalities. Eur Radiol 12:416–426
Featherstone T (1999) Magnetic resonance imaging in the diagnosis of sacral stress fracture. Br J Sports Med 33:276–277
Grangier C, Garcia J, Howarth NR, May M, Rossier P (1997) Role of MRI in the diagnosis of insufficiency fractures of the sacrum and acetabular roof. Skeletal Radiol 26:517–524
Peh WCG (2000) Intrafracture fluid: a new diagnostic sign of insufficiency fractures of the sacrum and ileum. Br J Radiol 73:895–898
Slocum KA, Gorman JD, Puckett ML, Jones SB (1997) Resolution of abnormal MR signal intensity in patients with stress fractures of the femoral neck. Am J Roentgenol 168:1295–1299
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ahovuo, J.A., Kiuru, M.J. & Visuri, T. Fatigue stress fractures of the sacrum: diagnosis with MR imaging. Eur Radiol 14, 500–505 (2004). https://doi.org/10.1007/s00330-003-1989-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-003-1989-2