
Abstract
A 23-year-old Japanese woman with no history of corticosteroid intake or alcohol abuse presented with a 10-month history of left hip pain without any antecedent trauma. An anteroposterior radiograph performed 10 months after the onset of pain showed slight joint space narrowing and bone erosions surrounded by sclerotic lesions in both the acetabular roof and femoral neck. Magnetic resonance images of the left hip showed a feature of osteonecrosis of the femoral head and a mass with villus proliferation extending from the posterior intertrochanteric area to the anteromedial aspect of the femoral neck. In addition, the left quadratus femoris muscle, which is generally located just above the nutrient vessels of the femoral head, was not detected. Based on these findings, the patient was diagnosed with osteonecrosis of the femoral head caused by impairment of the nutrient vessels from invasion of the pigmented villonodular synovitis. She underwent radical synovectomy of the left hip 16 months after the onset of pain, and her hip pain improved after the surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteonecrosis of the femoral head (ONFH) occurs mainly in relation to corticosteroid intake or alcohol abuse [1]. Although the precise mechanism of ONFH development remains unclear, it is generally considered to be secondary to disturbance of the nutrient artery, leading to ischemia. Previously suggested intravascular mechanisms of the etiology of ischemic events include fat embolism, hyperlipidemia, intravascular coagulation, and vasospasm [2–5]. Extravascular mechanisms have also been reported, including traumatic vascular injury due to femoral neck fracture or hip dislocation [6]. To our knowledge, only one report has described tumorous lesions of the hip joint causing impairment of the nutrient artery of the femoral head, eventually resulting in ONFH. We herein report a rare case of ONFH associated with pigmented villonodular synovitis (PVNS) and discuss the anatomy of the nutrient vessels of the femoral head.
Report of the case
This report was approved by our institutional review board. A 23-year-old Japanese woman developed left hip pain without any antecedent trauma. She had no history of corticosteroid intake, alcohol abuse, or smoking. No radiographic abnormalities were detected around the left hip joint immediately after the onset of pain. However, the hip pain continued for 10 months, and the range of motion was slightly restricted due to the pain. The results of blood examinations, including the C-reactive protein concentration and erythrocyte sedimentation rate, were within the normal range.
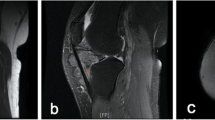
Ten months after the onset of pain, a plain radiograph showed slight joint space narrowing and bone erosions surrounded by sclerotic lesions in both the acetabular roof and femoral neck (Fig. 1). Magnetic resonance (MR) images showed a continuous nodular mass with villus proliferation from the posterior intertrochanteric area to the anteromedial aspect of the femoral neck. Additionally, a low-intensity band lesion in the left femoral head was seen on T1-weighted MR images; this is a characteristic feature of ONFH. The proximal side of the band was not enhanced on gadolinium-enhanced T1-weighted MR images (Fig. 2). Moreover, the left quadratus femoris muscle was not detected due to invasion of the mass (Fig. 3). This mass lesion exhibited low intensity on T1- and T2-weighted MR images, and the fluid lesion inside the mass exhibited high intensity on T2-weighted MR images. The surrounding area of the mass was enhanced on gadolinium-enhanced T1-weighted MR images.

a An anteroposterior radiograph obtained 10 months after the onset of pain showed slight joint space narrowing and bone erosions surrounded by sclerotic lesions in both the acetabular roof and femoral neck (white arrows). b A lateral radiograph of the left hip showed bone erosion in the center of the femoral neck

Magnetic resonance images obtained 10 months after the onset of pain. a An axial T1-weighted image [repetition time/echo time (TR/TE), 550/10 ms] showed a low-intensity mass lesion with villus proliferation from the posterior intertrochanteric area to the anteromedial aspect of the femoral neck (white arrowheads). b An axial T2-weighted image (TR/TE, 4700/105 ms) showed a mixed high- and low-intensity mass lesion (white arrowheads). c On a gadolinium-enhanced T1-weighted magnetic resonance image (TR/TE, 600/10 ms), the surrounding area of the mass was enhanced (white arrowheads). d A low-intensity band on a coronal T1-weighted image [repetition time/echo time (TR/TE), 550/10 ms] of the left femoral head showed a characteristic appearance of osteonecrosis (smooth, concave, and circumscribing all necrotic segments) (white arrows). e On the gadolinium-enhanced, fat-suppressed, T1-weighted images’ coronal view (TRTE, 570/10 ms), the proximal side of the band was not enhanced

On a gadolinium-enhanced T1-weighted axial MR image [repetition time/echo time (TR/TE), 600/10 ms], the left quadratus femoris muscle was not observed due to invasion of the mass (compared with contralateral side; white arrows)
Based on these findings, the patient was diagnosed with PVNS-associated ONFH. Collapse of the femoral head was not observed during the follow-up period. Therefore, she underwent radical synovectomy of the left hip joint about 16 months after the onset of pain. The histopathological findings of the resected synovial tissues were consistent with those of PVNS; i.e., nodular proliferation of spindle-shaped cells, aggregates of foamy histiocytes, and the presence of hemosiderin deposits (Fig. 4). The patient’s hip pain improved postoperatively.

Sections show nodular proliferation of oval to short spindle-shaped cells arranged in sheets, accompanied by hyalinized collagenous stroma. Multinucleated giant cells, aggregates of foamy histiocytes, and hemosiderin deposits are also seen. These features are consistent with those of pigmented villonodular synovitis. a Hematoxylin and eosin staining; original magnification, ×200. b Hematoxylin and eosin staining; original magnification, ×400
Discussion
ONFH is generally considered to be the result of a disturbance of the nutrient artery, leading to ischemia. The nutrition of the femoral head is reportedly supplied mainly by the superior retinacular artery (SRA) from the deep branch of the medial femoral circumflex artery (MFCA), occlusion of which is related to the occurrence of ONFH [7]. Anatomically, the deep branch of the MFCA runs over the lesser trochanter, ascends along the intertrochanteric crest, and then branches the SRA at the retinaculum of the femoral neck [8].
The diagnosis of ONFH is based on established diagnostic criteria, including findings on plain radiographs and MR images [9]. In the present case, plain radiographs showed diffuse osteosclerosis in the left femoral head without collapse, which differs from the characteristic findings of ONFH such as linear sclerosis or the crescent sign. Considering that the presence of hemosiderin observed in PVNS represents various increased densities on plain radiographs [10], these osteosclerotic changes in the present case may reflect the presence of PVNS. On the other hand, gadolinium-enhanced MR images of patients with ONFH show that the surrounding necrotic area generally is not enhanced, which differs from the characteristics of PVNS. Therefore, the low-intensity lesion inside the femoral head on T1-weighted MR images was considered to indicate ONFH in the current case.
We searched PubMed to identify relevant literature using the following terms: osteonecrosis and pigmented villonodular synovitis, in accordance with the previous report that indicates the steps in writing a narrative review [11]. PVNS is a rare disease observed in young adults aged 20–40 years. Therefore, only a few studies have reported cases of PVNS in patients with ONFH (Table 1) [10, 12, 13]. Similar to these reports, the patient in our case was a young adult within this age range. However, the causal relationship between PVNS and ONFH remains controversial. Vigorita [14] reported five cases in which routinely examined synovial tissues removed during joint surgery were pathologically similar to PVNS, and one was removed from a patient with ONFH. The author stated that whether true PVNS or rare reactions to bone, synovium, and cartilage breakdown products lead to a histologic pattern of PVNS remains unclear. Conversely, only one previous report has described the pathological association between PVNS and ONFH. Mimura et al. [13] reported that multiple bone erosions created by PVNS around the femoral neck may be associated with impairment of the nutrient artery, resulting in ONFH.
In the current case, PVNS was located continuously from the posterior part of the intertrochanteric area to the anteromedial aspect of the femoral neck; this is similar to the localization of the tumor previously reported by Mimura et al. [13]. In contrast, the bone erosion was observed on the superior portion of the femoral neck, apart from the route of the deep branch of the MFCA on radiographs. Furthermore, the deep branch of the MFCA generally runs through the adipose tissue under the quadratus femoris muscle and subsequently branches the SRA [8, 15]. In our case, the left quadratus femoris muscle was not observed because of the mass invasion as shown on MR images. This indicates that impairment of the deep branch of the MFCA at the level of the quadratus femoris muscle can contribute to the occurrence of ONFH (Fig. 5).

Relationship between the route of the primary vessels around the proximal femur and the localization of pigmented villonodular synovitis (PVNS). PVNS was located from the posterior intertrochanteric area to the anteromedial aspect of the femoral neck, corresponding to the route of both the medial femoral circumflex artery and superior retinacular artery
References
Hirota Y, Hirohata T, Fukuda K, Mori M, Yanagawa H, Ohno Y, Sugioka Y (1993) Association of alcohol intake, cigarette smoking, and occupational status with the risk of idiopathic osteonecrosis of the femoral head. Am J Epidemiol 137:530–538
Miyanishi K, Yamamoto T, Irisa T, Yamashita A, Jingushi S, Noguchi Y, Iwamoto Y (2002) Bone marrow fat cell enlargement and a rise in intraosseous pressure in steroid-treated rabbits with osteonecrosis. Bone 30:185–190
Moskal JT, Topping RE, Franklin LL (1997) Hypercholesterolemia: an association with osteonecrosis of the femoral head. Am J Orthop (Belle Mead NJ) 26:609–612
Jones JP Jr (1993) Fat embolism, intravascular coagulation, and osteonecrosis. Clin Orthop Relat Res 292:294–308
Ikemura S, Yamamoto T, Motomura G, Yamaguchi R, Zhao G, Iwasaki K, Iwamoto Y (2013) Preventive effects of the anti-vasospasm agent via the regulation of the Rho-kinase pathway on the development of steroid-induced osteonecrosis in rabbits. Bone 53:329–335
Zlotorowicz M, Czubak J, Caban A, Kozinski P, Boguslawska-Walecka R (2013) The blood supply to the femoral head after posterior fracture/dislocation of the hip, assessed by CT angiography. Bone Joint J 95-B:1453–1457
Atsumi T, Kuroki Y, Yamano K (1989) A microangiographic study of idiopathic osteonecrosis of the femoral head. Clin Orthop Relat Res 246:186–194
Gautier E, Ganz K, Krügel N, Gill T, Ganz R (2000) Anatomy of the medial femoral circumflex artery and its surgical implication. J Bone Joint Surg Br 82:679–683
Sugano N, Atsumi T, Ohzono K, Kubo T, Hotokebuchi T, Takaoka K (2002) The 2001 revised criteria for diagnosis, classification, and staging of idiopathic osteonecrosis of the femoral head. J Orthop Sci 7:601–605
Cotten A, Flipo RM, Chastanet P, Disvigne-Npoulet MC, Duquesnoy B, Delcambre B (1995) Pigmented villonodular synovitis of the hip: review of radiographic features in 58 patients. Skeletal Radiol 24:1–6
Gasparyan AY, Ayvazyan L, Blackmore H, Kitas GD (2011) Writing a narrative biomedical review: considerations for authors, peer reviewers, and editors. Rheumatol Int 31:1409–1417
Xie GP, Jiang N, Liang CX, Zeng JC, Chen ZY, Xu Q, Qi RZ, Chen YR, Yu B (2015) Pigmented villonodular synovitis: a retrospective multicenter study of 237 cases. PLoS ONE 10:e0121451
Mimura T, Kawasaki T, Yagi K, Mori K, Imai S, Matsusue Y (2013) Pigmented villonodular synovitis causing osteonecrosis of the femoral head: a case report. Case Rep Orthop. doi:10.1155/2013/756954
Vigorita VJ (1984) Pigmented villonodular synovitis-like lesions in association with rare cases of rheumatoid arthritis, osteonecrosis, and advanced degenerative joint disease. Clin Orthop Relat Res 183:115–121
Yamamoto T, Motomura G, Karasuyama K, Nakashima Y, Doi T, Iwamoto Y (2016) Results of the Sugioka transtrochanteric rotational osteotomy for osteonecrosis: frequency and role of a defect of the quadratus femoris muscle in osteonecrosis progression. Orthop Traumatol Surg Res 102:387–390
Acknowledgements
This work was partially supported by the Practical Research Project for Rare/Intractable Diseases from the Japan Agency for Medical Research and Development (AMED) and a grant-in-aid in Scientific Research (grant 16K10906) from the Japan Society for the Promotion of Science.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interests.
Informed consent
The patient was fully informed that her data would be submitted for publication, and she gave her consent.
Rights and permissions
About this article

Cite this article
Baba, S., Motomura, G., Fukushi, J. et al. Osteonecrosis of the femoral head associated with pigmented villonodular synovitis. Rheumatol Int 37, 841–845 (2017). https://doi.org/10.1007/s00296-016-3624-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-016-3624-y