
Abstract
Balance impairment is a frequent and undertreated manifestation in ankylosing spondylitis, leading to increased risk of falls and lower quality of life. Our aim was to assess supervised training and home-based rehabilitation efficacy on balance improvement in ankylosing spondylitis subjects on biologic agents. This was a single-blinded, quasi-randomized parallel study in a single outpatient Rehabilitation Clinic of a tertiary referral center. Subjects with ankylosing spondylitis on biologic agents were assigned either to supervised training and home-based rehabilitation program (rehabilitation group) plus educational–behavioral therapy, or to educational–behavioral therapy alone (educational groups). The same therapist provided therapy. Outcome measures were assessed at baseline (T0), end of treatment (T1) and at 7-month follow-up (T2). Rheumatologic outcomes were Bath Ankylosing Spondylitis Metrology Index, Bath Ankylosing Spondylitis Functional Index and Bath Ankylosing Spondylitis Disease Activity Index. Balance parameters (anterior–posterior oscillation, latero-lateral oscillation, sway area, sway density and sway path) were evaluated by stabilometry in a condition of open and closed eyes. Forty-six subjects (36 M, 10 F) were enrolled. Demographic data and clinical status at baseline were comparable between the two groups (22 rehabilitation group, 20 educational group). Primary outcome was sway density that improved both at T1 (SDy: open eyes p = 0.003, closed eyes p = 0.004) and at T2 (SDx: open eyes p = 0.0015, closed eyes p = 0.032). A trend toward improvement in the rehabilitation group rather than in the educational group emerged for balance parameters, especially those measured with closed eyes (0.004 < p < 0.048 at T1 and 0.004 < p < 0.036 at T2). Supervised training and home exercise lead to balance improvement in people with ankylosing spondylitis. Eyes-closed trials show a more marked trend toward improvement, and this may suggest a positive effect of rehabilitation on proprioception.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis is characterized by chronic and progressive inflammation of the axial, sacroiliac and peripheral joints, leading to ankylosis and posture modifications. Extra-articular manifestations including audio-vestibular dysfunction [1–3] may contribute to balance impairment which is often underdiagnosed [4–7]. This may affect up to a third of individuals with the condition [2]. Physical therapy is a mainstay therapy in ankylosing spondylitis. A metanalysis suggested better functional outcome after supervised group physiotherapy in comparison with individual, home or spa therapy [8]. Most of the reported studies were in people not on biologic agents, but two recent reports suggested marked efficacy of physical therapy also in subjects treated with these drugs [9, 10].
We hypothesis that physical therapy, acting synergistically with pharmacological treatment, could improve balance impairment in ankylosing spondylitis. We aim to evaluate the efficacy of a specific exercise protocol [11] on balance quantitative parameters in subjects on biological agents.
Methods
This was a single blinded, quasi-randomized controlled clinical trial. The study was approved by the local ethical committee.
Subjects with a diagnosis of ankylosing spondylitis according to the modified New York criteria were enrolled at a single unit. Inclusion criteria were: age 18–65 years taking infliximab, etanercept or adalimumab for at least 9 months and with a stable Bath Ankylosing Spondylitis Disease Activity Index for the last 6 months. Exclusion criteria were: having participated to other rehabilitation programs in the previous 6 months, having complete spine ankylosis or other medical conditions leading to physical disability. Changes to therapy during the study or withdrawal of consent would lead to drop out from the study.
Intervention and data collection
Participants were alternatively allocated, according to a quasi-randomized study design, to rehabilitation therapy or to educational–behavioral program alone. Rehabilitation consisted of supervised training and home-based rehabilitation plus educational–behavioral training. The educational–behavioral program consisted of group discussions, problem solving, and disease-specific lectures held twice with a two-week interval in between [9–11] (“Appendix”). The rehabilitation group received a previously validated exercise protocol [9–11]. It was developed by an interdisciplinary team (physical medicine doctor, rheumatologist, physiotherapist and psychologist). Twelve twice-weekly sessions lasting 60 min were provided by the same trained physiotherapist. The full protocol is reported in Table 1. At completion of the supervised exercise program, a handout with detailed home exercises was given to each participant. A diary was also provided to record exercise at home. Adherence to the program was monitored by regular follow-up phone calls by a researcher, supplemented by checks of the diaries.
Demographic and disease-related data including age, sex, time since diagnosis, symptom activity, erythrocyte sedimentation rate, reactive C protein, visual analog pain scale, and drugs were collected at baseline.
Primary outcome was sway density improvement. Secondary outcomes were the following quantitative balance and rheumatologic parameters. Rheumatologic and balance outcome measures were recorded at baseline, end of treatment (T1) and at 7-month follow-up (T2). Rheumatologic evaluation included: Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI), and Bath Ankylosing Spondylitis Metrology Index (BASMI). Fatigue and morning stiffness were obtained as sub-items of the BASDAI. Stabilometric analysis provided balance data, including anterior–posterior oscillation, latero-lateral oscillation and sway density. Subjects were allowed to choose their preferred foot position over the force plate during the protocol with feet comfortably apart. The deflections of the center of pressure (CoP) along the lateral (x) and anterior–posterior (y) axes were recorded with a force platform (ARGO, RGMD, Italy) [6]. A proprietary software provided sway area, measuring the area encompassed by CoP, sway density, measuring the entity of oscillations, and sway path, measuring the total length of CoP trajectory.
Each balance parameter was analyzed both with open and closed eyes. Each trial was separated by a 15-min rest interval to minimize fatigue.
Outcome measurements were assessed by the same examiner blinded to treatment.
Statistical analysis
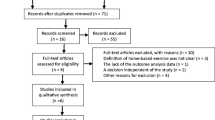
A pre-study sample size calculation predicted that, with an alpha of 5 % and a power of 90 %, a total number of 66 subjects would be needed. The study followed the ITT (intention-to-treat) analysis approach in line with the CONSORT statements [12] (Fig. 1).

Patients enrolled for the trial
Baseline characteristics of the groups were compared by unpaired t tests for independent samples (continuous data). Before–after training improvements (intra-group analysis) were tested with Wilcoxon matched-pairs test at T1 and T2. Mann–Whitney U test tested differences between the two groups (inter-group analysis) in score gains on balance and rheumatologic parameters. Treatment effects were analyzed stratifying by treatment (infliximab, etanercept or adalimumab) with Kruskal-Wallis test. Statistical significance was set at p < 0.05. Statistics were processed using SPSS version 20.0 (SPSS Inc., Chicago, Illinois).
Results
Participants
Participants were enrolled from September 2012 to March 2013. Last follow-up was in October 2013. Sixty-six individuals were screened (46 males). Of these, 46 enrolled (eleven refused consent; nine did not meet inclusion criteria). Four did not complete the full evaluation. A total of 22 (17 males) enrolled in educational and 20 (15 males) in the rehabilitation group, and all these were fully evaluable (Fig. 1).
Participants’ characteristics at baseline
No significant differences in demographics, pain or rheumatologic and balance parameters were detected (Table 2). Adherence to the program based on diary checking suggested that this was high, with home exercises carried out on a daily basis by 79 % of participants and at least 5 day per week by another 10 %.
Balance parameters
Intra-group analysis in the rehabilitation group demonstrated a reduction in closed-eyes oscillations and sway parameters at T1 and T2. Open-eyes parameters, despite not statistically different at the end of rehabilitation treatment, improved at 7-month follow-up compared to baseline (Table 3). In the educational group, open-eyes anterior–posterior oscillation, and open- and closed-eyes sway density improved at end of the rehabilitation program. Open-eyes sway Area improved only at 7-month follow-up (Table 3).
Inter-group comparison suggested better results in the rehabilitation group for latero-lateral oscillations (0.01 > p > 0.009) and some sway parameters (0.003 < p < 0.019), both with open and closed eyes at T1 (Table 3). At follow-up, the rehabilitation group maintained these results, with additional improvement on closed-eyes latero-lateral oscillations (p = 0.004) and all sway measures (0.015 < p < 0.046) (Table 3). The rehabilitation group showed no significant differences between the end of treatment and 7-month follow-up on balance parameters differentiating for drug (0.093 < p < 0.111) and years from diagnosis of ankylosing spondylitis (0.9 < p < 0.14).
Rheumatologic parameters
Intra-group analysis in the rehabilitation group showed Bath Ankylosing Spondylitis Disease Activity Index, Bath Ankylosing Spondylitis Functional Index and Bath Ankylosing Spondylitis Metrology Index improvement at end of rehabilitation program and at follow-up. In the educational–behavioral group, only Disease Activity Index improved at end of treatment, and Functional Index at follow-up (Table 3).
Inter-group comparison yielded better scores for the Metrology Index (p = 0.049 and 0.008) and the Disease Activity Index (p = 0.022 and 0.010) at end of treatment and follow-up in the rehabilitation group. The rehabilitation group showed no differences between end of treatment and 7-month follow-up on rheumatologic parameters differentiating for drug (0.093 < p < 0.111) and years from diagnosis of ankylosing spondylitis (0.9 < p < 0.14).
Discussion
Rehabilitation treatment seems effective on posture control in ankylosing spondylitis in a population taking biological agents, suggesting that there might be a synergistic effect of drugs and rehabilitation on balance. Current guidelines advise the association of physical and pharmacological treatment [13]. Due to recruitment problems, we did not reach the expected power but a clear trend was seen. This is in line with previous findings [8, 11] of a beneficial effects on spine mobility, pain and physical function in a similar population undergoing the same rehabilitation protocol.
This approach provides long-lasting benefits, highlighted by the persistence of improved balance parameters at follow-up. Eyes-closed trials showed a trend to improvement, and this may suggest a positive effect of rehabilitation on proprioception.
Postural control theory considers balance as the product of integrated inputs, and the body as a mechanical system that interacts with the nervous system in a continuously changing environment [14]. In ankylosing spondylitis, the biomechanical system, movement strategies and sensory strategies are likely to be impaired, due to the pathognomonic bone deformities, enthesitis and postulated vestibular dysfunction [1–3, 5].
Pathophysiologically, the observed beneficial results of rehabilitation training could be attributed not only to partial posture correction, but also to effects on vestibular dysfunction [1–3] and diffuse enthesitis [15]. While vestibular dysfunction produces a clear-cut, often asymmetric, disequilibrium, enthesitis, as an inflammatory process of the sites where tendons or ligaments insert into the bone, affects articular capsule nerve endings and Golgi organs. Chemosensitive nociceptor excitation in vertebral joints, muscles and tendons may alter the sensitivity of the muscle spindles by reflex activation of fusimotor neurones, leading to a decreased proprioceptive acuity.
Our study has limitations. Firstly, the expected power was not achieved, which may have prevented us reporting statistically significant results. Our initial hypothesis could not be confirmed but a clear trend for the efficacy of rehabilitation emerges. These results warrant replication on larger samples to confirm our findings.
Another limitation is the lack of enthesitis indexes. Given that correlations between the enthesitis indices and ankylosing spondylitis disease activity measures, participants global assessment and BASMI metrology are reported to be moderate to weak [16], enthesitis indexes were not considered a crucial measurement in the study design.
Another point is that the observed modification of BASDAI is not clinically significant, preventing us to conclude that also disease activity and progression were modified.
The single-blinded nature of the design needs to be considered a minor bias, although we cannot rule out the psychological component of the stricter follow-up and care received by the rehabilitation group. Lastly, the short follow-up may have masked possible relapses.
Despite these limitations, the study offers promising results: although our hypothesis was not fully confirmed, rehabilitation programs in ankylosing spondylitis suggest a benefit also on a neglected symptom such as balance impairment. Trials on larger population samples are needed to confirm these findings.
Transfer of these results to clinical practice should be implemented by incorporating a physical medicine doctor and a physiotherapist in the rheumatology clinic team.
References
Adam M, Erkan AN, Arslan D, Leblebici B, Ozluoglu L, Nafiz Akman M (2008) High-frequency sensorineural hearing loss in patients with ankylosing spondylitis: Is it an extraarticular feature of disease? Rheumatol Int 28:413–417
Amor-Dorado JC, Barreira-Fernandez MP, Vazquez-Rodriguez TR, Gomez-Acebo I, Miranda-Filloy JA, Diaz de Teran T et al (2011) Audiovestibular manifestations in patients with ankylosing spondylitis. Medicine (Baltimore) 90:99–109
Erbek SS, Erbek HS, Yilmaz S, Topal O, Yucel E, Ozluoglu LN (2006) Cochleovestibular dysfunction in ankylosing spondylitis. Audiol Neurootol 11:294–300
Murray HC, Elliott C, Barton SE, Murray A (2000) Do patients with ankylosing spondylitis have poorer balance than normal subjects? Rheumatology (Oxford) 39:497–500
Pompeu JE, Romano RS, Pompeu SM, Lima SM (2012) Static and dynamic balance in subjects with ankylosing spondylitis: literature review. Rev Bras Reumatol 52:409–416
Sawacha Z, Carraro E, Del Din S, Guiotto A, Bonaldo L, Punzi L, et al (2012) Biomechanical assessment of balance and posture in subjects with ankylosing spondylitis. J Neuroeng Rehabil 29:63-0003-9-63
Vergara ME, O’Shea FD, Inman RD, Gage WH (2012) Postural control is altered in patients with ankylosing spondylitis. Clin Biomech (Bristol, Avon) 27:334–340
Dagfinrud H, Kvien TK, Hagen KB (2004) Physiotherapy interventions for ankylosing spondylitis. Cochrane Database Syst Rev. 18(4): CD002822. Review. Update in: Cochrane Database Syst Rev. 2008; (1):CD002822
Masiero S, Bonaldo L, Pigatto M, Lo Nigro A, Ramonda R, Punzi L (2011) Rehabilitation treatment in patients with ankylosing spondylitis stabilized with tumor necrosis factor inhibitor therapy: a randomized controlled trial. J Rheumatol 38:1335–1342
Giannotti E, Trainito S, Arioli G, Rucco V, Masiero S (2014) Effects of physical therapy for the management of patients with ankylosing spondylitis in the biological era. Clin Rheumatol 33:1217–1230
Masiero S, Poli P, Bonaldo L, Pigatto M, Ramonda R, Lubrano E et al (2013) Supervised training and home-based rehabilitation in patients with stabilized ankylosing spondylitis on TNF inhibitor treatment: a controlled clinical trial with a 12-month follow-up. Clin Rehabil 28:562–572
Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P, CONSORT Group (2008) Extending the CONSORT statement to randomized trials of non-pharmacologic treatment: explanation and elaboration. Ann Intern Med 148:295–309
Braun J, van den Berg R, Baraliakos X, Boehm H, Burgos-Vargas R, Collantes-Estevez E et al (2011) 2010 Update of the ASAS/EULAR recommendations for the management of ankylosing spondylitis. Ann Rheum Dis 70:896–904
Horak FB, Macpherson JM (1996) Postural orientation and equilibrium. In: Rowell LB, Shepherd JT (eds) Handbook of physiology, section 12, exercise: regulation and integration of multiple systems. American Physiological Society, New York, pp 255–292
Aydog E, Depedibi R, Bal A, Eksioglu E, Unlu E, Cakci A (2006) Dynamic postural balance in ankylosing spondylitis patients. Rheumatology (Oxford) 45:445–448
van der Heijde D, Braun J, Deodhar A, Inman RD, Xu S, Mack ME, Hsu B (2013) Comparison of three enthesitis indices in a multicentre, randomized, placebo-controlled trial of golimumab in ankylosing spondylitis (GO-RAISE). Rheumatology (Oxford) 52:321–325
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest to declare in relation to this work.
Appendix
Rights and permissions
About this article

Cite this article
Demontis, A., Trainito, S., Del Felice, A. et al. Favorable effect of rehabilitation on balance in ankylosing spondylitis: a quasi-randomized controlled clinical trial. Rheumatol Int 36, 333–339 (2016). https://doi.org/10.1007/s00296-015-3399-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-015-3399-6