
Abstract
The aim of this study was to investigate the clinical, radiographic, and magnetic resonance imaging (MRI) findings of temporomandibular joint (TMJ) and masticatory muscles in rheumatoid arthritis (RA) patients. Twenty-eight RA patients and 29 healthy subjects were participated in the study. The patient underwent clinical and laboratory investigation. DAS28 scores were calculated. Lateral panoramic radiography was performed to evaluate condylar erosion and condylar movement. Craniofacial MRI was performed to evaluate TMJ and masseter, medial and lateral pterygoid muscles’ thickness, and cross-sectional area. It was found that the mean maximal interincisal distance, range of lateral, retrusive (P < 0.05) and protrusive motion were all lesser in RA group. Lateral panoramic radiography revealed a distinct erosion in 10.7% (3/28) and restricted condylar movement in 53.6% (15/28) of RA patients. Two RA patients demonstrating marked condylar erosion in lateral panoramic radiographs were RF negative and had DAS28 scores 3.41 and 4.61. MRI findings revealed condylar erosion and effusion in one RA patient and atrophic changes of masticatory muscles in another patient. There was no statistical significance between RA and healthy groups for the thickness and cross-sectional areas of the masticatory muscles. RA group revealed a strong linear relationship for the right and left muscle thickness and cross-sectional areas in regression analysis. TMJ symptoms are frequent findings and thought to be affected from mean disease duration in RA. Laboratory findings should be considered for disease activity–related TMJ involvement. RA patients did not present muscular atrophy or hypertrophy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory systemic disease with an unclear etiology that involves the joints dominantly [1, 2]. RA possesses many clinical features of a systemic disease but abnormalities in synovial structure and function are the primary manifestations [3]. Symmetrical joint alteration is a characteristic feature of this disease [2].
It is well known that RA often involves the temporomandibular joint (TMJ), particularly in its severe form [4–9], and also affects the function of the masticatory system [4, 8]. Reported frequencies of TMJ involvement vary between 2 and 86% [5, 6, 9, 10]. TMJs afflicted with RA may produce pain, swelling, crepitation, stiffness on opening the mouth, and limitation of movement [3, 8, 11]. Magnetic resonance imaging (MRI) that can demonstrate inflammatory changes within the bony and soft tissues of the joint that are not visible on conventional radiographs has become the specific modality in the evaluation of TMJ in RA [2, 11]. The most characteristic radiographic signs of RA in the TMJ are reduced joint space, synovial proliferation resulting in disk deformation, fragmentation, and destruction. Severe destruction of the cortical and subcortical bone can finally lead to almost complete loss of the condyle. Bone sclerosis and osteophytes may also occur [2, 11, 12]. Muscular weakness and atrophy is one of the hallmarks of RA too. These muscular abnormalities can relate to disuse or inflammatory changes [2, 13]. Muscle atrophy is related to a reduction in strength since there is a correlation between strength and cross-sectional area [13].
There is no study that has evaluated the TMJ and masticatory muscles by both clinical and MRI findings in RA patients. The aim of this study was to investigate the effects of RA on TMJ and masticatory muscles by comparing the associations between clinical, radiographic, and MRI findings of the RA patients so as to determine the detectable changes on the stomatognathic system.
Materials and methods
Twenty-eight patients with clinically established RA based on the criteria of the American Rheumatism Association (Mean age of the patients was 44 ± 8.49) and 29 age- and sex-matched control subjects (Mean age of the healthy subjects was 45.75 ± 9.12) over the age of 30 were included in the study. Patients with RA and controls who referred to the Süleyman Demirel Univesity Education and Research Hospital, Division of Rheumatology and Faculty of Dentistry, Oral Diagnosis and Radiology Department for diagnostic examination and treatment were selected. No subjects had any history of diseases affecting the masticatory system. Subjects who could not undergo maxillofacial MRI examination for reasons including acute panic disorder or orthopedic prosthesis were excluded from the study. This controlled, clinical, and radiological study was approved by the Ethics Committee of Süleyman Demirel University, Faculty of Medicine, and all subjects had given written informed consent to their participation in the study.
Clinical examination
Clinical manifestations of the subjects and the use of the relevant medicine were noted. The subjects were evaluated by the same doctor of dentistry. The masticatory system and TMJ of the subjects were examined for each side separately by palpation in a normally equipped dental unit. The temporal, masseter, sternocleidomastoid, medial, and lateral pterygoid muscles were palpated and tenderness or pain of these muscles was recorded. The severity of the subjective symptoms in the masticatory system was determined by the patients according to a 5-point scale (1 = no or minimal discomfort, 2 = slight discomfort, 3 = moderate discomfort, 4 = severe discomfort, and 5 = very severe discomfort) [8].
All subjects were asked whether they had experienced tenderness, pain, swelling, stiffness on opening the mouth, and limitation of movement in the TMJ. Clicking and crepitation sounds of TMJ were noted. The severity of TMJ symptoms of the subjects was assessed on the basis of responses to the question, ‘How would you describe your TMJ symptoms?’ (1 = no discomfort or very minimal discomfort, 2 = mild discomfort, 3 = severe discomfort, and 4 = very severe discomfort). According to this grading system, grade 1 was described as ‘asymptomatic TMJ’ and grades 2–4 were combined and described as ‘severely symptomatic TMJ’. Maximum mouth opening was evaluated by measuring the interincisal distance of maximum opening. The subjects were next instructed to move the mandible laterally, and the extent of lateral excursion measured. Protrusive and retrusive movement were also evaluated in a similar manner. Pain during these movements was recorded. Maximum mouth opening measured less than 40 mm was considered as limited mouth opening. Deviations during mouth opening and closure were also recorded. Parafunctional habits (tooth clenching, tooth grinding, and unilateral mastication) of subjects were questioned.
Clinical and functional evaluation of the RA patients was assessed by the same rheumatologist. Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and rheumatoid factor (RF) levels of RA patients were studied, and DAS28 scores were calculated.
Radiographic examination
The subjects underwent routine panoramic radiographs (OPGs), lateral panoramic radiographs in open and closed mouth positions to evaluate condylar erosion and condylar movement with a Planmeca 2002 CC Proline unit.
Lateral panoramic images were analyzed for the condylar erosion and scored using a scale (0: no erosion, 1: very slight erosion, 2: erosion of top of the condyle, 3: half of the condyle eroded, and 4: condyles completely eroded).
Condylar movements on the lateral panoramic radiograph were recorded and graded as 1: normal joint movement, 2: nearly normal movement, 3: only light movement, and 4: no movement at all.
Craniofacial MRI was performed with a 0.2-T scanner (General Electric Medical System, Signa, USA) to evaluate TMJ and masticatory muscle thickness and area. The subjects were scanned in supine position with the Francfurt horizontal plane was perpendicular to the scan table. The subjects were instructed to hold their teeth together but to avoid clenching in mouth closed position. 5-mm-thick contiguous slices were acquired. Scan specifications were axial T1- and T2-weighed images, sagittal T2, and coronal T1-weighed images of mouth in closed position. Additionally, sagittal T1-weighed scans were acquired in mouth opened position for the subjects with symptomatic TMJ. MRI scans were evaluated by a radiologist without knowledge of clinical data. MRI slices that TMJ could be seen were examined for the morphology of the condyle and articular eminence, discal position, effusion, osteofits, and condylar erosion.
Masseter, medial, and lateral pterygoid muscle thickness and areas were measured on T1-weighed axial images. The thickness and areas of masseter and medial pterygoid muscles were measured at the oropharyngeal level on the sections that the mandibular ramus could be seen and the coronoid process of the mandible had not observed yet. The measurements of the lateral pterygoid muscle were performed at the oropharyngeal level, on the slices that the mandibular condyle could be seen. The areas of the masseter, medial, and lateral pterygoid muscles were calculated by using the Image J (Version 1.40 g, National Institutes of Health, USA) program for the right and left sides on the slices that the muscle thickness was measured after the outlines of these muscles were drawn on an acetate paper and digitalized.
Statistical analysis
Examinations of categorical parameters according to prevalence’s were evaluated using the χ2 test and presented with frequencies. Interval and ratio scale variables were evaluated with independent samples t-test and expressed as means and standard deviations. Mann–Whitney U test was used for comparisons of the properties between the RA and control groups that the ranges were not distributed normally. Regression analyis was used to detect whether the relationship is significant or not between muscle thickness and cross-sectional area.
Results
The characteristics of subjects are shown in Table 1. RA patients were between the ages of 30–61, while control subjects were 30–56. Disease duration of RA patients was changing between 2 and 20 years. 17 (60.71%) of RA patients had positive RF. Eight (28.57%) of RA patients were with high ESR and 15 (53.57%) of RA patients were with high CRP levels. RF level was between 10 and 620 IU/ml, ESR level was between 5 and 40 m/h, and the CRP level was between 3 and 173 mg/l. In RA patients, no one was in the remission period while three had low, 24 had medium, and one patient had high disease activity according to DAS28 score.
Subjective and clinical parameters
Values for maximal mouth opening, lateral, retrusive, and protrusive motion were all found less in RA group. Limited mouth opening was detected in three subjects in control group and six in RA patients. There was statistically significant difference between the RA and control groups for the mean value of retrusion (Table 2).
Distribution of the number of TMJ symptoms in RA and control groups was demonstrated in Table 3. There were no subjects with TMJ swelling.
TMJ with severe discomfort was reported significantly most often in RA group than in the control group (P < 0.05).
Tooth grinding, tooth clenching, and unilateral chewing habits were determined among the subjects. Tooth grinding was most often reported in control group (15/29, 51.7%) while chewing with right was most often in RA group (11/29, 37.9%). There were no subjects reported parafunctional habits with very severe TMJ discomfort.
RA group estimated the subjective symptoms in the masticatory system was significantly worse than the control group (P = 0.026).
Statistically significant difference was found between the RA and control groups for the pain on palpation of the left masseter muscle (P = 0.010) and right medial pterygoid muscle (P = 0.036).
Radiographic findings
Lateral panoramic radiography revealed a distinct erosion in 10.7%(3/28) and restricted condylar movement in 53.5%(15/28) of RA patients while very slight erosion was observed in right condyle only for one subject in control group. Severe erosion in two right and two left condyles in RA group (Table 4). There were no significant differences found for condylar erosion and for the condylar movement of right and left TMJ in lateral panoramic radiography between the RA and control groups. Examples of condylar erosion and restricted condylar movement in lateral panoramic radiography are provided in Fig. 1.

Cropped lateral panoramic radiograph demonstrating condylar erosion and restricted condylar movement in a: right condyle mouth close, b: right condyle mouth open, c: left condyle mouth close, and d: left condyle mouth open positions
There were no significant differences found between the condylar erosion in lateral panoramic radiographs and the mean DAS28 score, ESR, and CRP levels in RA group. There was one RA patient with marked erosion in both right and left condyle with negative RF and DAS28 score = 3.41 while another RA patient with negative RF and DAS28 score = 4.61 showing marked erosion in only left condyle in lateral panoramic radiographs.
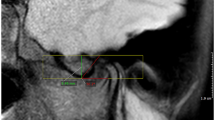
MRI findings of the TMJ are shown in Table 5. Disk displacement occurred in both RA and control groups but most frequently in RA patients (3/28, 10.7%). Degeneration of disk, joint effusion, and erosion of condyle was not observed in control group. Atrophic changes and high intensity with fatty degeneration on masticatory muscles were observed only in one RA patient on MRI (Fig. 2).

Cropped spin echo T2-weighed axial MRI slice demonstrating fatty atrophic changes (arrow) on lateral pterygoid muscle of a RA patient
The mean cross-sectional area and the mean thickness measurements of masseter, lateral pterygoid, and medial pterygoid muscles on MRI slices are shown in Table 6. Significant difference was not found for the mean cross-sectional area and the mean thickness of these muscles between RA and control groups.
Regression analyses were performed for the muscle thickness and cross-sectional area of the right and left masseter, medial pterygoid, and lateral pterygoid muscles for RA and control group. RA group revealed a strong linear relationship for the right and left muscle thickness of masseter (linear y = −0.341 + 1.061x; R 2 = 0.645), medial pterygoid (linear y = 2.947 + 0.693x; R 2 = 0.600), and lateral pterygoid muscles (linear y = 2.202 + 0.803x; R 2 = 0.707). Also, control group revealed a linear relationship for the right and left muscle thickness of masseter (linear y = 0.118 + 1.036x; R 2 = 0.621), medial pterygoid (linear y = 2.316 + 0.837x; R 2 = 0.623), and lateral pterygoid muscles (linear y = 1.194 + 0.911x; R 2 = 0.835) (Fig. 3).

Estimation of linear regression equation between right and left muscle thickness for the lateral pterygoid muscle in control group
Masseter, medial pterygoid, and lateral pterygoid muscle cross-sectional areas for right and left side were analyzed with regression analysis for RA patients, and a strong linear relationship was detected for masseter (linear y = 1,777 + 0.869x; R 2 = 0.680) (Fig. 4), lateral pterygoid (linear y = 3,971 + 0.554x; R 2 = 0.519), and medial pterygoid (linear y = 2,708 + 0.532x; R 2 = 0.501) muscles. Control group revealed a strong linear relationship for the cross-sectional area of the right and left lateral pterygoid (linear y = 884.1 + 0.988x; R 2 = 0.548) muscle while right and left medial pterygoid (linear y = 2,228 + 0.670x; R 2 = 0.464) and masseter (linear y = 5,050 + 0.596x; R 2 = 0.431) muscle revealed a less strong linear relationship.

Estimation of linear regression equation between right and left cross-sectional area for the masseter muscle in RA group
Discussion
The effects of systemic diseases on oral and surrounding tissues are calling the investigators’ attention. Thus, the researches about the effects of RA on stomatognathic system are increasingly continuing. With the aim of determining the changes in the masticatory muscles and TMJ in RA patients, we thought to evaluate these structures together that are collaborating in masticatory system.
We found the sensitivity (P < 0.05), pain (P < 0.01), morning stiffness (P < 0.05), and clicking (P < 0.05) of the right and left TMJ on palpation significantly more in RA patients. RA patients exhibited more severe TMJ symptoms than the matched controls, and this finding was in agreement with the results reported by Helenius et al. [14]. The number (9/28, 32.14%) of RA patients with severe TMJ symptoms was found lower than the number (16/28, 57.14%) of RA patients with no or minimal TMJ discomfort. However, lateral panoramic radiography revealed distinct erosion for three (10.7%) of RA patients with no or minimal TMJ discomfort. Despite the radiographic findings of erosion, most of the RA patients had no or minimal discomfort and it was understood that TMJ-related problems had remained clinically silent. Subjective TMJ discomfort or complaints should be overshadowed by other joint problems elsewhere in the body [6, 9]. TMJ is structurally different from other joints. It has special retrodiscal tissue that is rich in blood vessels, which may act as a highly efficient drainage system for joint exudates. In this manner, joint swelling and pain may be alleviated or even prevented. In our study, there were no subjects with TMJ swelling. TMJ’s special articular disk structure, which divides the TMJ two distinct cavities, may also another cause for reduced self-awareness of TMJ problems among RA patients.
The duration of RA especially 5 years or more is thought to be another factor affecting the severity of TMJ involvement [7, 9, 15]. In our study, the mean disease duration of RA was found to be 5.78 ± 0.89 years, and 28.57% of RA patients with symptomatic TMJ involvement were having disease for more than 5 years.
Early diagnosis and treatment reduce joint destruction, preserve function, and improve survival [16]. It was reported that early referral and treatment especially in the first 3 months might be the most important ‘joint protecting’ measure for patients with RA [17]. RA patients in our study were treated medically and controlled regularly in rheumatology department. Marked condylar erosion was determined only in three patients, and their disease duration was more than 5 years. The number of patients with TMJ involvement in RA group was more than the control group but the severity of TMJ involvement is thought to be reduced with the effect of regular treatment.
We found the values for maximal mouth opening, retrusion, protrusion, and laterotrusion were lower in RA patients than in control subjects as the previous studies reported [4, 14, 18]. However, only the retrusion value was significantly lower in RA group.
Parafunctional habits of RA patients with severe TMJ involvement were tooth clenching, tooth grinding, and unilateral masticatory habits in our study. Kobs et al. [19] found a statistically significant relationship between the incidence of “clenching” and muscle palpation findings, as well as between sensitivity in the mandibular joints with positive muscle palpation findings. We found that left TMJ clicking and left masseter muscle pain on palpation were significantly different between the RA and control groups. This is suggested to be due to the left TMJ involvement in RA, and related masseter muscle pain should be increased with the effect of mastication only with left side. Previous reports [14, 20, 21] revealed that masticatory muscle pain was more frequent in RA patients. These findings are compatible with our results but differently in this study, the masticatory muscles were investigated as right and left sides. It has been suggested that compression of retrodiscal tissue may be the cause of such pain. Other suggested causes are inflammatory change secondary to internal derangement, stretching of the joint capsule, and synovitis [14, 21].
Kallenberg et al. [8] compared the patients with RA and temporomandibular disorders by a subjective dysfunction score and found that the patients with temporomandibular disorders estimated their subjective symptoms significantly worse than the RA group. We found that the severity of symptoms of the stomatognathic system in RA patients was significantly worse than that of the control group. This difference between the results is because their control group is formed by the patients with temporomandibular disorders.
The relationship between the chronic inflammation and joint damage has been widely established. The level of RF, ESR, CRP, trombocyte count, and plasma tumor necrosis factor-α have all been reported to correlate with the severity of TMD [7, 9, 16, 22–24]. In our study, the majority of RA patients were RF + (60.71%) and 28.57% were with high ESR and 53.57% were with high CRP levels. However, the patients with condylar erosions were all had negative RF. The disease durations of all were more than 5 years. The disease duration is thought to be one of the major determinants of erosions. And, anti-CCP positivity is also a known risk factor. However, we could not be able to detect anti-CCP levels.
Different imaging techniques may be used for TMJ evaluation. In the present study, it is thought that the effects of RA on stomatognathic system should be evaluated accurately with the symptoms and radiographic interpretation, and consequently, the panoramic, lateral panoramic, and MRI screening were performed to evaluate both TMJ and masticatory muscles. Although we faced with some problems evaluating the TMJ because of screening with a 0.2-T MRI system and not using a TMJ coil, TMJ involvement in RA was found to be more frequent and the masticatory muscles could be evaluated well. RA patients revealed disk displacement, degeneration of disk, joint effusion, and erosion of the condyle while in control group, only disk displacement was detected. Atrophic changes with fatty degeneration in masticatory muscles are detected in one RA patient examined by MRI.
Previous studies evaluated muscle function in the stomatognathic system by determining maximum bite force [25], sectional area [26–28], thickness [29], and volume [28] of the muscles. In this study, the thickness and sectional area measurement of digital images of masseter, lateral pterygoid, and medial pterygoid muscles were obtained by MRI axial sections and no statistical difference was found between the RA and control groups for the muscle thickness and area. The mean sectional area of masseter muscle was found larger than the medial pterygoid muscle as in related articles [30–32]. Goto et al. [27] found the sectional area in jaw-close position, respectively, as masseter, lateral pterygoid, and medial pterygoid muscle from larger to smaller.
A comparison of the right and left muscles did not reveal any statistical difference in sectional area as Goto et al. [27] reported. This is thought to represent the symmetry of right and left muscles in our study groups.
In conclusion, TMJ symptoms such as pain, tenderness, morning stiffness, and clinical findings such as limited mandibular function, masticatory muscle pain, and TMJ clicking were frequent clinical findings in RA patients. TMJ symptoms were thought to be affected from the mean disease duration time in RA. Also, laboratory findings should be considered for disease activity and related TMJ involvement. The results of muscle thickness and area measurements in our study did not suggest muscular atrophy or hypertrophy in RA patients when compared with control group. Clinical and radiological follow-up of RA patients with TMJ and masticatory muscle complaints is essential. Early diagnosis of TMJ changes can provide better treatment planning. Rheumatologists and dental specialists should consult the patient for TMJ and stomatognathic system complaints as to diagnose and determine effective therapeutic strategies for TMJ involvement. Further studies are needed to study the TMJ and masticatory muscle involvement in RA with larger study groups.
References
Akil M, Veerapen K (2004) Rheumatoid arthritis: clinical features and diagnosis. In: Snaith ML (ed) ABC of rheumatology, 3rd edn. BMJ Publishing, London, pp 50–60
Resnick D (2002) Diagnosis of bone and joint disorders, vol 2, 4th edn. Saunders, Philadelphia
Klippel JH, Dieppe PA (2000) Rheumatology, vol 1, section 5, 2nd edn. Mosby, London
Tegelberg A, Kopp S (1987) Clinical findings in the stomatognathic system for individuals with rheumatoid arthritis and osteoarthrosis. Acta Odontol Scand 45:65–75
Larheim TA, Smith HJ, Aspestrand F (1990) Rheumatic disease of the temporomandibular joint: MR imaging and tomographic manifestations. Radiology 175:527–531
Goupille P, Fouquet B, Cotty P, Goga D, Mateu J, Valat JP (1990) The temporomandibular joint in rheumatoid arthritis: correlations between clinical and computed tomography features. J Rheumatol 17:1285–1291
Celiker R, Eryilmaz M, Gökce-Kutsal Y (1995) Temporomandibular joint involvement in rheumatoid arthritis. Relationship with disease activity. Scand J Rheumatol 24:22–25
Kallenberg A, Wenneberg B, Carlsson GE, Ahlmen M (1997) Reported symptoms from the masticatory system and general well-being in rheumatoid arthritis. J Oral Rehabil 24:342–349
Lin YC, Hsu ML, Yang JS, Liang TH, Chou SL, Lin HY (2007) Temporomandibular joint disorders in patients with rheumatoid arthritis. J Chin Med Assoc 70:527–534
Helenius LM, Tervahartiala P, Helenius I, Al-Sukhun J, Kivisaari L, Suuronen R et al (2006) Clinical, radiographic and MRI findings of the temporomandibular joint in patients with different rheumatic diseases. Int J Oral Maxillofac Surg 35:983–989
Narváez JA, Narváez J, Roca Y, Aguilera C (2002) MR imaging assessment of clinical problems in rheumatoid arthritis. Eur Radiol 12:1819–1828
Raustia AM, Pyhtinen J (1991) Computed tomography of the masticatory system in rheumatoid arthritis. J Rheumatol 18:1143–1149
Herbison GJ, Ditunno JF, Jaweed MM (1987) Muscle atrophy in rheumatoid arthritis. J Rheumatol 14:78–81
Helenius LM, Hallikainen D, Helenius I, Meurman JH, Könönen M, Leirisalo-Repo M et al (2005) Clinical and radiographic findings of the temporomandibular joint in patients with various rheumatic diseases. A case-control study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 99:455–463
Ogus H (1975) Rheumatoid arthritis of the temporomandibular joint. Br J Oral Surg 12:275–284
Shovman O, Gilburd B, Zandman-Goddard G, Sherer Y, Orbach H, Gerli R et al (2005) The diagnostic utility of anti-cyclic citrullinated peptide antibodies, matrix metalloproteinase-3, rheumatoid factor, erythrocyte sedimentation rate, and C-reactive protein in patients with erosive and non-erosive rheumatoid arthritis. Clin Dev Immunol 12:197–202
Nell VP, Machold KP, Eberl G, Stamm TA, Uffmann M, Smolen JS (2004) Benefit of very early referral and very early therapy with disease-modifying anti-rheumatic drugs in patients with early rheumatoid arthritis. Rheumatology 43:906–914
Ardic F, Gokharman D, Atsu S, Güner S, Yilmaz M, Yorgancioglu R (2006) The comprehensive evaluation of temporomandibular disorders seen in rheumatoid arthritis. Aust Dent J 51:23–28
Kobs G, Bernhardt O, Kocher T, Meyer G (2005) Oral Parafunctions and positive clinical examination findings. Stomatol Baltic Dental Maxillofac J 7:81–83
Ettalo-Ylitalo UM, Syrjänen S, Halonen P (1987) Functional disturbances of the masticatory system related to temporomandibular joint involvement by rheumatoid arthritis. J Oral Rehabil 14:415–427
Könönen M, Wenneberg B, Kallenberg A (1992) Craniomandibular disorders in rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis. A clinical study. Acta Odontol Scand 50:281–287
Voog Ü, Alstergren P, Eliasson S, Leibur E, Kallikorm R, Kopp S (2003) Inflammatory mediators and radiographic changes in temporomandibular joints of patients with rheumatoid arthritis. Acta Odontol Scand 61:57–64
Nordahl S, Alstergren P, Eliasson S, Kopp S (2001) Radiographic signs of bonedestruction in the arthritic temporomandibular joint with special reference to markers of disease activity: a longitudinal study. Rheumatology 40:691–694
Plant MJ, Williams AL, O’Sullivan MM, Lewis PA, Coles EC, Jessop JD (2000) Relationship between time-ıntegrated C-reactive protein levels and radiologic progression ın patients with rheumatoid arthritis. Arthritis Rheum 43:1473–1477
Sasaki K, Hannam AG, Wood WW (1989) Relationships between the sizes, position and angulation of human jaw muscles and unilateral first molar bite force. J Dent Res 68:499–503
van Spronsen PH, Weijs WA, Valk J, Prahl-Andersen B, van Ginkel FC (1989) Comparison of jaw- muscle bite-force cross-sections obtained by means of magnetic resonance imaging and high-resolution CT scanning. J Dent Res 68:1765–1770
Goto TK, Yahagi M, Nakamura Y, Tokumori K, Langenbach GE, Yoshiura K (2005) In vivo cross-sectional area of human jaw muscles varies with section location and jaw position. J Dent Res 84:570–575
Goto TK, Nishida S, Yahagi M, Langenbach GE, Nakamura Y, Tokumori K et al (2006) Size and orientation of masticatory muscles in patients with mandibular laterognathism. J Dent Res 85:552–556
Kubota M, Nakano H, Sanjo I, Satoh K, Sanjo T, Kamegai T et al (1998) Maxillofacial morphology and masseter muscle thickness in adults. Eur J Orthod 20:535–542
Gionhaku N, Lowe AA (1989) Relationship between jaw muscle volume and craniofacial form. J Dent Res 68:805–809
Boom HP, van Spronsen PH, van Ginkel FC, van Schijndel RA, Castelijns JA, Tuinzing DB (2008) A comparison of human jaw muscle cross-sectional area and volume in long- and short-face subjects, using MRI. Arch Oral Biol 53:273–281
Hsu CW, Shiau YY, Chen CM, Chen KC, Liu HM (2001) Measurement of the size and orientation of human masseter and medial pterygoid muscles. Proc Natl Sci Counc Repub China B 25:45–49
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yilmaz, H.H., Yildirim, D., Ugan, Y. et al. Clinical and magnetic resonance imaging findings of the temporomandibular joint and masticatory muscles in patients with rheumatoid arthritis. Rheumatol Int 32, 1171–1178 (2012). https://doi.org/10.1007/s00296-010-1743-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-010-1743-4