
Abstract
The objective of this study was to estimate the unit costs of non-vertebral osteoporotic fractures in five European countries based on the results of the SOTI and TROPOS clinical trials in postmenopausal osteoporotic women. The information recorded in the Case Report Forms was used. The perspective of third party payers was adopted. Hip fracture unit cost was the highest. The ranges of costs among countries was narrow for hip from 8,346€ (Italy) to 9,907€ (France), but wider for other fractures: 890€ (Spain) to 2,022€ (Italy) for wrist, 1,167€ (Spain) to 3,268€ (Italy) for pelvis, 837€ (Spain) to 2,116€ (Italy) for sternum/clavicle, 565€ (Spain) to 908€ (France) for rib, 1,518€ (Spain) to 3,651€ (Belgium) for humerus, 1,805€ (Spain) to 3,521€ (Italy) for leg. The costs of those fractures should be considered when estimating the cost of osteoporosis.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is characterized by low bone mass and microarchitectural deterioration of bone structure, resulting in bone fragility and increased susceptibility to fracture [1]. Osteoporosis in postmenopausal Caucasian women is defined as a value for bone mineral density (BMD) more than 2.5 standard deviations below the young average value. The diagnostic threshold identifies approximately 15–20% of postmenopausal women as having osteoporosis when measurements using dual-energy X-ray absorptiometry are made at the spine or the hip [2]. Lifetime risk of any osteoporotic fracture is very high and lies within the range of 40–50% in women and 13–22% for men [3]. In Malmo (Sweden) lifetime risk of forearm, hip and spine fracture were 21.5, 23.3 and 15.4%, respectively, in women at the age of 45 years and corresponding values for men were 5.2, 11.2 and 8.6% [4]. It was estimated in 1990 that approximately 1.7 million hip fractures occurred throughout the world [5]. As the population is becoming older especially in developed countries, this number is projected to increase almost sixfold from 1995 to 2050 [6].
The introduction of new osteoporosis treatments raises the possibility of fracture prevention, but the economic implications are uncertain because the potential patient population is very large [7]. Due to the increasing costs of medical care, health authorities are now looking at new methods whereby health budgets can be spent most effectively and made more accountable [8]. Until the burden of illness to society can be clearly established, it is difficult to determine priorities in the effective allocation of the resources for health care and prevention. Efforts to devise cost-effective strategies for the use of the treatments of osteoporosis have been hampered by the paucity of detailed data on fracture costs [9, 10]. There have been a few reports on direct medical costs for hip fractures, fewer yet on vertebral and distal forearm fractures, and only one to our knowledge on the other fractures related to osteoporosis [11, 12].
The aim of this study was to estimate the unit costs of non-vertebral osteoporotic fractures in 5 countries: France, UK, Spain, Italy and Belgium by combining the data issued from two clinical trials [13–16] and external data extracted from validated database.
Material and methods
Sources and selection of data
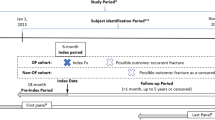
SOTI and TROPOS were two prospective, randomized, double-blind clinical phase 3 trials comparing, in two parallel groups, the daily oral dose of 2 g of strontium ranelate with placebo, the patients of both groups receiving calcium and vitamin D according to their own deficiencies [13, 14]. The main objective of SOTI and TROPOS was to demonstrate a reduction in the incidence of postmenopausal women experiencing a new osteoporotic fracture (vertebral fracture in SOTI and non-vertebral fracture in TROPOS) with a main analysis over a 3-year treatment period. Both trials assessed the incidence of non-vertebral fractures (secondary endpoint in SOTI). One of the secondary objectives was to provide data regarding the management of non-vertebral osteoporotic fractures in order to subsequently estimate the costs. In SOTI, 1,649 women above 50 years of age were enrolled with at least one osteoporotic vertebral fracture at inclusion and a lumbar BMD ≤ 0.840 g/cm2. In TROPOS 5,091 women with or without prevalent vertebral fractures above 70 years of age with a femoral neck BMD ≤ 0.600 g/cm2 were enrolled. In both trials, the first follow-up visit took place at 3 months, then at 6 months, and the subsequent visits were scheduled every 6 months. Twelve countries participated to these studies.
Among those, we selected five countries which had reported data for at least 50 non-vertebral fractures. A total number of 4,483 patients and 633 osteoporotic fractures were included as follows: Italy (1,061 patients and 102 fractures), UK (1,034 patients and 112 fractures), Belgium (947 patients and 185 fractures), France (887 patients and 179 fractures), and Spain (554 patients and 55 fractures).
Model of direct cost estimation of fractures
The resource utilization data recorded in the case report forms (CRFs) on non-vertebral osteoporotic fractures were the following: surgical treatment (except prosthesis) and the procedure used (pin, screw, plate), prosthesis, orthopaedic treatments, immobilisation of the fracture by cast or splint, length of hospitalisation and length of rehabilitation treatment (at home and in specialized institutions).
The inpatient costs were estimated based on local costs per disease related group (DRG) (France, UK, Spain, Italy), or average costs of hospitalisation per day in orthopaedic services for all diagnoses combined (Belgium). Sources for the cost estimates are the following:
- Belgium:
-
Institut National d’Assurance Maladie-Invalidité (INAMI), Nomenclature des Prestations de Santé, Bruxelles.
- Spain:
-
SOIKOS, Centro de Estudios de Economía de la Salud y Política Social, Base de Datos de Costes Sanitarios, Versión 1.4.
- :
-
COCHTA A guidance document for the costing process. Version 1.0. 1996.
- Italy:
-
Ministry of Health. Aggiornamento delle tariffe delle prestazioni di assistenza ospedaliera di cui al DM 14.12.1994; DM 30.6.97 SO GU n° 209 8.9.1997, Allegato II.
- :
-
Ministry of Health. DM 22 luglio 1996. Prestazioni di assistenza specialistica ambulatoriale erogabili nell’ambito del SSN e relative tariffe GU n 216 of 14/11/1996: DM of 22/07/1996.
- UK:
-
NHS Reference Costs, 2001. CIPFA/HFM, 2001. PSSRU, 2001.
- :
-
The Chartered Institute of Public Finance and Accountancy (CIPFA), The Health Service Database 2001 (Financial Year 2000–2001), CIPFA/HFM, IPF, London.
- France:
-
Nomenclature des actes médicaux (Caisse Nationale d’Assurance Maladie) http://www.ameli.fr
- :
-
Programme de médicalisation des systémes d’information (PMSI) 2001. http://www.atih.sante.fr
When detailed information were not available, assumptions were made in order to estimate the costs (e.g., with regard to the number of visits, X-rays, etc.):
-
In case of hospitalisation, we assumed a standard management comprising three outpatient follow-up consultations and three imaging procedures in all countries considered here.
-
In absence of hospitalisation, we assumed that the standard management included four outpatient visits and four imaging procedures. Finally, all patients with non-hospitalised fractures were assumed to have immobilisation with a cast or splint.
Standard cost of the initial management of fractures
We defined three categories of initial management (prior to rehabilitation): orthopaedic treatment with hospitalisation, surgical treatment with hospitalisation, ambulatory treatment.
It was not possible to estimate the frequency of treatment options for each country and fracture locations separately. This was the case since the number of parameters to be estimated was quite large (5 countries × 7 fracture locations × 3 types of initial management = 105) in relation to the total number of observed fractures in both trials (N = 633). Sample sizes were often too small to allow sufficiently accurate estimates. In particular, certain categories had no observations at all.
In order to define clusters of fractures initial management, we used a logistic regression analysis. This was done in two steps. First, we estimated a logistic regression model with the odds of hospitalisations as the outcome variable and binary predictive variables for country and fracture location. For this analysis, France was the country of reference and forearm fractures was the reference location. This analysis allowed us to regroup countries and fracture locations that did not have statistically significant differences in their odds of hospitalisations. In order to minimize the possibility of regrouping country and fracture locations with different odds of hospitalisation we fixed the α (type I error) at 0.20.
A similar approach using logistic regression analysis was also used to regroup countries and fracture locations that had sufficiently similar odds for surgery.
For example, if the odds ratio (OR) of hospitalisation in Belgium compared with France was not significantly different from 1 (P > 0.20), we assumed that the proportion of patients hospitalised for a fracture was similar for both countries.
Rehabilitation standard cost
For estimating the average length of rehabilitation, we used the mean value of the whole sample, given the small variability across countries and the small numbers of patients observed. For the same reason, the clavicle/sternum, pelvic and ribs fractures have been grouped to estimate the average length of rehabilitation. In the CRF, data on rehabilitation services at home were given in terms of number of weeks of rehabilitation. However, costing these services required information on the number of sessions. We therefore made the assumption that a week of rehabilitation was equivalent with two sessions of physical therapy.
Fracture locations
The fracture locations in the trials were regrouped into seven categories: pelvic fractures (sacrum, pelvis), rib, humerus, wrist (distal forearm), clavicle/sternum, hip (femoral neck or trochanteric), leg (tibia, fibula and femur except hip). Fingers, toes and ankle fractures have been considered as non-osteoporotic but traumatic.
Perspective
The health insurance (third-party payer) perspective was primarily adopted in this study and we limited the costs considered to direct medical costs.
A tentative estimate of corresponding societal costs was also provided. We assumed that the Organisation for Economic Co-operation and Development (OECD) ratio of public expenditure on health on the total expenditure in each country [17] could be applied to our fracture cost estimates.
Currencies
The results are provided in Euros for the year 2002. For UK, we used an exchange rate of 0.7055 pounds for 1 Euro.
Sensitivity analysis
We conducted a sensitivity analysis by varying two types of parameters:
-
1.
The estimated proportions of fractures treated in an outpatient setting, hospitalised without surgery, and hospitalised with surgical intervention; In order to assess the maximum impact of such variations, we considered the following two extreme cases:
-
Minimum costs: the proportion of fractures treated in an outpatient setting is equal to the upper bound of the 95% confidence interval and among the hospitalised fractures, the proportion of those with surgical intervention is the lower bound of the 95% confidence interval;
-
Maximum costs: the proportion of fractures managed in an outpatient setting is the lower bound of the 95% confidence interval and among the hospitalised fractures, the proportion of those with surgical intervention is the upper bound of the 95% confidence interval.
-
-
2.
The unit costs of fractures were varied by ± 10%.
Results
For the five selected countries a total of 533 women with a mean age of 77 years, experienced at least one fracture: 132 (mean age 71 years) included in the SOTI trial and 401 (mean age 78 years) included in the TROPOS trial. Among those 533 women, 633 fractures were observed (i.e. 1.19 fractures per woman): 156 in the SOTI trial (1.18 fractures per woman) and 477 in the TROPOS trial (1.19 fractures per woman).
Among those 633 fractures, the most frequent were those of the hip (N = 159) and wrist (N = 147), followed by fractures of the humerus (N = 102), ribs (N = 91), pelvis (N = 64), leg (tibia, fibula and femur except hip) (N = 48), and clavicle/sternum (N = 22). The total number of fractures observed in Belgium was 185, in France 179, in UK 112, in Italy 102 and in Spain 55.
Logistic regression analyses
Proportion of fractures treated with hospitalisation
For the purpose of this analysis, the reference group for country was France and for the fracture location, wrist fractures.
Based on the logistic regression analyses, two clusters of countries could be distinguished:
-
France (reference group), Belgium (OR = 1.2), Italy (OR = 0.6) and UK (OR = 1.2), for which the odds ratios for hospitalisation were not significantly different from one another;
-
Spain where the proportion of fractures treated with hospitalisation was lower (OR = 0.3).
With regard to fracture locations and compared to wrist fractures (reference group), results showed that differences of hospitalisation for the following fracture locations were not significant: pelvis (OR = 1.2), humerus (OR = 1.2) and leg (OR = 1.4).
In contrast, hip fractures were all treated with hospitalisation and fractures of the wrist and those of the clavicle/sternum (OR = 0.4) and of the ribs (OR = 0.4) were less frequently hospitalised as compared with those of the wrist.
Proportion of surgical interventions in patients hospitalised
Among patients hospitalised for their fractures, the proportion of fractures that had surgical interventions was not significantly different in the following countries: France, Belgium, Italy and Spain.
Compared to France, UK had a lower proportion of fractures treated with surgical interventions.
For fractures treated in an inpatient setting, the proportions of fractures operated were similar for the following locations: wrist, humerus, leg. Hip fractures were more frequently operated than wrist fractures and pelvis and clavicle/sternum were less frequently operated. None of the ribs fractures were operated.
Estimation of combined results (country and fracture locations)
Table 1 shows the proportion of patients treated with hospitalisation and surgery as estimated.
As we saw above, the logistic regression concluded that the rates of fractures not hospitalised, hospitalised without surgery and hospitalised with surgery were not significantly different in the following countries: France, Italy and Belgium. Therefore, those three countries have been pooled. For the same reason, estimates of the rates of fractures hospitalised versus not hospitalised in UK was also grouped with those three countries and the rate of fractures hospitalised and having a surgical procedure versus no surgical procedure in Spain were pooled with the three countries.
For hip fracture, we used the crude (unweighted) estimates, which could be considered reliable given the larger number of observations. The management of this fracture was very similar across countries with more than 90% of them treated with surgery.
Duration of rehabilitation
Table 2 shows the duration of rehabilitation in specialised centres and at home.
The highest lengths of stay in specialised centres were observed for hip fractures (20.6 days) and leg (17.2 days). Average length of stay in specialised centres was substantially lower for other fractures: 11.6 days for humerus fractures, 5.2 days for ribs, pelvis and clavicle/sternum fractures and 4.2 days for wrist fractures.
On the other hand, duration of rehabilitation at home was longer for fractures of the upper limbs, and shorter for the lower limbs.
Costing
Inpatient care
Table 3 shows the unit costs of hospitalisation based on external data sources in each country. The groupings of localisations for unit costs estimates were made according to the available data in each country.
Costs were higher for fractures that underwent surgical interventions as compared with those without surgery. In correlation with the severity of the clinical events, cost of hip fractures were substantially higher than cost of other fractures in all countries and for all types of management except those without surgery for Belgium.
The least costly fractures were those of the ribs. However, costs varied substantially by country and type of management.
Rehabilitation
Table 4 shows costs of rehabilitation for different types of fractures in each country.
The highest costs were observed for hip fractures, followed by those of the leg and the humerus. The lowest costs were observed for fractures of the wrist. According to the countries highest costs are observed in Italy and UK, followed by Spain, France and Belgium.
Total direct costs by fracture
Using the above estimates of cost elements, we estimated the total costs of management for different fracture locations.
Contrasted direct (medical) costs were found according to the category of fractures (Table 5). Hip fracture cost was the highest followed by leg, humerus and pelvis. Cost of wrist, clavicle/sternum and rib fractures were much lower (except wrist fractures for UK). In the five countries, cost varied substantially by country except hip fracture for which costs varied relatively little:
-
Wrist: 890€ (Spain) to 2,022€ (Italy);
-
Clavicle/sternum: 837€ (Spain) to 2,116€ (Italy);
-
Pelvis: 1,167€ (Spain) to 3,268€ (Italy);
-
Hip: 8,346€ (Italy) to 9,907€ (France);
-
Rib: 565€ (Spain) to 908€ (France);
-
Humerus: 1,518€ (Spain) to 3,651€ (Belgium);
-
Leg: 1,805€ (Spain) to 3,521€ (Italy).
Our study was focused on the third party payer perspective. However, rough estimates of the societal cost can be calculated on the basis of the ratios of the public expenditure on the total expenditure for health provided by the OECD [17]. This proportion varies according to the countries: 71.2% (Belgium), 71.4% (Spain), 75.6% (Italy), 76.0% (France) and 83.4% (UK). The results are displayed in Table 6.
Breakdown of fracture costs according to resources are presented for illustration in Fig. 1 for Italy.

Mean unit direct medical costs of fractures in Italy (Euro-2002): breakdown according to care categories
The mean unit cost associated with rehabilitation was often higher than inpatient care: for example, it represented around 59% for hip fractures.
Sensitivity analysis
Table 7 shows the results of sensitivity analyses for the five countries. Substantial variations in the range of 50% concerned fractures of the ribs and clavicle/sternum. They were due to the limited sample size for these fractures which resulted in wider confidence intervals in the proportion of fractures hospitalised or having a surgical intervention.
Variations in the costs of other fracture locations were of a lower magnitude, about 30% (wrist, humerus, leg, hip). The lowest magnitude of variation was observed for hip fractures.
Discussion
To our knowledge, this is the first study estimating the cost of fractures other than vertebral, hip, wrist, especially in Spain, and in Italy and Belgium where published data are restricted to hip fractures. In most studies, the fractures associated with osteoporosis were generally restricted to hip, wrist and vertebral fracture [18].
Our estimates were based on data collected in clinical trials, they might concern a selected subgroup of women meeting the inclusion criteria, i.e. women with at least one osteoporotic vertebral fracture and a lumbar BMD ≤ 0.840 g/cm2 (SOTI) or a femoral neck BMD ≤ 0.600 g/cm2 (TROPOS) and above 50 (SOTI) or 70 years old (TROPOS). However, these characteristics apply to most women who have access to antiosteoporotic treatments. Several studies demonstrated that only limited differences characterise osteoporotic fracture costs as compared to non-osteoporotic [19].
The sample size of the groups enrolled in each country with a specific type of fracture was sometimes also limited, which could bring a lack of precision. The utilization of a logistic regression model to determine clusters of combined variables (countries, fracture, location and type of management) allowed to increase the precision of our estimates.
The information on the resources used for fractures medical management was limited to hospitalisation and rehabilitation. Therefore, we used assumptions about outpatient care (consultations and imaging) as usually done in other studies [19, 20]. This approach was justified because hospitalisation, surgery and rehabilitation are recognized as the major drivers of fractures cost [21–24].
We only took into account the initial phase of the medical management. This excluded the re-hospitalisations and nursing home stays. Most studies on cost of hip fractures conducted in Europe have also focused on the phase of the acute care [19, 22, 24–33]. Only few authors have measured all resources consumed in the following year after the occurrence of the fracture [34–39]. According to these studies, the additional costs represented 34–73% of the initial management cost.
As indirect costs (productivity losses) associated with fractures are minor given the age of the patient population, we limited the costs considered to direct costs, in line with most published studies (Table 8).
Ideally, studies should be conducted from a societal perspective. Because of data constraints, the health insurance (third-party payer) perspective was adopted in this study. In other words, the direct costs included were those reimbursed in the different health systems. A tentative approach of the societal cost estimate used the ratio of health public expenditure on the total health expenditures for the different countries [17]. The results rely on the assumption that this proportion is relevant for fracture costs, which is questionable. Actually, as fracture management costs include for a large part inpatient care, our results are probably underestimated.
International comparisons of costs are difficult because of the different organisation of health care within countries. Despite this limitation, our estimates were in the same order of magnitude in the different countries.
We compared our results to similar published data, which raised problems of heterogeneity in methods and perspectives, survival for example in the year after the fracture was considered in some studies but not in others.
The cost attributable to fracture management may be estimated in different ways. In some studies, all health care resources following the fracture occurrence were assumed to be due to the fracture; in other studies, the estimate was an incremental cost obtained by comparing the preceding year or to a control group.
To compare our results to previous studies, we adjusted the estimates to the 2002 values (3% per year) and converted them in Euros by using the 8/2004 exchange rates. The results are presented in Tables 8 and 9.
Despite the limitations cited above, our results on hip fractures were in the same order of magnitude than previous studies in the same countries. The study by Levy in France (1989) found higher estimates for hip fractures (15,907€ after adjustment). This difference may be due to the important number of days in rehabilitation centres found in Levy’s study (75–450) leading to a rehabilitation cost of 7,081€. This might be due to a more frequent management of hip fracture by orthopaedic treatment or immobilisation by cast or splint in the late eighties, compared to current practices.
In other European countries of similar economic level, most 2003 adjusted estimates were in the same order of magnitude as our results i.e. in a range between 8,799 and 16,200€. Three studies estimated costs up to 29,207€ (Sernbo), 23,539€ (Zethraus) and 17,564€ (Haentjens) because they considered all resources consumed in the full year following the fracture. The main items accounting for the increase of the total cost were nursing home stays and re-hospitalisations. Kanis estimated the cost of hip fracture leading to nursing home admission in UK at 44,422€ in first year, and at 30,965€ in the second year following the occurrence of fractures. Schürch in Switzerland estimated at 47,897€ the cost for acute care for hip fracture. This very high estimate was due to the high cost of inpatient care per day in this country. In Belgium the inpatient costs were estimated based on duration of hospitalization (in other countries, local costs per Disease Related Group were used). In the study of Reginster in this country, the mean duration of hospitalization was 26 days and this duration was 29 days in the study of Haentjens [34, 23]. These numbers are very closed to the one of our study (24 days).
For wrist fractures, our estimates were higher than in other published studies [40]. The main reason for this difference is due to a higher rate of hospitalisation (56.1%) than most other studies (0–40%). This highlights the fact that the hospitalisation rate is a key factor for estimating the cost of this type of fractures.
If one considers that the increasing incidence of fractures associated with osteoporosis is age-dependant and that osteoporosis is the major, if not the unique, factor inducing such an age-related change, then many other fractures must be considered as osteoporotic at least in Caucasian women [36, 41]. Consequently, the real costs of osteoporosis are probably underestimated in most studies.
References
Consensus development conference (1993) Diagnosis, prophylaxis and treatment of osteoporosis. Am J Med 94:646–650
Kanis JA, Melton LJ, Christiansen C, Johnston CC, Khaltaev N (1994) The diagnosis of osteoporosis. J Bone Miner Res 9:1137–1141
Johnell O, Kanis J (2005) Epidemiology of osteoporotic fractures. Osteoporos Int 16(Suppl 2):S3–S7
Kanis JA, Johnell O, Oden A, Sernbo I, Redlund-Johnell I, Dawson A, De Laet C, Jonsson B (2000) Long-term risk of osteoporotic fracture in Malmo. Osteoporos Int 11(8):669–674
Cooper C, Campion G, Melton LJ III (1992) Hip fractures of the elderly: a worldwide projection. Osteoporos Int Int 2:285–289
Gillet P, Reginster JY (1999) Increased number of hip fractures. Lancet 353:2160–2161
Melton LJ III (1999) Cost-effective treatment strategies for osteoporosis. Osteoporosis Int 9(Suppl 2):S111–S116
Holland E, Rogers L (1989) Osteoporosis: impact on the elderly, sociatal concerns, and the role of radiology. Curr Probl Diagn Radiol 18:46–61
Edy DM, Johnston CC Jr, Cummings SR (1998) Osteoporosis: review of the evidence for prevention, diagnosis, and treatment and cost-effectiveness analysis. Status report. Osteoporos Int 8(Suppl 4):1–88
US Congress Office of Technology Assessment (1994) Hip fracture outcomes in people age 50 and over: background paper. Washington DC/ US Goverment Printing office, July
Johnell O (1997) The socioeconomic burden of fractures: today and in the 21st century. Am J Med 103(2A):20S–25S
Gabriel SE, Tosteson AN, Leibson CL, Crowson CS, Pond GR, Hammond CS, Melton LJ 3rd (2002) Direct medical costs attributable to osteoporotic fractures. Osteoporos Int 13(4):323–330
Meunier PJ, Reginster JY (2003) Design and methodology of the phase 3 trials for the clinical development of strontium ranelate in the treatment of women with postmenopausal osteoporosis. Osteoporos Int 14(Suppl 3):S66–S76
Reginster JY, Lecart MP, Deroisy R, Lousberg C (2004) Strontium ranelate: a new paradigm in the treatment of osteoporosis. Expert Opin Investig Drugs 13(7):857–864
Meunier PJ, Roux C, Seeman E, Ortolani S, Badurski JE, Spector TD, Cannata J, Balogh A, Lemmel EM, Pors-Nielsen S, Rizzoli R, Genant HK, Reginster JY (2004) The effects of strontium ranelate on the risk of vertebral fracture in women with postmenopausal osteoporosis. N Engl J Med 350:459–468
Reginster JY, Seeman E, De Vernejoul MC, Adami S, Compston J, Phenekos C, Devogelaer JP, Curiel MD, Sawicki A, Goemaere S, Sorensen OH, Felsenberg D, Meunier PJ (2005) Strontium, ranelate reduces the risk of nonvertebral fractures in post-menopausal women with osteoporosis: treatment of peripheral osteoporosis (TROPOS) study. J Clinical Endocrinol Metab 90(5):2816–2822
Data available on the site: http://www.oecd.org/dataoecd/13/12/31963479.xls. Consulted on November 2nd 2005
Lindsay R (1995) The burden of osteoporosis: cost. Am J Med 98(2A):9S–11S
Levy E (1989) Cost analysis of osteoporosis related to untreated menopause. Clin Rheumatol 8(Suppl 2):76–82
Jönsson B, Christiansen C, Johnell O, Hedbrandt J (1995) Cost-effectiveness of fracture prevention in established osteoporosis. Osteoporos Int 5(2):136–142
Kakarlapudi TK, Santini A, Shahane SA, Douglas D (2000) The cost of treatment of distal radial fractures. Injury 31(4):229–232
French FH, Torgerson DJ, Porter RW (1995) Cost analysis of fracture of the neck of femur. Age Ageing 24(3):185–189
Reginster JY, Gillet P, Ben Sedrine W, Brands G, Ethgen O, De Froimont C, Gosset C (1999) Direct costs of hip fractures in patients over 60 years of age in Belgium. Pharmacoeconomics 15(5):507–514
Parker MJ, Myles JW, Pryor GA, Lodwick R (1991) Cost analysis of different aspects of treatment of patients following fracture of the proximal femur. J Bone Joint Surg Br 73B:70
Visentin P, Ciravegna R, Fabris F (1997) Estimating the cost per avoided hip fracture by osteoporosis treatment in Italy. Maturitas 26(3):185–192
Hollingworth W, Todd CJ, Parker MJ (1996) The cost of treating hip fractures in the twenty-first century: short report. Osteoporos Int 6(Suppl 2):13–15
Dolan P, Torgerson DJ (1998) The cost of treating osteoporotic fractures in the United Kingdom female population. Osteoporos Int 8(6):611–617
Schurch MA, Rizzoli R, Mermillod B, Vasey H, Michel JP, Bonjour JP (1996) A prospective study on socioeconomic aspects of fracture of the proximal femur. J Bone Miner Res 11(12):1935–1942
Koeck CM, Schwappach DL, Niemann FM, Strassmann TJ, Ebner H, Klaushofer K (2001) Incidence and costs of osteoporosis-associated hip fractures in Austria. Wien Klin Wochenschr 113(10):371–377
Ankjaer-Jensen A, Johnell O (1996) Prevention of osteoporosis: cost-effectiveness of different pharmaceutical treatments. Osteoporos Int 6:265–275
Borgquist L, Lindelöw G, Thorngren KG (1991) Costs of hip fracture. Rehabilitation of 180 patients in primary health care. Acta Orthop Scand 62:39–48
Koeck CM, Schwappach DL, Niemann FM, Strassmann TJ, Ebner H, Klaushofer K (2001) Incidence and costs of osteoporosis-associated hip fractures in Austria. Wien Klin Wochenschr 113(10):371–377
Brecht JG, Kruse HP, Felsenberg D, Mohrke W, Oestreich A, Huppertz E (2003) Pharmacoeconomic analysis of osteoporosis treatment with risedronate. Int J Clin Pharmacol Res 23(4):93–105
Haentjens P, Autier P, Barette M, Boonen S; Belgian Hip Fracture Study Group (2001) The economic cost of hip fractures among elderly women. A one-year, prospective, observational cohort study with matched-pair analysis. Belgian Hip Fracture Study Group. J Bone Joint Surg Am 83-A(4):493–500
Nurmi I, Narinen A, Luthje P, Tanninen S (2003) Cost analysis of hip fracture treatment among the elderly for the public health services: a 1-year prospective study in 106 consecutive patients. Arch Orthop Trauma Surg 123(10):551–554
De Laet CE, van Hout BA, Burger H, Weel AE, Hofman A, Pols HA (1999) Incremental cost of medical care after hip fracture and first vertebral fracture: the Rotterdam study. Osteoporos Int 10(1):66–72
Sernbo I, Johnell O (1993) Consequences of hip fracture: a prospective study over 1 year. Osteoporosis Int 3:148–153
Zethraeus N, Gerdtham UG (1998) Estimating the costs of hip fracture and potential savings. Int J Technol Assess Health Care 14(2):255–267
Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M (2002) Treatment of established osteoporosis: a systematic review and cost-utility analysis. Health Technol Assess 6(29):1–146
Chamberlin B, Benazet JP, Humbert B, Saillant G (1999) Direct cost assessment of wrist fractures. Rev Chir Orthop Reparatrice Appar Mot 85(8):828–833
Seeley DG, Browner WS, Nevitt MC, Genant HK, Scott JC, Cummings SR (1991) Which fractures are associated with low appendicular bone mass in the elderly women? The Study of Osteoporotic Fractures Research Group. Ann Intern Med 115:837–842
Acknowledgments
This study has been granted by the Servier Laboratories.
Author information
Authors and Affiliations
Corresponding author
Additional information
Conflict of Interest: Professors Meunier and Reginster have received fees from Servier for their support as consultant for the research conducted by Servier.
This is the first published study estimating the cost of osteoporotic fractures other than vertebral, hip and wrist. The estimates are based on data collected in two clinical trials and might concern a selected subgroup of women meeting the inclusion criteria.
Rights and permissions
About this article
Cite this article
Bouee, S., Lafuma, A., Fagnani, F. et al. Estimation of direct unit costs associated with non-vertebral osteoporotic fractures in five European countries. Rheumatol Int 26, 1063–1072 (2006). https://doi.org/10.1007/s00296-006-0180-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-006-0180-x