
Abstract
The aim of the study was to compare the effects of once-weekly alendronate sodium and daily risedronate sodium treatment on bone mineral density (BMD) and bone turnover markers in postmenopausal osteoporotic subjects. For this purpose, 50 patients were included in this study and randomly classified into two groups. Group I (n=25) received risedronate (5 mg/day) and group II (n=25) received alendronate Na (70 mg/week). The study duration was limited to 12 months. The efficacy of the treatment was evaluated by BMD measurements at spine and hip at 6th and 12th months of the treatment, as well as by the measurement of bone turnover markers such as serum osteocalcin (OC), bone-specific alkaline phosphatase (BASP), urine deoxypyridinoline (DPD) and calcium/creatine ratio in 24-h urine at 1st, 3rd, 6th and 12th months. The evaluation of the changes in BMD in all regions revealed a significant increase in BMD in both groups compared to baseline values except for spine (L2–L4) in alendronate group at 6th and 12th month and femoral neck in risedronate group at 6th month. However, the difference in percentage increase in BMD measurements was not statistically significant between the two groups at 6th and 12th months. In both groups, serum OC, BSAP and urine DPD were found to be significantly attenuated at 1st month of the treatment period, and continued to be lowered throughout the 3rd, 6th and 12th months (P<0.05). However, there was no statistically-significant difference between both groups of patients (P>0.05). In conclusion, our results suggest that both treatment protocols provide treatment options of similar efficiencyfor postmenopausal osteoporosis, and have almost-similar effects in enhancing the BMD and in slowing the bone turnover. Risedronate seems to havea more potent effect in the spinal region than that of alendronate, although this potency was not statistically significant.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is defined as a skeletal condition characterized by reduced bone mass, micro-architectural deterioration of bone tissue leading to increased bone fragility, and a consequent increase in fracture risk [1]. Osteoporotic fractures are widely recognized as common and important causes of morbidity and mortality among postmenopausal women [2]. Osteoporosis, which is a very frequent disease affecting a large proportion of the population, is considered to be a worldwide major health problem [3].
Current treatment alternatives for osteoporosis include bisphosphonates, calcitonin, and selective estrogen receptor modulators, but sufficient calcium and vitamin D are prerequisites [4]. Over the past 15 years, bisphosphonates have been demonstrated as effective therapy for the treatment of osteoporosis based on their ability to suppress bone turnover, resulting in increased bone mineral content and increased bone strength [5]. They are listed as a first-line therapeutic option for the management of postmenopausal osteoporosis [6]. These drugs strongly suppress osteoclastic bone resorption both in vitro and in vivo. The potency of these compounds in inhibiting osteoclastic activity differs by as much as 10,000-fold and is clearly influenced by their structures [7].
Risedronate and alendronate have consistently demonstrated to reduce the biochemical markers of bone turnover and to increase bone mineral density (BMD). Risedronate, a third-generation pyridinylbisphosphonate, is shown to inhibit bone resorption at doses which neither impair bone mineralization nor cause osteomalasia [8]. It has also been shown to reduce the incidence of vertebral fractures and a composite endpoint of osteoporosis-related fractures [9–11]. As with risedronate, alendronate has also been reported to reduce the incidence of osteoporotic fractures including spine, hip and the wrist in postmenopausal women with osteoporosis [12–15]. To facilitate its usage and to improve convenience and tolerability, a 70-mg once-weekly form has been developed. The effects of this newly-developed form of alendronate have been compared with the daily form in some recent studies, and it has been suggested that both have similar effects on BMD and bone turnover parameters over 24 months of treatment [16, 17].
Although there are many studies comparing the effects of alendronate and risedronate with ethidronate [18–20] there are limited data comparing the effects of weekly alendronate and daily risedronate treatments [21]. In the present study, the effects of alendronate Na (70 mg/week) and risedronate Na (5 mg/day) on BMD and bone turnover markers were compared.
Participants and methods
Participants
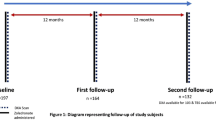
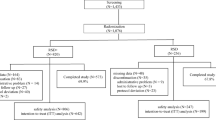
In this prospective, single-blind randomized study, 50 postmenopausal women with osteoporosis were included and randomized into two groups. Group I (n=25) were given 5 mg of risedronate daily, and Group II (n=25) were given weekly 70 mg alendronate Na. Both groups also received 1000 mg/day calcium and 400 IU/day D vitamins as supplemental therapy throughout the study. All patients were evaluated in detail for osteoporotic risk factors such as smoking, alcohol and coffee consumption, calcium intake, number of parity and lactation period. Patients over 75 years and taking treatment for osteoporosis (i.e. estrogens, calcitonin, and anabolic steroids) were not included in the study. The presence of any disease which interferes with bone metabolism (i.e. metabolic, inflammatory, hepatic, renal, malignant or immune disorders), recent use of drugs known to affect bone metabolism and history of esophagitis and peptic ulcer were also accepted as exclusion criteria. Lateral and anteroposterior (AP) thoracic and lumbar spine radiographs were obtained at baseline and at 12th month, and were evaluated for vertebral fracture. All subjects were asked to give written informed consent for participation in the study, which was approved by the Ethical Review Committee of Celal Bayar University, Faculty of Medicine.
Methods
Bone mineral density was measured by DXA using a Lunar DPX (IQ, MD, USA) device in the pretreatment period and at 6th and 12th months at the following sites: lumbar spine (L2–L4) in AP projection, and left hip including femoral neck, trochanter, Ward’s triangle and total hip. A diagnostic criterion for osteoporosis was proposed according to the WHO criteria and was defined as T-score of less than −2.5 SD [22]. Bone turnover markers including bone formation markers of serum osteocalcin (OC) and bone specific alkaline phosphatase (BSAP) levels were assessed, in addition to bone resorption markers of urine deoxypyridinoline (DPD) levels and urine calcium and creatine ratio (Ca/Cr) in 24-h urine samples in the pretreatment period and at 1st, 3rd, 6th and 12th months. Serum OC and urinary DPD levels were measured by means of an enzyme-amplified chemiluminescence assay (IMMULITE, Diagnostic Products Corporation, Los Angeles, CA, USA). Osteocalcin test method sensitivity was 0.1 ng/ml; intra- and inter-assay CV% was 2.8 and 3.9 respectively at 6.92 ng/ml. Reference ranges for osteocalcin levels were 0.4–8.2 ng/ml in the premenopausal period and 1.5–11 ng/ml in the postmenopausal period). DPD test method sensitivity was 4.4 nM; intra- and inter-assay CV% were 8.9 and 9.7 respectively at 100 nM. Reference ranges for DPD levels were 3.0–7.4 nM DPD/mg creatine. Serum BSAP levels was assessed by heat inactivation method. Serum total alkaline phosphatase, urine calcium and urine creatine levels were assessed by enzymatic methods on auto analyzer by commercial reagents (Integra 800, Roche Diagnostics Corporation, Indianapolis, USA).
Statistical analysis
SPSS version 11.0 was used for statistical analysis. Data are expressed as mean ± standard deviation (SD). Differences between the pre- and post-treatment values in the same group were analyzed by Friedman test and their post-hoc analyses were performed using the Wilcoxon signed rank test. Differences between the two groups at baseline and at 1st, 3rd, 6th and 12th months were analyzed using the Mann–Whitney U-test. P-values<0.05 were considered to be significant.
Results
Characteristics of the patients included in the study are summarized in Table 1. Age, menopause age, body mass index and daily calcium intake were similar in both groups. BMD values during the pretreatment period for the region of spine (L2–L4), femoral neck, trochanter and Ward’s triangle were also similar. Two patients in the risedronate group and three patients in the alendronate group had previous compression fractures in lumbar vertebrae. No other fracture was detected throughout the study period.
The changes in BMD values and the percentage increase in BMD levels at the 6th and the 12th months of treatment are summarized in Table 2 and in Fig. 1. The evaluation of the changes in BMD in all regions revealed a significant increase in BMD in both groups compared to the baseline values, except for the spine (L2–L4) in the alendronate group at the 6th and 12th months and the femoral neck in the risedronate group at 6th month. However, the difference in percentage increase in BMD measurements was not statistically significant between the two groups at the 6th and 12th months.

Percentage increase in BMD with standard deviation in the two groups of patients at 6th and 12th months of treatment in the two groups of patients. No significant difference was found between the two groups in all measurements.
Values and percentage changes in serum OC, BSAP, urine DPD and 24-h urine calcium/creatine (Ca/Cr) ratio at baseline, 1st, 3rd, 6th and 12th months of the treatment in the two groups of patients are given in Table 3. In both groups, serum OC, BSAP and urine DPD values were found to be significantly attenuated at 1st month of the treatment period and persisted at 3rd, 6th and 12th months (p<0.05). However, there was no statistically-significant difference between the two groups of patients. 24-h urine Ca/Cr ratio was found decreased at 1st month of the study period in the risedronate group, and observed to increase after 3rd month. In the alendronate group, the Ca/Cr ratio in 24-h urine was found to be decreased after 1st month of treatment period. However the change in the Ca/Cr ratio in 24-h urine was not statistically significant between the two groups of patients.
Discussion
In the present study, the effects of two therapy protocols were observed to be similar both on BMD and bone turnover. Although risedronate gave a noteworthy increase in BMD at 6th and 12th months at the spine region compared to alendronate, the differences were not statistically significant. We used a daily dose of 5 mg risedronate in the present study, because a once-weekly dose of 35 mg risedronate was not commercially available at the time we started the study. Nevertheless, a recent study comparing the effects of 5 mg/day and 35 mg/week doses of risedronate therapy revealed similar results on BMD [23]. Thus we believe that the differences between the doses and intervals would not be the source of much variation.
Bisphosphonates are commonly used in postmenopausal osteoporosis, and their efficacy is proved by numerous studies [17, 24–26]. However, there are limited data concerning their comparative efficacy in postmenopausal osteoporosis. In one of these comparative studies concerning the therapeutic efficacy of 10 mg/day alendronate and 400 mg/day cyclic ethidronate, the increase in the BMD of lumbar vertebrae was not found to be significant at 12th month, similar to our results in the alendronate-treated group; however, statistically-significant increases were detected in BMD of the lumbar vertebrae in the ethidronate-treated group [19]. In addition, significant enhancement was reported in the entire femur region at 12th month with ethidronate therapy, whilst the only increase in BMD was found in trochanter and Ward’s triangle regions at 12th month with alendronate therapy.
In patients with involutional osteoporosis, 2.5 mg/day risedronate and 200 mg/day cyclic ethidronate treatments were compared, and the enhancements in BMD at L2–L4 were found to be higher in risedronate treatment compared to that of intermittent cyclic ethidronate treatment at the end of a 48-week therapy [18]. In the present study, the medications and the doses administered in the treatment protocol were different, and comparisons with these studies were not possible. Recently, once-weekly alendronate treatment has been considered as an advance in osteoporosis treatment for its administrational convenience. Rizzoli et al. [17] compared treatments of various doses of alendronate in postmenopausal osteoporosis, and reported that once-weekly 70 mg alendronate treatment has the same efficacy as daily doses. Sahota et al. [20], in their comparative study of continuous alendronate, cyclic alendronate and cyclic ethidronate treatments,reported that both types of treatment protocols have similar beneficial effects in terms of the gain in BMD at the spine and total hip.
In the extensive Medline search, only one study comparing once-weekly alendronate and daily risedronate therapy was detected [21]. In this multicenter study, the effects of alendronate (70 mg/week) and risedronate (5 mg/day) were compared. The authors state a higher enhancement in BMD values at the lumbar region in the alendronate group at 6th and 12th months, compared to the risedronate group. However, in our study, a statistically-significant enhancement was found in the risedronate group both at the lumbar and hip regions at the end of 1 year, while in the alendronate group significant BMD increase was observed only in the hip region, and no significant increase was detected at the lumbar region. Nevertheless, statistical evaluations showed that no significant increases in BMD were found between the groups when all the regions were compared.
In addition, Hosking et al. [21] stated that there are higher enhancements in BMD in the trochanter and total hip BMD measurement at 6th and 12th months in the alendronate group compared to risedronate group; however, in our study no significant differences were found between the alendronate and risedronate groups in BMD at the femoral neck, trochanter and Ward’s triangle of the hip region. This discrepancy between our results and Hosking et al. [21] could be related to the limited number of patients in our study groups.
Although more patients were included at the commencement of the present study, some patients did not complete the 12-month treatment period for private reasons and thus were excluded from the study. In addition, the mean age of our study groups were lower than for Hosking et al. [21]. The mean age of the patients in the study by Hosking et al. [21] is 68.9±5.9 years in the risedronate group and 69.2±6.6 years in the alendronate group. In the present study the mean age ± SD of the patients in the risedronate group is 60.3±7.1 years and that for the alendronate group is 57.3±6.6 years. The mean duration of the menopause period is 20.3±8.0 years in the risedronate group and 20.8±8.3 years in the alendronate group in the study by Hosking et al. [21]. However, in the present study menopause-period durations are shorter. Thus, the mean age and the durations of the menopause period of our study groups were lower than those of Hosking et al. [21], which may further explain the discrepancies between the two studies.
In the present study, bone-turnover markers were observed to be similarly decreased in both therapy alternatives. In both groups, serum OC, BSAP and urine DPD levels were found to be significantly decreased at 1st month of treatment period and maintained throughout the 3rd, 6th and 12th months (P<0.05). Our results seem to be in contradiction with those of Hosking et al. [21], who reported that once-weekly alendronate produces a significantly-greater reduction in urine NTx and BSAP levels than risedronate does (52% vs 32%, P<0.001 and 40% vs 24%, P<0.001). However, in our study reductions in the urine DPD and BSAP levels was quite similar in once-weekly alendronate and risedronate groups (58% and 57.8%, P>0.05, 31.6% and 25%, P>0.05 respectively). Moreover, OC levels were found to be decreased at 1st month and maintained throughout 3rd, 6th and 12th months. No difference was observed in reduction of OC values between both groups (Table 3).
There are many suggestions for the therapeutic efficacy of antiresorptive agents and for their therapeutic durations. There are reports stating that most rapid achievements in BMD are at 6th month, and the efficacy continues in the second and third years; nevertheless, some researchers also state that due to long remodeling cycles it may not be possible to observe the real effect of the antiresorptive agents on BMD in the first year, but that efficacy may be prominent in the second and third years of treatment [19]. In our study, the therapy period was limited to 12 months; however, the enhancements in BMD achieved in both alendronate and risedronate therapies within a period of 6 months support the former theory.
If summarized, the achievements attained by both therapy protocols on treatment of postmenopausal osteoporosis were found to be similar. Between administrations of 70 mg of once-weekly alendronate and of 5 mg/day risedronate, the bone-formation and resorption markers of urine DPD and serum OC levels showed no significant differences at 3rd, 6th and 12th months compared to the pretreatment levels. In both therapy protocols, no significant differences were found between the groups at 6th and 12th months in the BMD measurements of lumbar vertebrae (L2-L4), left hip Ward’s triangle, trochanter and femoral neck. In both treatment protocols, BMD was found to be increased in all regions at 6th and 12th months compared to those of the pretreatment levels. In the alendronate group, the enhancements in BMD at the lumbar region at 6th and 12th months and in the risedronate group enhancement in BMD at the femoral neck at 6th month were not found to be statistically significant.
In conclusion; our results suggest that both treatment protocols provide treatment options of similar efficiency for postmenopausal osteoporosis and have almost-similar effects in enhancing the BMD and in slowing bone turnover. Daily risedronate treatment seems to have a more potent effect in the lumbar region compared to alendronate, although this potency was not statistically significant.
References
Consensus development conference: prophylaxis and treatment of osteoporosis (1991) Osteoporos Int 1:114–117
Garrett-Connor E (1995) The economic and human costs of osteoporotic fracture. Am J Med 98:3–8
Ammann P, Rizzoli R (2003) Bone strength and its determinants. Osteoporos Int 14(suppl 3):13–18
Akesson K (2003) New approaches to pharmacological treatment of osteoporosis. Bull World Health Organ 81:657–664
Cohen SB (2004) An update on bisphosphonates. Curr Rheumatol Rep 6:59–65
Cummings SR, Karpf DB, Harris F, Genant HK, Ensrud K, LaCroix AZ, Black DM (2002) Improvement in spine bone density and reduction in risk of vertebral fractures during treatment with antiresorptive drugs. Am J Med 112:281–289
Yates J, Rodan GA (1998) Alendronate and osteoporosis. Drug Dis Today 3:69–78
McClung M, Bensen W, Bologne M (1996) Risedronate treatment of postmenopausal women with low bone mass: preliminary data. Osteoporos Int 6(suppl I):256
Clemmesen B, Ravn P, Zegels B,Taquet AN, Christiansen C, Reginster JY (1997) A 2-year phase II study with 1-year of follow-up of risedronate (NE-58095) in postmenopausal osteoporosis. Osteoporos Int 7:488–495
Reginster J, Minne HW, Sorensen OH, Hooper M, Roux C, Brandi ML, Lund B, Ethgen D, Pack S, Roumagnac I, Eastell R (2000) Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral efficacy with risedronate therapy (VERT) study group. Osteoporos Int 11:83–89
Harris ST, Watts NB, Genant HK, McKeever CD, Hangartner T, Keller M, Chesnut CH, Brown J, Eriksen EF, Hoseyni MS, Axelrod DW, Miller PD (1999) Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis.: a randomized control trial. Vertebral efficacy with Risedronate therapy (VERT) study group. JAMA 282:1344–1352
Liberman UA, Weiss SR, Broll J, Minne HW, Quan H, Bell NH, Rodriguez-Portales J, Downs RW, Dequeker J, Favus M (1995) Effect of alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. N Engl J Med 333:1437–1443
Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC, Bauer DC, Genant HK, Haskell WL, Marcus R, Ott SM, Torner JC, Quandt SA, Reiss TF, Ensrud KE (1996) Randomized trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Lancet 348:1535–1341
Black DM, Thompson DE, Bauer DC, Ensrud K, Musliner T, Hochberg MC, Nevitt MC, Suryawanshi S, Cummings SR (2000) Fracture risk reduction with alendronate in women osteoporosis: the Fracture Intervention Trial : FIT Research Group. J Clin Endocrinol Metab 85:4118–4124
Levis S, Quandt SA, Thompson D, Scott J, Schneider DL, Ross PD, Black D, Suryawanshi S, Hochberg M, Yates J (2002) Alendronate reduces the risk of multiple symptomatic fractures: results from the fracture intervention trial. J Am Geratr Soc 50:409–415
Schnitzer T, Bone HG, Crepaldi G, Adami S, McClung M, Kiel D, Felsenberg D, Recker RR, Tonino RP, Roux C, Pinchera A, Foldes AJ, Greenspan SL, Levine MA, Emkey R, Santora AC, Kaur A, Thompson DE, Yates J, Orloff JJ (2000) Therapeutic equivalence of alendronate 70 mg once-weekly and alendronate 10 mg daily in the treatment of osteoporosis. Alendronate Once-Weekly Study Group. Aging (Milano)12:1–12
Rizzoli R, Greenspan SL, Bone G, Schnitzer TJ, Watts NB, Adami S, Foldes AJ, Roux C, Levine MA, Uebelhart B, Santora AC 2nd, Kaur A, Peverly CA, Orloff JJ (2002) Alendronate Once-Weekly Study Group: Two-year results of once-weekly administration of alendronate 70 mg for the treatment of postmenopausal osteoporosis. J Bone Miner Res 17:1988–1996
Fukunaga M, Kushida K, Kishimoto H, Shiraki M, Taketani Y, Minaguchi H, Inoue T, Morita R, Morii H, Yamamoto K, Ohashi Y, Orimo H (2002) A comparison of the effect of risedronate and ethidronate on lumbar bone mineral density in Japanese patients with osteoporosis: a randomized controlled trial. Osteoporos Int 13:971–979
Ertekin H, Onbasi K, Yaradanakul S (1999) Postmenopozal osteoporozda ethidronat ve alendronat tedavilerinin karsilastirilmasi. Cukurova Universitesi Tip Fakultesi Dergisi 24:125–137
Sahota O, Fowler I, Blackwell PJ, Lawson N, Cawte SA, San P, Masud T, Hosking DJ (2000) A comparison of continuous alendronate, cyclical alaendronate and cyclical ethidronate with calcitriol in the treatment of postmenopausal vertebral osteoporosis: a randomized controlled trial. Osteoporos Int 11:956–966
Hosking D, Adami S, Felsenberg D Andia JC, Valimaki M, Benhamou L, Reginster JY, Yacik C, Rybak-Feglin A, Petruschke RA, Zaru L, Santora AC (2003) Comparison of change in bone resorption and bone mineral density with once-weekly alendronate and daily risedronate: a randomized, placebo-controlled study. Curr Med Res Opin 19(5):1–12
World Health Organization (1994) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. WHO Technical Report Series 843, Geneva
Brown JP, Kendler DL, McClung MR Emkey RD, Adachi JD, Bolognese MA, Li Z, Balske A, Lindsay R. (2002) The efficacy and tolerability of risedronate once a week for a treatment of post-menopausal osteoporosis. Calcif Tissue Int 71:103–111
Seeman E (1999) The antifracture efficacy of alendronate. Int J Clin Pract Suppl 101:40–45
Fogelman I, Ribot C, Smith R, Ethgen D, Sod E, Reginster JY (2000) Risedronate reverses bone loss in postmenopausal women with low bone mass: results from a multinational, double-blind, placebo-controlled trial. BMD-MN study group. J Clin Endocrinol Metab 85:1895–1900
Watts NB, Josse RG, Hamdy RC, Hughes RA, Manhart MD, Barton I, Calligeros D, Felsenberg D (2003) Risedronate prevents new vertebral fractures in postmenopausal women at risk. J Clin Endocrinol Metab 88:542–549
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sarioglu, M., Tuzun, C., Unlu, Z. et al. Comparison of the effects of alendronate and risedronate on bone mineral density and bone turnover markers in postmenopausal osteoporosis. Rheumatol Int 26, 195–200 (2006). https://doi.org/10.1007/s00296-004-0544-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-004-0544-z