
Abstract
Purpose
ATI-1123 is a liposomal formulation of docetaxel and may be administered without the premedications and hypersensitivity reactions. This Phase I study examines the safety, tolerability, pharmacokinetics (PKs), and antitumor activity of ATI-1123.
Methods
Patients with advanced solid malignancies received escalating doses of ATI-1123 intravenously over 1-h every 3 weeks. The dosing commenced using an accelerated titration design and was followed by a modified 3 + 3 Fibonacci schema to determine maximally tolerated dose (MTD). Plasma was analyzed for encapsulated/non-encapsulated docetaxel; PK analyses were performed using model independent method. Response was assessed using RECIST criteria.
Results
In total, 29 patients received doses ranging from 15 to 110 mg/m2. At 110 mg/m2, two of six patients experienced dose-limiting toxicities including grade 3 stomatitis and febrile neutropenia. The 90 mg/m2 cohort was expanded to ten patients and identified as the MTD. The most common adverse events were fatigue, nausea, neutropenia, anemia, anorexia, and diarrhea. ATI-1123 exhibited linear and dose proportional PKs. One patient with lung cancer had confirmed partial response, and stable disease was observed in 75 % patients.
Conclusions
ATI-1123 demonstrated an acceptable tolerability and favorable PK profile in patients with solid tumors. Our results provide support for Phase II trials to determine the antitumor activity of this drug.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Docetaxel is an antimitotic agent which binds to the beta subunit of tubulin and causes stabilization of tubulin polymerization. This stabilization results in cell cycle arrest at the G2/M phase, thus inhibiting mitosis [1]. It is a poorly water soluble semisynthetic taxane analogue, commonly used in the treatment of a variety of solid tumors including head and neck, non-small cell lung, prostate, breast, and gastric cancer [2–4]. The current recommended regimen for docetaxel is 60–100 mg/m2 administered over 1-h every 3 weeks, depending upon the indication [5].
Taxotere® is the standard formulation of docetaxel with well-established safety and efficacy when administered in 3-week cycles [6]. Because of its poor water solubility, it is formulated with solvents that can potentially contribute to treatment-related adverse events such as hypersensitivity reaction. Current docetaxel and other taxane formulations often complicate drug delivery and can alter both the PK and toxicity profiles. These problematic issues have spurred interest in the development of liposomal taxanes including ATI-1123.
Liposomes are drug carriers that serve as sustained release systems, while providing protection from drug degradation. Liposomes may also help in overcoming multidrug resistance mediated by transporter-mediated resistance efflux mechanisms [7, 8]. Currently, there are several liposome-based drugs approved for clinical use including amphotericin B (Ambisome®), liposomal doxorubicin (Doxil®), and liposomal daunorubicin (DaunoXome®). ATI-1123 is a liposomal formulation of docetaxel using protein-stabilized nanoparticles (PSN) encapsulating docetaxel in the lipid bilayer of liposome. The ATI-1123 liposome is constructed of phospholipids, cholesterol, human serum albumin, and sucrose. This results in a potentially safer formulation of docetaxel for the treatment of a variety of malignancies. Preclinical experience with ATI-1123 did not suggest a negative effect of liposomal encapsulation on the drug activity (unpublished preclinical data). The rationale behind the development of ATI-1123 is to remove the need for unwanted solvents such as Tween 80, reduce hypersensitivity reactions, eliminate the requirement for premedications, and enhance systemic docetaxel exposure.
Significant antitumor activity was reported in several human tumor xenograft models, including prostate, pancreatic, and docetaxel-resistant mesothelioma (unpublished preclinical data). Overall, the systemic exposure and peak plasma concentration (C max) were significantly higher for ATI-1123 in comparison with the Taxotere®. The distribution of ATI-1123 was higher in liver and lung tissues as compared to Taxotere®. The toxicities observed with ATI-1123 in animal models included lethargy, emesis, diarrhea, and mucosal necrosis at high doses. Reversible suppression of bone marrow function was observed at higher doses with adequate recovery by Day 21.
To explore the potential clinical utility of ATI-1123, we have conducted a Phase I study of this drug for patients with advanced solid tumors. The objectives of this trial were to determine the MTD, toxic effects, and PK profile of this formulation. Because of the liposomal encapsulation, we anticipated that hypersensitivity reactions would be diminished or absent.
Materials and methods
Study design
This first-in-human Phase I, bicenter study was approved by the relevant Institutional Review Boards; all participating patients signed an informed consent document in accordance with the Declaration of Helsinki (trial was registered on clinicaltrials.gov as NCT01041235).
ATI-1123 was administered as a 1-h intravenous infusion every 21 days in adult patients with solid tumors. Standard pretreatment medications for docetaxel (corticosteroids, HI and H2 antagonists, antiemetics) were not administered before the initial dose of ATI-1123. If a patient experienced clinically significant hypersensitivity reaction after the initial dose, pretreatment medication was allowed as medically indicated before subsequent doses. The up-front prophylactic use of granulocyte-colony stimulating factor (G-CSF) during first cycle was not permitted. However, after the first treatment cycle, patients who had experienced grade 4 neutropenia or grade 3 febrile neutropenia could receive prophylactic G-CSF with subsequent treatment cycles. If treatment was well tolerated, patients were allowed to receive repeated 21-day treatment cycles until the occurrence of progressive disease or unacceptable toxicity.
Based on preclinical experience, the ATI-1123 starting dose for the first cohort was 15 mg/m2. The MTD in a single-dose good laboratory practice (GLP) toxicology study in the rat was 213.4 mg/m2. Based on approximately one-tenth of the MTD dose in rat, the starting dose in humans estimated to be 21.3 mg/m2. However, a lower starting dose of 15 mg/m2 was used to account for significantly higher drug exposure of ATI-1123 as compared to Taxotere®. The study initially followed an accelerated titration design to minimize the number of patients treated with potentially sub-therapeutic doses. At each dose level during this phase, single-patient cohorts were treated, with 100 % dose escalation. The accelerated titration phase reverted to traditional 3 + 3 design, when a patient experienced a ≥grade 2 drug-related or dose-limiting toxicity. During this phase, at least three patients were treated at each dose level, and dose escalations proceeded in accordance with a modified Fibonacci schema. If one patient experienced a DLT, up to three additional patients were treated at that dose level. The MTD was the highest dose at which no more than one of six patients experienced a DLT. If two or more patients experienced a DLT, a total of six patients were treated at the previous dose level. Once the MTD was determined, additional patients were treated at that dose to further confirm the safety profile of ATI-1123. Patients who experienced a DLT stopped study medication, but could restart at a lower dose level if they recovered to grade ≤2 adverse event (AE) with in 1 week (up to one dose reduction allowed). Dose reduction was also made for patients who had a delay in treatment greater than 1 week due to a lack of recovery of any toxicity. Subsequent retreatment of such patients after recovery was up to the medical monitor, taking into account the potential benefit and risk. No intrapatient dose escalation was allowed.
The following drug-related AEs (National Cancer Institute Common Terminology Criteria for Adverse Events; NCI CTCAE version 3.0) were protocol defined as DLTs: grade 4 neutropenia for more than 7 days, grade 3 or greater febrile neutropenia, grade 4 thrombocytopenia or grade 3 thrombocytopenia with clinically significant bleeding, grade 3 or 4 non-hematological toxicity (except for inadequately managed nausea, vomiting, or diarrhea). Any drug-related toxicity resulting in a dose interruption in cycle 1 of more than 2 weeks was also considered as dose limiting.
Patient eligibility
Male or female patients with a histologically confirmed metastatic solid tumor for whom no standard curative/palliative treatment existed or was no longer effective were eligible. Other eligibility criteria included: signed informed consent; age ≥18 years; Eastern Cooperative Oncology Group (EGOG) performance status of <2; life expectancy of at least 3 months; recovery from any prior surgery and any AEs related to previous therapy, previous radiotherapy or chemotherapy >4 weeks before the first dose (>6 weeks for mitomycin C or nitrosoureas); adequate bone marrow function (absolute neutrophil count >1,500/mm3, platelet count >100,000/mm3); adequate hepatic function (normal bilirubin, AST and ALT <2.5 times upper limit of normal); and adequate renal function (serum creatinine <1.5× upper limit of normal). Patients were permitted to have had prior chemotherapy, radiation therapy, or biological therapy. Patients with progressive brain metastases, seizure disorder, unstable angina or cardiac arrhythmia, severe chronic obstructive pulmonary disease, any active infection, and previous history of hepatitis B, C or human immunodeficiency virus were excluded. Patients with past history of allergic reactions to docetaxel and pregnant women were also excluded.
Pharmacokinetic sampling
PK blood sampling for ATI-1123 was performed during the first cycle prior to the initiation of infusion, at completion of infusion (time 0), and at 15 min, 30 min, 1 h, 2 h, 4 h, between 8–10 h, 24 h, and 48 h after the completion of infusion. A single PK sample was also collected on day eight. Patients who received a second cycle of treatment and were enrolled in the MTD cohort had blood samples collected prior to the initiation and end of ATI-1123 infusion to determine the effects of repeat dosing on pharmacokinetics. The pharmacokinetic parameters included C max, area under the plasma concentration–time curve (AUC), half-life (t1/2), clearance (CL), and volume of distribution (Vd). These PK parameters were determined in each subject by standard model independent method (WinNonlin). Dose proportionality of the three analytes of docetaxel was examined using a simple linear regression model and a power-law model using GraphPad Prism v 5.01 (GraphPad Inc., CA). The equation for linear regression is C max or AUC(0–inf) = μ + β × dose, where μ represents the intercept and β is the slope of the regression model. If the slope was significantly greater than zero and the intercept was not significantly greater than zero, then evidence of dose linearity was assumed (P value set at P ≥ 0.05). In the power model, log C max and log AUC(0–inf) were modeled as a function of subject, and log dose, with subject being considered as a random factor [9, 10]. The equation for power model is log C max or log AUC(0–inf) = log (μ) + β × log dose + ε, where log(μ) and β are the intercept and slope, respectively. On the back-transformed scale, this model is EAUC(0–inf) or C max = α × doseβ. The slopes of log PK parameters versus log dose and its 90 % confidence intervals (CIs) are used to conclude dose proportionality (the 90 % CI for the slope should include 1.00). A slope of 1.00 indicates perfect dose proportionality, and a slope of <1.00 or >1.00 indicates a less or greater than dose proportional, respectively. All plasma samples were assayed for encapsulated, non-encapsulated, and total docetaxel. Quantification of docetaxel concentrations was performed using a validated LC–MS/MS method developed by MicroConstants (San Diego, CA). Dose proportionality for the three analytes was assessed using a power-law model, linear regression model, and analysis of variance (ANOVA) model.
Response evaluation
Patients underwent response assessment as defined in the RECIST version 1.1 following completion of two 21-day cycles of therapy. Confirmatory scans were obtained no more than 4 weeks following the initial documentation of an objective response. Patients with stable disease or objective response who were tolerating study drugs were eligible for continued therapy with repeat response assessments performed after every other cycle.
Results
Patient demographics
A total of 29 patients received at least one dose of ATI-1123 and were included in the safety analysis. This included ten patients treated at MTD. The dose levels and the number of patients treated are listed in Table 1. The most common cancer types were lung, pancreas, and ovarian. The study population was heavily pretreated (median number of prior anticancer therapies was three). About one-third of study patients had prior exposure to Taxotere®. The baseline demographic characteristics of these patients are provided in Table 2.
Safety, maximally tolerate dose (MTD), and dose-limiting toxicities (DLT)
The MTD cohort had a total of ten evaluable patients. The maximally tolerated dose of this regimen is 90 mg/m2 as a 1-h intravenous infusion repeated every 3 weeks. In general, the ATI-1123 was tolerated well and had an acceptable toxicity profile. DLTs were observed in two out of six patients treated at 110 mg/m2. The ATI-1123 dose was reduced to 90 mg/m2, and the dosing cohort was expanded to include a total of ten subjects. Although three patients developed grade 4 neutropenia, all patients recovered quickly without any clinically significant infectious complications. Secondary prophylaxis with G-CSF was given only to those patients who experienced a neutropenic complication from a prior cycle of chemotherapy in line with American Society of Clinical Oncology guidelines [11]. At an intermediate dose level of 75 mg/m2, no DLTs were observed during the first cycle. With the two DLTs observed at 110 mg/m2 and no DLT in the intermediate cohort of eight patients, the MTD for ATI-1123 was defined at 90 mg/m2.
Of the two DLTs that occurred at 110 mg/m2 dose level, the first patient was a 62-year-old male with metastatic gastroesophageal carcinoma, who developed grade 3 stomatitis/mucositis during the first cycle. The second patient was a 46-year-old male with pancreatic cancer, who developed grade 3 febrile neutropenia 1-week post-initial treatment and needed hospitalization. Both of these patients continued on treatment after dose reduction.
Across all dose cohorts and treatment courses, fatigue (reversible) was the most commonly reported treatment-related AE (79 %), followed by nausea and neutropenia (both 65 %), anemia (62 %), anorexia, and diarrhea (both 48 %). These AEs were typically mild to moderate, not clinically significant and are listed in Table 3. In total, ten patients experienced a grade 2 or less hypersensitivity reaction during first cycle. Prior to subsequent cycles, these patients received premedication with a combination of oral corticosteroids, histamine-1 and 2 antagonists about 12 h as well as 30 min before a test dose (1 mg ATI-1123 over 3–5 min). This test dose was followed by administration of remainder of the protocol specified dose of ATI-1123 over 90 min. Only one patient discontinued treatment permanently in the setting of grade 3 immediate hypersensitivity reaction during first cycle (at 75 mg/m2). The remaining 18 patients were able to receive treatment without a premedication. The incidence of peripheral sensory neuropathy was 34 %. Of note, no grade ≥3 peripheral neuropathy was observed in any of the treatment cohorts. No cardiac events were reported throughout the treatment period. The most common reason for study discontinuation was disease progression. No cumulative toxicity was seen in the patients receiving multiple cycles.
Pharmacokinetic results
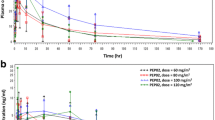
The PK parameters are listed in Table 4. Both ATI-1123 (encapsulated docetaxel) and free docetaxel were produced in vivo from the nanoparticle-associated liposomal preparation. ATI-1123 demonstrated linear and dose proportional PKs. Specific PK parameters are shown in Fig. 1. The PK exposure of encapsulated, non-encapsulated, and total docetaxel was dose proportional (Table 5). The value 1.00 was within the 90 % CI range for each C max and AUC. The encapsulated docetaxel, non-encapsulated docetaxel, and total docetaxel versus ATI-1123 dose suggested that both parameters were dose proportional (Table 5; Fig. 1). The encapsulated docetaxel exposure (C max and AUC) was ~2–3× higher than that of corresponding values for non-encapsulated (free) docetaxel. The non-encapsulated docetaxel had large volume of distribution with mean V ss ranging values from 47.0 ± 6.3 L/m2 (110 mg/m2 dose) to 104 L/m2 [30 mg/m2 dose; no SD since N = 1; Table 5]. The V ss values suggest apparent distribution in the whole body water and potential binding to other body tissues. The encapsulated docetaxel had a moderate volume of distribution with mean V ss values ranging from 13.7 ± 3.47 L/m2 (60 mg/m2 dose) to 18.7 ± 3.46 L/m2 (110 mg/m2 dose; Table 4). The V ss values suggest apparent distribution into the vascular and the interstitial fluid compartments.

a Mean plasma concentration–time profiles of encapsulated, non-encapsulated, and total docetaxel following 1-h infusion of ATI-1123. The encapsulated and non-encapsulated docetaxel plasma concentrations were summed together for each of the corresponding time points to calculate the total docetaxel concentration time profiles. The plasma concentrations of the three analytes increase as the dose of ATI-1123 increases. b The relationship between C max and AUC(0–inf) of total docetaxel versus ATI-1123 dose in human subjects following 1-h infusion of escalating doses of ATI-1123. Filed circles represent the actual data, solid lines represent the mean, and dashed lines represent the 90 % CI while. Data indicate linearity for both parameters (see also Table 3)
ATI-1123 appeared to have enhanced drug exposure as compared to the exposure of Taxotere® as reported by Loos et al. [12]. Table 6 compares the current study results with the results from Bruno et al. [13] at docetaxel dose of 100 mg/m2 [13]. The CL and T 1/2 values determined in the current study are consistent with the values reported by Bruno et al. [13]. Docetaxel exposure as measured by the C max and AUC in the current study appeared to be higher than the values reported by Bruno et al. [13]. In addition, the current study also showed encapsulated docetaxel exposure 2–3× higher than that of corresponding values for (free) docetaxel, which may be attributed to the reduced clearance of encapsulated docetaxel (Fig. 1). Consequently, encapsulated docetaxel could be considered as in depo source for non-encapsulated (free) docetaxel.
Antitumor activity results
One of the 29 evaluable patients demonstrated a partial response as defined by RECIST version 1.1 (Fig. 2a). This subject with non-small cell lung carcinoma previously treated with docetaxel was enrolled at MTD and had a time to disease progression of 30 weeks. Twenty-two patients (75 %) had SD as their best response at 6-week assessment. Among patients with SD, significant treatment induced tumor size reduction was observed (lung—19.6 %, pancreas—12.2 %, pancreas—12 %, lung—11 %). This also includes a pancreatic cancer subject, treated at MTD, achieving a 29.4 % reduction in tumor size from baseline. Eight patients had prolonged SD lasting more than 15 weeks. Two prostate cancer patients had robust PSA response (>95 % reduction) following multiple treatment cycles, including one patient who was progression free for 54 weeks. Figure 2b shows the percentage change in total lesion length from baseline for 19 patients with measureable lesions.

Antitumor activity of ATI-1123. a Non-small cell lung cancer patient with partial response (PR). b Patient response summary in 19 patients with measurable disease
The treatment results achieved with ATI-1123 were durable and maintained with minimal toxicity. Three out of a total of five patients with prostate cancer were able to receive ≥15 cycles of therapy. The maximum number of cycles administered was 21, which occurred in a 74-year-old subject with castrate-resistant prostate cancer who was treated with 30 mg/m2 dose. Three patients with non-small cell lung cancer treated at MTD dose level also received ≥5 cycles.
Of the nine subjects in this study with prior Taxotere® exposure, one confirmed PR (as described above) and five cases of SD were observed (prostate and pancreatic cancer). This included two subjects (one at MTD and one at 60 mg/m2) who had primary Taxotere® resistance as evident by previously documented disease progression. When treated with ATI-1123, they both had SD lasting >30 weeks.
Discussion
Docetaxel is a semisynthetic taxoid and targets intracellular tubulin. It is currently the standard of care for the treatment of several malignancies and is administered once every 3 weeks. Taxotere® is a commercially available docetaxel formulation with Tween 80, a carrier that enhances its solubility in water for intravenous administration [5]. This complicated drug delivery can alter drug pharmacokinetics, and the use of Tween 80 is associated with adverse events such as hypersensitivity reactions, nausea, fatigue, and anemia [12]. Liposomal docetaxel represents a new class of chemotherapy delivery system that may improve the therapeutic index of docetaxel.
This clinical trial was conducted to examine the MTD, PK properties, and spectrum of toxic effects associated with ATI-1123. The liposomal formulation of docetaxel was manageable overall with an acceptable safety profile as most reported AEs were either grade 1 or grade 2. Only two patients experienced a DLT during the first treatment cycle, at maximally administered dose (MAD), consisting of grade 3 stomatitis and febrile neutropenia. Peripheral neuropathy was only ≤2 in severity, and no cumulative neurotoxicity was apparent in the patients receiving multiple cycles. This appears quite favorable when compared to Taxotere® which is well known to cause dose-dependent and sometimes disabling neuropathy [14]. The incidence of peripheral edema was low (38 %) as compared to Taxotere® [15]. Hypersensitivity reactions were generally mild, low grade, and successfully managed with prolongation in infusion time or premedication. Our results show that ATI-1123 can indeed be administered safely as a short infusion over 1 h without dexamethasone or antihistamine premedication. Although direct comparison to Taxotere® administered at this schedule is not possible, the AEs induced by ATI-1123 appeared to be less severe than that reported for Taxotere® infusions. Thus, it appears to offer advantages in terms of safety (avoidance of hypersensitivity reactions), morbidity (avoidance of dexamethasone premedication), patient convenience and comfort (less time spent in the treatment center), and therefore decrease in cost of therapy.
Although objective PR rate was low in this trial, many heavily pretreated patients demonstrated reduction in target lesions on imaging studies. Anticancer activity was even observed in patients who had previously progressed during or shortly after receiving docetaxel-based chemotherapy. Among nine patients with prior Taxotere® exposure, six patients demonstrated efficacy signal with either PR or SD. This observation would support within the limitations of a Phase I study that ATI-1123 has activity in subjects with primary or secondary Taxotere® resistance. This finding should be further explored in larger studies.
Recently a multicenter, Phase I study using a different formulation of liposomal encapsulated docetaxel (LE-DT) in patients with advanced solid tumors reported similar antitumor and toxicity results [16]. The recommended Phase 2 dose of LE-DT was 85 mg/m2, which was safely escalated to 110 mg/m2 with G-CSF support. The toxicity profile of LE-DT included neutropenia, anemia, and fatigue. There was no significant peripheral neuropathy observed with LE-DT.
ATI-1123 demonstrated linear and dose proportional PKs. The CL and T 1/2 values determined in the current study are consistent with the values reported by Bruno et al. Docetaxel exposure as measured by the C max and AUC in the current study appeared to be higher than the values reported previously. In addition, the current study showed encapsulated docetaxel exposure was 2–3-folds higher than that of corresponding values for (free) docetaxel, which may be attributed to the reduced clearance of encapsulated docetaxel. The non-encapsulated docetaxel had large volume of distribution as compared to encapsulated docetaxel.
In conclusion, ATI-1123 is a novel albumin-stabilized liposomal docetaxel formulation that demonstrated an acceptable tolerability, a favorable PK profile as well as promising antitumor activity, and warrants further exploration in larger Phase 2 trials.
References
Dumontet C, Sikic BI (1999) Mechanisms of action of and resistance to anti-tubulin agents: microtubule dynamics, drug transport, and cell death. J Clin Oncol 17(3):1061–1070
Ajani JA, Moiseyenko VM, Tjulandin S, Majlis A, Constenla M, Boni C, Rodrigues A, Fodor M, Chao Y, Voznyi E, Marabotti C, Van Cutsem E (2007) Clinical benefit with docetaxel plus fluorouracil and cisplatin compared with cisplatin and fluorouracil in a phase III trial of advanced gastric or gastroesophageal cancer adenocarcinoma: the V-325 Study Group. J Clin Oncol 25(22):3205–3209. doi:10.1200/jco.2006.10.4968
Blohmer JU, Schmid P, Hilfrich J, Friese K, Kleine-Tebbe A, Koelbl H, Sommer H, Morack G, Wischnewsky MB, Lichtenegger W, Kuemmel S (2010) Epirubicin and cyclophosphamide versus epirubicin and docetaxel as first-line therapy for women with metastatic breast cancer: final results of a randomised phase III trial. Ann Oncol 21(7):1430–1435. doi:10.1093/annonc/mdp585
Burstein HJ, Manola J, Younger J, Parker LM, Bunnell CA, Scheib R, Matulonis UA, Garber JE, Clarke KD, Shulman LN, Winer EP (2000) Docetaxel administered on a weekly basis for metastatic breast cancer. J Clin Oncol 18(6):1212–1219
Taxotere (docetaxel) injection concentrate. Full prescribing information 2013
Rivera E, Mejia JA, Arun BK, Adinin RB, Walters RS, Brewster A, Broglio KR, Yin G, Esmaeli B, Hortobagyi GN, Valero V (2008) Phase 3 study comparing the use of docetaxel on an every-3-week versus weekly schedule in the treatment of metastatic breast cancer. Cancer 112(7):1455–1461. doi:10.1002/cncr.23321
Drummond DC, Meyer O, Hong K, Kirpotin DB, Papahadjopoulos D (1999) Optimizing liposomes for delivery of chemotherapeutic agents to solid tumors. Pharmacol Rev 51(4):691–743
Immordino ML, Dosio F, Cattel L (2006) Stealth liposomes: review of the basic science, rationale, and clinical applications, existing and potential. Int J Nanomed 1(3):297–315
Klamerus KJ, Maloney K, Rudolph RL, Sisenwine SF, Jusko WJ, Chiang ST (1992) Introduction of a composite parameter to the pharmacokinetics of venlafaxine and its active O-desmethyl metabolite. J Clin Pharmacol 32(8):716–724
Gough K, Hutchison M, Keene O, Byrom B, Ellis S, Lacey L, McKellar J (1995) Assessment of dose proportionality: report from the statisticians in the pharmaceutical industry/pharmacokinetics UK joint working party. Drug Inf J 29:1039–1048
Smith TJ, Khatcheressian J, Lyman GH, Ozer H, Armitage JO, Balducci L, Bennett CL, Cantor SB, Crawford J, Cross SJ, Demetri G, Desch CE, Pizzo PA, Schiffer CA, Schwartzberg L, Somerfield MR, Somlo G, Wade JC, Wade JL, Winn RJ, Wozniak AJ, Wolff AC (2006) 2006 update of recommendations for the use of white blood cell growth factors: an evidence-based clinical practice guideline. J Clin Oncol 24(19):3187–3205. doi:10.1200/jco.2006.06.4451
Loos WJ, Baker SD, Verweij J, Boonstra JG, Sparreboom A (2003) Clinical pharmacokinetics of unbound docetaxel: role of polysorbate 80 and serum proteins. Clin Pharmacol Therm 74(4):364–371. doi:10.1016/s0009-9236(03)00222-4
Bruno R, Riva A, Hille D et al (1997) Pharmacokinetic and pharmacodynamic properties of docetaxel: results of phase I and phase II trials. Am J Health Syst Pharm 54(24 Suppl 2):S16–S19
Hilkens PH, Verweij J, Stoter G, Vecht CJ, van Putten WL, van den Bent MJ (1996) Peripheral neurotoxicity induced by docetaxel. Neurology 46(1):104–108
Behar A, Pujade-Lauraine E, Maurel A, Brun MD, Chauvin FF, Feuilhade de Chauvin F, Oulid-Aissa D, Hille D (1997) The pathophysiological mechanism of fluid retention in advanced cancer patients treated with docetaxel, but not receiving corticosteroid comedication. Br J Clin Pharmacol 43(6):653–658
Deeken JF, Slack R, Weiss GJ, Ramanathan RK, Pishvaian MJ, Hwang J, Lewandowski K, Subramaniam D, He AR, Cotarla I, Rahman A, Marshall JL (2013) A phase I study of liposomal-encapsulated docetaxel (LE-DT) in patients with advanced solid tumor malignancies. Cancer Chemother Pharmacol 71(3):627–633. doi:10.1007/s00280-012-2048-y
Bruno R, Hille D, Riva A et al (1998) Population pharmacokinetics/pharmacodynamics of docetaxel in phase II studies in patients with cancer. J Clin Oncol 16(1):187–196
Acknowledgments
The authors wish to express their deep appreciation to Ms. Susan Beardslee for reviewing the manuscript and providing very valuable comments. This study was sponsored by Azaya Therapeutics.
Conflict of interest
None to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mahalingam, D., Nemunaitis, J.J., Malik, L. et al. Phase I study of intravenously administered ATI-1123, a liposomal docetaxel formulation in patients with advanced solid tumors. Cancer Chemother Pharmacol 74, 1241–1250 (2014). https://doi.org/10.1007/s00280-014-2602-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-014-2602-x