
Abstract
Purpose
Leptomeningeal carcinomatosis is a devastating complication of malignant disease. In this study, we evaluated the safety and pharmacokinetics of intrathecally administered pemetrexed in rats.
Methods
Three levels of pemetrexed (0.3, 1, and 3 mg/kg) were administered to 15 rats per level (45 rats in total) twice a week for 2 weeks through specifically designed indwelling subarachnoid catheters. Presence of clinical and pathological neurotoxicity was evaluated. To evaluate the pharmacokinetics of pemetrexed, independent cohorts of 30 rats were treated with 1 mg/kg of pemetrexed and its concentration in cerebrospinal fluid (CSF) and blood was measured using UPLC/MS/MS.
Results
There were no cases of clinical or pathologic neurotoxicity after intrathecal administrations of pemetrexed at levels of 0.3 and 1 mg/kg; however, 5 of 15 (33%) rats died after administration of 3 mg/kg pemetrexed. The distribution/elimination of pemetrexed in CSF was best described by a two-compartment model, with initial and terminal half-lives of 0.43 and 1.43 h, respectively. The predicted maximal concentration in CSF was 588 μM, and high levels of pemetrexed appeared to be maintained for a long time. Area under the curve and volume of distribution at steady state were 560 μM h and 1.14 ml, respectively.
Conclusions
The no observed adverse effect level of intrathecal administration of pemetrexed was 1 mg/kg in rats. At this level, therapeutically high and durable pemetrexed concentrations could be achieved. Based on these results, further research on intrathecal pemetrexed in humans or non-human primates should be considered.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Leptomeningeal carcinomatosis (LMC) represents a devastating complication of malignant disease with a dismal prognosis. In contrast to the real and significant improvements in overall survival in cancer patients seen with newly developed antitumor agents over the past few decades [6, 15], the median overall survival of patients with LMC has remained relatively constant at 2.4–5.8 months [8, 34].
Intravenous administration of conventional doses of antitumor agents cannot adequately penetrate into cerebrospinal fluid (CSF), and thus, treatment of LMC is usually performed by direct intrathecal administration of drugs, with a few drugs such as methotrexate being currently used for such intrathecal use [2, 20]. Although many agents or modalities have been investigated to overcome the poor outcomes of the current treatment for LMC, they continue to be unsatisfactory [4, 14, 16]. Specifically, the dismal prognosis of LMC can be in part attributed to a lack of efficient intrathecal antitumor agents. However, it is possible that any cytotoxic drug could be candidate for the intrathecal use, particularly drug with activity against the primary tumor, if the substantial potential for neurotoxicity associated with intrathecal administration could be avoided.
Pemetrexed is an antifolate antimetabolite that targets at least three enzymes including thymidylate synthase, dihydrofolate reductase, and glycinamide ribonucleotide formyltransferase. It is conceivable that the inhibitory effect brought about by targeting these three enzymes at multiple cancer sites would give rise to a broader spectrum of antitumor effects compared with methotrexate. In cell culture and clinical studies, pemetrexed shows cytotoxicity in a variety of tumors, including mesothelioma, non-small cell lung cancer (NSCLC), breast, cervical, colorectal, head and neck, bladder, and leukemia [9, 13, 21, 25, 29]. Given that the most frequent tumors metastasizing into the leptomeninges are NSCLC and breast cancer [8, 33], the potential for pemetrexed to be effective in treating LMC is highly encouraging. Furthermore, this drug has significant activity in cell lines and xenografts that are resistant to methotrexate [28]. Together, these findings suggest that pemetrexed may be also useful in LMC refractory to methotrexate. However, as is the case for methotrexate, pemetrexed concentrations in CSF are very low after systemic administration [10, 20, 30]. Therefore, intrathecal administration of pemetrexed should be investigated as a way to overcome its limited CSF penetration.
We conducted a preclinical study in rats to evaluate the relevance of intrathecal pemetrexed therapy. We first identified the no observed adverse effect level (NOAEL) of intrathecally administered pemetrexed in rats. We then performed pharmacokinetic studies at the NOAEL dose to estimate how long pemetrexed concentrations in CSF could be maintained at therapeutically relevant levels.
Materials and methods
All experimental procedures were in accordance with the guidelines approved by our institutional animal care committee. Adult male Sprague–Dawley rats (340–380 g) were purchased from the OrientBio inc. (South Korea). Rats were singly housed in an animal room with a controlled temperature (24–25°C) and 12 h light–dark cycle, with access to standard laboratory rat chow and tap water.
Catheterization of the spinal subarachnoid space
A modified form of the catheterization method described by Poon et al. [23] was used in this study. Figure 1 illustrates the basic components of the intrathecal catheter. Briefly, we modified 10-cm-long PE-20 catheters (inner and outer diameters of 0.38 and 1.09 mm, respectively) for the intrathecal use. One end of the catheter was heated and stretched to a thinner 1 cm end length (outer diameter 0.45 mm). Next, a joint was made between the stretched and unstretched catheter with a ball-like appearance (bead) using heat and elaborate compression in order to form a functional cap and anchorage point for placement through a bone hole.

An illustration of the subarachnoid catheter. The joint portion between the stretched and unstretched catheter was made such that it had a ball-like appearance (bead)
Rats were anesthetized with pentobarbital sodium (50 mg/kg, intraperitoneally). Next, a rectangular area of the skin above the T9 to L2 vertebrae was shaved and sterilized with povidone iodine. A midline incision was then made, and paravertebral muscles attached to the left side of the T12 to L1 vertebrae were reflected from the spinous processes. A small hole was made over the exposed left T13 lamina proper with small hand drill (Strong 207B, Saeshin, South Korea) equipped with a carbide burr (Prima Classic HP557, Prodenti, England) until the bone was nearly punctured (Fig. 2a). The hole was further excavated carefully with a 3-ml syringe fitted with a 26-s gauge needle until the lamina and dura were thoroughly punctured (Fig. 2b). Successful dura puncture was denoted by visible leakage of clear CSF. The previously made catheter was then filled with 0.9% NaCl, inserted caudally, and advanced as gently as possible until the bead was lodged on the hole of the vertebra (Fig. 2c). The small portion cut from vertebral muscle was then applied over the bead (Fig. 2d), and tissue glue (Histoacryl; B. Braun, Germany) was dropped over the muscle (Fig. 2e) to prevent the leakage of CSF and movement of the catheter. Another second skin incision was made above the upper T-spine area, and the other end of the catheter was made to exit via the incision after being passed through the subcutaneous area (Fig. 2f). The buried portion of the catheter under the skin was further secured on the fascia of paravertebral muscle with sutures. The exterior end of the catheter was closed with tube sealant (Sure-Seal, Baxter, US). The skin wound was then closed in layers, and rats were injected subcutaneously with enrofloxacin (10 mg/kg). Animals were returned to the animal room for postoperative recovery in individual cages.

Illustration of the procedures used for implantation of the subarachnoid catheter. a Thoracic vertebra showing the position of the hole for catheter insertion. b–e Longitudinal section view of T13 lamina at the hole showing the key steps in insertion, anchorage, and fixation of the catheter. f The schematic illustration of the catheter exiting after subcutaneous tunneling and sutures to increase the stability of the catheter
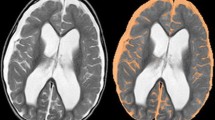
The proper placement of the catheter tip in the subarachnoidal space was confirmed in a subset of rats by five successive intrathecal administrations of 20 μl of contrast medium 10 min apart. Radiographs of the animals were taken in the prone position 5 min after each dosing, and the distribution of the contrast medium in the subarachnoid space was recorded. The distribution of contrast media was identified to be confined within the subarachnoid space and to increase with repeated injections (Fig. 3). All experimental procedures described later for toxicity and pharmacokinetic studies were performed after confirming no catheter-related adverse events during a 24-h observation period after catheter insertion.

Roentgenological images before and after injections of contrast medium of 20 μl, given 10 min apart. Arrows indicate both ends of the distribution of contrast medium
Toxicity study
Before conducting toxicity screening for pemetrexed, we evaluated the safety of the intrathecal catheter and determined a safely administrable volume. Five rats were intrathecally administered four times with 0.1 ml 0.9% NaCl solution every 3 days. No abnormal neurologic behavior was observed and body weights increased up to our expectations for 17 days, from the day of the catheter insertion to the seventh day after the last injection (mean 98 ± 15 g).
Evaluation of toxicity of repetitive intrathecal administration of pemetrexed was performed at three concentration levels (0.3, 1, and 3 mg/kg). After appropriate anesthetic procedures, each concentration level of pemetrexed in 0.1 ml 0.9% NaCl solution was slowly injected over 20 min into 15 rats (45 rats in total) every 3 or 4 days (four times in total). Animals were closely monitored following drug administration and daily for up to 7 days after the last administration. Body weights were followed up regularly throughout the study period.
Adverse neuropathologic effects were also analyzed by the histopathologic examination. One randomly chosen rat that survived after completion of toxicity testing at each pemetrexed level and all of the rats that showed signs of adverse effects of pemetrexed were sacrificed by an overdose of halothane by inhalation. The entire neuraxis was then removed and fixed in buffered neutral formalin for 7–10 days and placed in a decalcifying solution. Two representative sections, taken from the brain and the spinal cord at the thoracic level, were obtained from each animal. Sections were embedded in paraffin, and 6-μm sections were stained with Bodian silver, Luxol fast blue, and hematoxylin and eosin, and all the slides were examined under a light microscopy by a neuropathologist (YLS).
Pharmacokinetic study
Intrathecal pharmacokinetic studies were performed on an independent cohort comprised of 30 rats. The amount of administration for the pharmacokinetic study was 1 mg of pemetrexed per kg of baseline rat weight (1 mg/kg), which was based on the results from the toxicity study. After being anesthetized with pentobarbital sodium (50 mg/kg), all rats were intrathecally administered with pemetrexed (1 mg/kg) in a 0.1 ml 0.9% NaCl solution over 20 min.
CSF and blood were sampled from five rats at each of six time points (0.75, 2, 4, 6, 10, and 24 h). CSF samples were taken from the cistern magna by placing a needle through the muscle layer overlying the atlanto-occipital membrane. Briefly, anesthetized rats were placed in a stereotactic frame for CSF sampling. The back of the head and neck was shaved, prepared and draped in sterile conditions, and a 250-μl Hamilton syringe with a 26-s gauge needle was advanced horizontally through a 1-cm incision made in the skin at the level of the cisterna magna, until the dura was punctured. Slight negative pressure was applied to the syringe until CSF (approximately 50–100 μl) was obtained. After sampling of CSF, rats were dissected and blood specimens were obtained from an inferior vena cava puncture, after which the animals were allowed to exsanguinate completely to death.
Pemetrexed concentrations in plasma and CSF sample were analyzed by ultra performance liquid chromatography mass spectroscopy/tandem mass spectroscopy (UPLC/MS/MS) using the methodof Churchwell et al. [7] with minor modification. The calibration curves were linear (r 2 > 0.99) over the ranges of 20–5,000 ng/ml for serum and 30–5,000 ng/ml for CSF samples. Intra- and inter-assay imprecisions were less than CV 10%. Quantitative analysis was performed in the multiple reaction monitoring mode (m/z 428.0 > 281.0 for pemetrexed and 455.0 > 308.0 for internal standard, methotrexate).
Results
Toxicity assessment
The toxicities of pemetrexed administered by repetitive intrathecal injections are shown in Table 1. There was no clinical or pathologic neurotoxicity during or after 4 successive (twice a week for 2 weeks) administrations of pemetrexed at the levels of 0.3 and 1 mg/kg. The average weight gain for 17 days was 96 ± 14 and 82 ± 17 g at 0.3 and 1 mg/kg, respectively. Five out of 15 rats given pemetrexed at a level of 3 mg/kg died while showing hyperactive and abnormal movements (turning, screaming, etc.) within 10 min after the first (four rats) and second (one rat) injection. However, neuropathologic analyses for these five rats revealed no specific abnormality accountable for the death. For the other 10 rats at the level of 3 mg/kg, there was no significant clinical adverse event and the average weight gain for 17 days was 64 ± 10 g. For all histologically evaluated rats, including both deceased and surviving rats, there was no evidence of neuronal loss, demyelination, ventriculitis, ependymitis, or vasculitis attributable to pemetrexed administration (Fig. 4).

Histopathologic analysis of a deceased rat after intrathecal pemetrexed injection. a No evidence of neuronal cell damage in hippocampus (hematoxylin and eosin stain). b No evidence of axonalopathy (Bodian silver satin). c No evidence of myelinopathy (Luxol fast blue stain)
Pharmacokinetic analysis
As was the case in the toxicity study, intrathecal pemetrexed at a level of 1 mg/kg was well tolerated in all 30 animal subjects. Further, there was no clinical evidence of neurotoxicity associated with intrathecally injected pemetrexed at this dose. However, one pair of blood and CSF samples could not be taken because one rat died of an intracranial hemorrhage caused by a ruptured vessel during CSF sampling at the 6-h time point. Therefore, pharmacokinetic analysis was performed on pairs of blood and CSF samples in a total of 29 rats.
Data of the mean concentrations in CSF and plasma at each time point are shown in Table 2. Based on the mean concentrations, the predicted maximal concentration (Cmax at time zero), area under the concentration versus time curve (AUC), clearance, steady-state volume of distribution (Vss), and mean residence time (MRT) in CSF and plasma were calculated using non-compartment methods (Table 3). In CSF, a Cmax of 588 μM was achieved with an AUC of 560 μM h and Vss of 1.14 ml. In plasma, the Cmax was 6.88 μM with an AUC of 10.8 μM h and Vss of 166 ml. The AUCcsf and AUCplasma were 560 and 10.8 μM h, respectively, leading to a penetration from CSF to plasma (AUCplasma/AUCcsf) of 1.9%. Figure 5 shows the CSF and plasma concentration–time curves as logarithmic means. The distribution/elimination of pemetrexed in CSF decreased in parallel with that in plasma and could be best explained by a two-compartment model. Based on the mean CSF concentrations, half-lives for the initial distribution/elimination and terminal elimination phase were 0.43 and 1.43 h, respectively.

Cerebrospinal fluid and plasma concentration–time curves of pemetrexed following intrathecal administration at a dose of 1 mg/kg
Discussion
Leptomeningeal carcinomatosis is invariably frustrating for physicians and lethal for patients since conventional therapy offers no meaningful chance of cure. Systemic chemotherapy can be an effective intervention, but the limited delivery to the leptomeninges of intravenously administered drugs, coupled with the systemic toxicity associated with intravenous therapy, significantly limits this approach. Direct administration of chemotherapeutic agents such as methotrexate into the subarachnoid space minimizes systemic toxicity; however, the chronic uses of agents that have limited antitumor activity are associated with profound neurotoxicity. Therefore, new approaches that use an intrathecal route to administer novel drugs with a high therapeutic index might represent a major clinical advance for patients with LMC. Given that intrathecal pemetrexed could be candidate for LMC based on data generated from previous preclinical and clinical studies, we performed toxicity and pharmacokinetic studies on intrathecal pemetrexed administration in rats.
In our toxicity study, no adverse events occurred at levels of 0.3 and 1 mg/kg, while at a level of 3 mg/kg, 33% (five out of 15 rats) died. Therefore, the NOAEL was identified as 1 mg/kg pemetrexed. However, several studies previously described that intrathecal chemotherapy induced cognitive or behavioral dysfunction as well as evident neurotoxicities, by showing that neurologically damaged rats had shortened escape latency and searching distance [18, 22, 26]. In the present study, we did not evaluate a delicate difference of cognitive or behavioral function. However, no significant difference in the weight change, between the group of pemetrexed 1 mg/kg and the group of 0.1 ml normal saline, indicated there were no significant early cognitive or behavioral changes.
Although the causes of deaths at the 3 mg/kg level were unclear even after histologic analysis, they may have been caused by dose-dependent neurotoxicity, because we did not observe any adverse events at the two lower dose levels and the five deaths occurred acutely. The reason that we could not find any histologic abnormality in deceased rats can be caused by that we did not use the optimal staining methods. Many experimental studies were investigated to detect the minute or delayed neurotoxicities using amino-cupric silver stain, Ki-67 [1, 3, 11, 27]. Further, no observable neuropathologic abnormality could be explained in part by the shortage of time for any histologic change.
In addition, we found that as much as 100 μl of fluid could be administered safely to the rats through an indwelling subarachnoid catheter. Previous studies have shown that intrathecal injections of volumes of 20–30 μl are well tolerated in rats [17]. However, one study showed that the extent of intrathecal distribution of drugs is proportional to the administered drug volume [23]. A similar phenomenon was observed in our study. Specifically, the extent of distribution increased as the 20 μl of contrast media was injected repetitively. Therefore, a large volume injection was needed to guarantee even distribution of pemetrexed in the subarachnoid space, and we identified that 100 μl of 0.9% NaCl could be safely administered intrathecally. Based on this observation, further experiments in our study were performed with an injection volume of 100 μl, which did not cause any adverse events.
The IC50 for pemetrexed was previously shown to range from 9.3 nM to 4.3 μM, with a median IC50 value of 0.191 μM based on studies in various NSCLC cell lines [5]. In our pharmacokinetic study following a dose of 1 mg/kg, high pemetrexed concentrations were maintained in CSF for a long time. It is of note that the Cmax was 588 μM and the pemetrexed concentration in CSF at 24 h after injection was 0.143 μM, which is close to the median IC50 value in NSCLC cell lines. A previous study showed that the CSF penetration of pemetrexed is about 0.76% following intravenous administration to monkeys [30]. Considering that the AUCplasma after intravenous administration of a conventional dose of pemetrexed (500 mg/m2) to humans was 264 μM h, and the CSF penetrations of drugs are very similar between monkeys and humans [19, 24], the predicted AUCCSF in human following intravenous administration of the conventional pemetrexed dose would be 2.0 μM h (264 μM h × 0.76%), which is much lower than the AUCCSF (560 μM h) observed in our study. Therefore, the treatment of LMC may be more effective with direct intrathecal administration of much lower doses of pemetrexed than with intravenous administration, because the cytotoxicity of pemetrexed has been previously demonstrated to be dependent on both concentration and exposure time [12].
In this study, a 1 mg/kg dose (mean 0.35 mg per rat with mean weight of 0.35 kg) of intrathecal pemetrexed was found to be safe and capable of delivering a therapeutically durable concentration in rats. Based on these results, we estimated the starting dose in humans or non-human primates for future studies. For drugs administered into the intrathecal space, which has little subsequent distribution outside of the subarachnoid space, dosage should be adjusted according to the compartment volume and concentration of the drugs, not according to the body surface area among different species [31]. The total CSF volumes of rats, monkeys, and human are known to be approximately 0.4, 13, and 140 ml [24, 32]. Therefore, 0.35 mg of pemetrexed resolved in 0.4 ml CSF plus 0.1 ml injected solution (total 0.5 ml) in rats corresponds to a dose of 9 and 98 mg of pemetrexed in CSF of monkeys and humans, respectively, with final concentration in CSF reaching 0.7 mg/ml. Taking one value between 10 and 20 for the safety coefficient, the optimal starting dose of pemetrexed between 5 and 10 mg for human studies should be considered.
To our knowledge, this was the first study to investigate the possibility and therapeutic relevance of intrathecal pemetrexed therapy. Our findings could give some signals to many investigators finding new methods to overcome the intractable LMC and induce the development of new cancer animal models to evaluate the effectiveness of several drugs in the treatment of LMC.
In summary, 1 mg/kg pemetrexed can be safely administered to the subarachnoid space of rats. At this level, therapeutically relevant and durable pemetrexed concentrations could be achieved. Based on these results, further research on the use of intrathecal pemetrexed in humans or non-human primates should be considered.
References
Balaban CD, O’Callaghan JP, Billingsley ML (1988) Trimethyltin-induced neuronal damage in the rat brain: comparative studies using silver degeneration stains, immunocytochemistry and immunoassay for neuronotypic and gliotypic proteins. Neuroscience 26:337–361
Bleyer WA, Drake JC, Chabner BA (1973) Neurotoxicity and elevated cerebrospinal-fluid methotrexate concentration in meningeal leukemia. N Engl J Med 289:770–773
Bueno A, De Olmos S, Heimer L, De Olmos J (2003) NMDA-antagonist MK-801-induced neuronal degeneration in Wistar rat brain detected by the Amino-Cupric-Silver method. Exp Toxicol Pathol 54:319–334
Chamberlain MC, Kormanik P, Howell SB, Kim S (1995) Pharmacokinetics of intralumbar DTC-101 for the treatment of leptomeningeal metastases. Arch Neurol 52:912–917
Chan DC, Chen V, Helfrich B, Zhang Z, Hirsch F, Ma D, Bunn P (2006) Preclinical studies of pemetrexed and gemcitabine, alone and in combinations, in human lung cancers. AACR Meeting Abstracts 2006:1278b
Chu KC, Tarone RE, Kessler LG, Ries LAG, Hankey BF, Miller BA, Edwards BK (1996) Recent trends in US breast cancer incidence, survival, and mortality rates. J Natl Cancer Inst 88:1571–1579
Churchwell MI, Twaddle NC, Meeker LR, Doerge DR (2005) Improving LC-MS sensitivity through increases in chromatographic performance: comparisons of UPLC-ES/MS/MS to HPLC-ES/MS/MS. J Chromatogr B 825:134–143
Clarke JLM, Perez HR, Jacks LMM, Panageas KSD, DeAngelis LMM (2010) Leptomeningeal metastases in the MRI era. Neurology 74:1449–1454
Cripps C, Burnell M, Jolivet J, Batist G, Lofters W, Dancey J, Iglesias J, Fisher B, Eisenhauer EA (1999) Phase II study of first-line LY231514 (multi-targeted antifolate) in patients with locally advanced or metastatic colorectal cancer: an NCIC clinical trials group study. Ann Oncol 10:1175–1179
Dai H, Chen Y, Elmquist WF (2005) Distribution of the novel antifolate pemetrexed to the brain. J Pharmacol Exp Ther 315:222–229
de Olmos JS, Beltramino CA, de Lorenzo S (1994) Use of an amino-cupric-silver technique for the detection of early and semiacute neuronal degeneration caused by neurotoxicants, hypoxia, and physical trauma. Neurotoxicol Teratol 16:545–561
Giovannetti E, Mey V, Nannizzi S, Pasqualetti G, Marini L, Del Tacca M, Danesi R (2005) Cellular and pharmacogenetics foundation of synergistic interaction of pemetrexed and gemcitabine in human non–small-cell lung cancer cells. Mol Pharmacol 68:110–118
Hanna N, Shepherd FA, Fossella FV, Pereira JR, De Marinis F, von Pawel J, Gatzemeier U, Tsao TCY, Pless M, Muller T, Lim H-L, Desch C, Szondy K, Gervais R, Shaharyar S, Manegold C, Paul S, Paoletti P, Einhorn L, Bunn PA Jr (2004) Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy. J Clin Oncol 22:1589–1597
Hitchins R, Bell D, Woods R, Levi J (1987) A prospective randomized trial of single-agent versus combination chemotherapy in meningeal carcinomatosis. J Clin Oncol 5:1655–1662
Kim HS, Park K, Jun HJ, Yi SY, Lee J, Ahn JS, Park YH, Kim S, Lee S, Ahn MJ (2009) Comparison of survival in advanced non-small cell lung cancer patients in the pre- and post-gefitinib eras. Oncology 76:239–246
Kooistra KL, Rodriguez M, Powis G (1989) Toxicity of intrathecally administered cytotoxic drugs and their antitumor activity against an intrathecal walker 256 carcinosarcoma model for meningeal carcinomatosis in the rat. Cancer Res 49:977–982
Kooistra KL, Rodriguez M, Powis G, Yaksh TL, Harty GJ, Hilton JF, Laws ER (1986) Development of experimental models for meningeal neoplasia using intrathecal injection of 9L gliosarcoma and walker 256 carcinosarcoma in the rat. Cancer Res 46:317–323
Li F, Gong Q-H, Wu Q, Lu Y-F, Shi J-S (2010) Icariin isolated from Epimedium brevicornum maxim attenuates learning and memory deficits induced by d-galactose in rats. Pharmacol Biochem Behav 96:301–305
Nakagawa K, Kudoh S, Matsui K, Negoro S, Yamamoto N, Latz JE, Adachi S, Fukuoka M (2006) A phase I study of pemetrexed (LY231514) supplemented with folate and vitamin B12 in Japanese patients with solid tumours. Br J Cancer 95:677–682
Pavlidis N (2004) The diagnostic and therapeutic management of leptomeningeal carcinomatosis. Ann Oncol 15(Suppl 4):iv285–iv291
Paz-Ares L, Bezares S, Tabernero JM, Castellanos D, Cortes-Funes H (2003) Review of a promising new agent—pemetrexed disodium. Cancer 97:2056–2063
Phillips PC, Thaler HT, Allen JC, Rottenberg DA (1989) High-dose leucovorin reverses acute high-dose methotrexate neurotoxicity in the rat. Ann Neurol 25:365–372
Poon YYM, Chang AYWP, Ko SFM, Chan SHHP (2005) An improved procedure for catheterization of the thoracic spinal subarachnoid space in the rat. Anesth Analg 101:155–160
Poplack DG, Bleyer WA, Wood JH, Kostolich M, Savitch JL, Ommaya AK (1977) A primate model for study of methotrexate pharmacokinetics in the central nervous system. Cancer Res 37:1982–1985
Schultz RM, Patel VF, Worzalla JF, Shih C (1999) Role of thymidylate synthase in the antitumor activity of the multitargeted antifolate, LY231514. Anticancer Res 19:437–443
Schunior A, Mullenix PJ, Zengel AE, Landy H, Howes A, Tarbell NJ (1994) Radiation effects on growth are altered in rats by prednisone and methotrexate. Pediatr Res 35:416–423
Seigers R, Schagen SB, Beerling W, Boogerd W, van Tellingen O, van Dam FSAM, Koolhaas JM, Buwalda B (2008) Long-lasting suppression of hippocampal cell proliferation and impaired cognitive performance by methotrexate in the rat. Behav Brain Res 186:168–175
Shih C, Chen VJ, Gossett LS, Gates SB, MacKellar WC, Habeck LL, Shackelford KA, Mendelsohn LG, Soose DJ, Patel VF, Andis SL, Bewley JR, Rayl EA, Moroson BA, Beardsley GP, Kohler W, Ratnam M, Schultz RM (1997) LY231514, a Pyrrolo[2, 3-d]pyrimidine-based antifolate that inhibits multiple folate-requiring enzymes. Cancer Res 57:1116–1123
Spielmann M, Martin M, Namer M, duBois A, Unger C, Dodwell DJ (2001) Activity of pemetrexed (ALIMTA, multitargeted antifolate, LY231514) in metastatic breast cancer patients previously treated with an anthracycline and a taxane: an interim analysis. Clin Breast Cancer 2:47–51
Stapleton SL, Reid JM, Thompson PA, Ames MM, McGovern RM, McGuffey L, Nuchtern J, Dauser R, Blaney SM (2007) Plasma and cerebrospinal fluid pharmacokinetics of pemetrexed after intravenous administration in non-human primates. Cancer Chemother Pharmacol 59:461–466
US Department of Health and Human Services, Food and Drug Administration, Center for Biologics Evaluation and Research. (2005) Guidance for industry: estimating the maximum safe starting dose in initial clinical trials for therapeutics in adult healthy volunteers. Pharmacology and Toxicology
van den Berg MP, Romeijn SG, Verhoef JC, Merkus FWHM (2002) Serial cerebrospinal fluid sampling in a rat model to study drug uptake from the nasal cavity. J Neurosci Methods 116:99–107
Waki F, Ando M, Takashima A, Yonemori K, Nokihara H, Miyake M, Tateishi U, Tsuta K, Shimada Y, Fujiwara Y, Tamura T (2009) Prognostic factors and clinical outcomes in patients with leptomeningeal metastasis from solid tumors. J Neurooncol 93:205–212
Wasserstrom WR, Glass JP, Posner JB (1982) Diagnosis and treatment of leptomeningeal metastases from solid tumors: experience with 90 patients. Cancer 49:759–772
Acknowledgments
The authors thank Ms. So Youn Lee (Laboratory Animal Research Center, Samsung Biomedical Research Institute) for assistance with animal studies. The author (MH Nam) drew figures 1 and 2. Grant Support: This work was supported by the Ministry of Health and Welfare, Republic of Korea (A040041) and a Samsung Biomedical Research Institute grant (CA71033).
Conflict of interest
No potential conflict of interest was disclosed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sun, JM., Nam, M.H., Chung, J.Y. et al. Safety and pharmacokinetics of intrathecal administration of pemetrexed in rats. Cancer Chemother Pharmacol 68, 531–538 (2011). https://doi.org/10.1007/s00280-010-1522-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-010-1522-7