
Abstract
Background
Dihydropyrimidine dehydrogenase (DPD) enzyme is responsible for the elimination of approximately 80% of administered dose of 5-FU. DPD deficiency has been associated with severe 5-FU toxicity. Syndrome of DPD deficiency manifests as diarrhea, stomatitis, mucositis, and neurotoxicity and in some cases death. This is a true pharmacogenetic syndrome, with symptoms being unrecognizable until exposure to the drug.
Patients and methods
A 75-year-old patient with metastatic pancreatic adenocarcinoma developed grade 4 thrombocytopenia, grade 3 coagulopathy, and grade 3 neurologic toxicity with a fatal outcome following administration of 5-FU. Due to pancytopenia, DPD activity could not be determined in peripheral blood mononuclear cells (PBMC) using a previously described radioassay. Therefore, screening and genotypic analysis of homozygous and heterozygous, known and unknown sequence variants, in the DPYD gene were performed using DHPLC as previously described. All DPYD sequence variants identified by DHPLC were confirmed by DNA sequencing using a dideoxynucleotide chain termination method and capillary electrophoresis on an ABI 310 Automated DNA Sequencer.
Results
Genotyping analysis of the DPYD gene revealed the presence of the heterozygous mutation, IVS14 + 1 G > A, DPYD*2A.
Conclusion
Genotypic analysis using DHPLC can be employed to screen DPD deficiency in a patient with severe neutropenia. The mutation IVS14 + 1 G > A, DPYD*2A, is the most common mutation associated with DPD deficiency. A G > A base change at the splice recognition sequence of intron 14, leads to exon skipping and results in a 165-bp deletion in the DPD mRNA. We have previously demonstrated that a homozygote DPYD*2A genotype results in complete deficiency while the heterozygous DPYD*2A genotype results in partial deficiency of DPD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fluorouracil (5-FU), an analog of uracil, is one of the most commonly used chemotherapeutic agents and constitutes the mainstay of chemotherapy for most gastrointestinal tumors [1]. The cytotoxicity of 5-FU is thought to be secondary to: (1) inhibition of thymidylate synthase (TS), principally via the actions of its metabolite, fluorodeoxyuridine monophosphate (FdUMP); and (2) synthesis of defective RNA as a result of incorporation of a second metabolite, fluorouridine triphosphate (FUTP), into RNA [2] (Fig. 1). The most common 5-FU toxicities include neutropenia, mucositis, diarrhea, and hand–foot syndrome, with the latter two adverse effects predominating when 5-FU is administered as a continuous intravenous (IV) infusion [3]. Like other conventional cytotoxic antineoplastic agents, 5-FU has a relatively narrow therapeutic index. Its toxicity often limits the dose that can be administered, limiting its overall therapeutic usefulness. Furthermore, since the late 1980s, there have been multiple case reports demonstrating unanticipated fatal and near fatal toxicities in patients with dihydrpyrimidine dehydrogenase (DPD) deficiency following intravenous and oral fluoropyrimidines [4–8].

80–85% of 5-FU is catabolized to inactive metabolites by DPD and only 1–3% of the 5-FU mediated cytotoxic effects on tumor cells and normal tissue through anabolic actions. Increased anabolism of 5-FU in patients with DPD deficiency
As DPD catalyzes the rate limiting step in the catabolic pathway of 5-FU, a deficiency of DPD can produce the clinical syndrome of 5-FU toxicity including mucositis, granulocytopenia, neuropathy, and death) [3]. Van Kuilenburg et al. [6] showed that cancer patients with 5-FU toxicity had a 59% reduced DPD activity. Johnson et al. [7] showed similar results, with 43% of these patients showing reduced DPD activity. The gene for DPD has been isolated to chromosome 1p22 (DPYD). Over 32 different DPYD alleles have been identified, the functional significance of most remains to be elucidated. Current efforts at screening for DPD are aimed at testing the DPD activity as opposed to screening for an actual genetic marker. We here present a patient with pancreatic cancer who developed severe toxicity following 5-FU and results of his genotype analysis of the DPYD gene.
Patients and methods
Patient
The patient was a 75-year-old Caucasian male with histologically confirmed metastatic pancreatic adenocarcinoma. His past medical history was remarkable for peripheral vascular disease requiring arterial bypass surgery of the right lower extremity 5 years prior. His medications included oxycontin, warfarin, alprazolam and zolpidem. He smoked one pack of cigarettes daily for over 50 years. The initial physical examination was notable for an ECOG performance status of 1; right upper quadrant tenderness and hepatomegaly. Initial laboratory evaluation revealed a white blood cell count of 11.1 × 103, hemoglobin 10.2 gm/dl, platelets 270 × 103, creatinine 1.4 mg/dl, AST 64 U/l, ALT 30 U/l, total bilirubin 0.6 mg/dl, alkaline phosphatase 299 U/L, CA 19-9 of 5743 U/ml and normal electrolytes.
He was treated with bolus 5-FU administered intravenously once weekly for 3 weeks followed by 1 week with no therapy. He tolerated two treatments with 5-FU without significant toxicity, except grade 1 nausea, grade 2 anemia and grade 1 thrombocytopenia. On the third week, however, he presented with generalized weakness, altered mental status, deterioration of his performance status to 3 and pancytopenia (white blood count 2.2 × 103 [grade 2]; hemoglobin 8.6 gm/dl [grade 2]; platelets 14 × 103 [grade 4]; INR 3.4 [grade 3]). Other laboratory abnormalities included grade 2 creatinine (2.4 mg/dl), grade 1 weight loss and grade 3 anorexia. He was admitted to the oncology unit for transfusion of red blood cells and platelets. In addition, the patient underwent an extensive workup to rule out an underlying infection, disseminated intravascular coagulation and gastrointestinal bleeding. Given the patient’s presentation of mental status changes and pancytopenia following 5-FU, DPD deficiency was a major diagnostic concern. 5-FU was stopped and blood was collected to isolate peripheral blood mononuclear cells (PBMC) to determine DPD activity but was not successful due to absence of sufficient PBMC. His mental status continued to decline to grade 3 and on hospital day four, he expired.
After obtaining informed consent, an autopsy was performed. Post-mortem examination was remarkable for moderately to poorly differentiated adenocarcinoma of the pancreatic body and tail with extensive metastatic spread to the liver, diaphragm and regional lymph nodes. Gastrointestinal examination revealed a perforated duodenal ulcer. Central nervous system examination revealed lacunar infarction, hypertensive small vessel disease and remote focal hemorrhage of the basis pontis. Post-mortem blood cultures were positive for Candida albicans as were tissue cultures from the duodenal ulcer.
DPYD genotyping
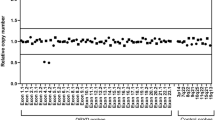
Screening and genotypic analysis of homozygous and heterozygous, known and unknown sequence variants, in the DPYD gene were performed using DHPLC as previously described [9]. DHPLC is a DNA screening method based on temperature-modulation heteroduplex separation of dsDNA containing mismatched base pairs. Heteroduplex DNA is generated by denaturing and reannealing a mixed population of reference wild-type samples and mutant DNA. Under conditions of partial heat denaturation (within a linear acetonitrile gradient), the heteroduplex fragments having internal sequence variations will have reduced column retention time relative to their homoduplex counterparts and will illustrate a melting pattern or a finger print characteristic of each sequence variant. In the DHPLC method, heteroduplexes are resolved without the use of radioactivity, acrylamide gel, or chemical denaturants [9].
All DPYD sequence variants identified by DHPLC were confirmed by DNA sequencing using a dideoxynucleotide chain termination method (Big Dye Kit; Applied Biosystems, Foster City, CA, USA) and capillary electrophoresis on an ABI 310 Automated DNA Sequencer (Applied Biosystems, Foster City, CA, USA) (Fig. 2).

DPYD genotyping. DHPLC and direct sequence analysis revealed the presence of the inactivating mutation, DPYD*2A
Results
Because of pancytopenia, DPD enzyme activity could not be assessed in the patient. Genotype analysis of the DPYD gene revealed the presence of the heterozygous mutation, IVS14 + 1 G > A, DPYD*2A, now recognized as the most common cause of DPD deficiency [10].
Discussion
This case demonstrates the importance of understanding the interplay between pharmacology and clinical medicine. Genotypic analysis using DHPLC was employed to screen DPD deficiency in this patient with severe neutropenia as DPD radioassay could not be performed due to lack of sufficient PBMC. The postmortem examination was significant for a perforated duodenal ulcer and candidemia that we believe were related to 5-FU-associated severe mucositis and prolonged neutropenia, respectively. In patients with severe DPD enzyme deficiency, even a small dose or a very short administration of 5-FU could lead to a marked surge in plasma 5-FU concentrations (C max), leading to increased 5-FU anabolism in susceptible tissues e.g. GI tract, hair, and bone marrow. Syndrome of DPD deficiency manifests as diarrhea, stomatitis, mucositis, and neurotoxicity and in some cases death [4, 5]. These individuals are at significant risk if they develop cancer and are given 5-FU.
To date, the more than 32 sequence variations in the DPYD gene have been described [9]. Yet, only DPYD*2A and DPYD*13 have been consistently associated with DPD deficiency. Genotypic screening for DPYD*2A may benefit only a limited number of cancer patients due to the low frequency of this variation in the general population (0.94% frequency in the Caucasian population [9].
The mutation IVS14 + 1 G > A, DPYD*2A, is the most common mutation associated with DPD deficiency. A G > A base change at the splice recognition sequence of intron 14, leads to exon skipping and results in a 165-bp deletion in the DPD mRNA [11]. We have previously demonstrated by genotype analysis of the DPYD gene that a homozygote DPYD*2A genotype results in complete deficiency while a heterozygote genotype results in partial deficiency of DPD [9].
Most assays that are currently available to detect this pharmacogenetic syndrome are too labor-and-time intensive to be routinely used to screen cancer patients prior to 5-FU administration [12]. Recently, we developed and validated an oral UraBT, which may potentially be used as a screening method to rapidly detect DPD deficiency in cancer patients prior to 5-FU administration [13]. This in vivo assay utilizes 2-13C-uracil (which has a similar substrate affinity for the DPD enzyme as 5-FU [14]. As the 2-13C-uracil substrate is degraded by DPD and other enzymes of the pyrimidine catabolic pathway, the 13C label is released as 13CO2. The 13CO2 present in breath can then be quantitated by infrared spectrophotometry. Previously, we demonstrated DPD deficient individuals have an impaired ability to catabolize the 2-13C-uracil, which results in altered 13CO2 breath profiles.
Options for DPD deficient patients are limited usually requiring discontinuation of 5-FU. Thymidine and uracil rescues have been reported inconsistently in 5-FU toxicity. The clinical feasibility of 5-FU dose escalation with PN401 has been demonstrated in preclinical and phase I studies [15–17]. However, no data on the effect of PN401 in DPD-deficient patients exist. Animal experiments with ethynyluracil in our laboratory have manifested that PN401 can protect against 5-FU toxicity in DPD deficient patients, suggesting that PN401 may be very helpful in patients at risk of toxicity following the administration of standard doses of 5-FU [14]. The demonstration in the Ashour study that toxicity reduction is still observed when PN401 is given 48 h after a lethal dose of 5-FU [18] suggests that PN401 can be used as an antidote after accidental overdose of 5-FU (e.g. due to pump malfunction or ingestion of excessive quantities of 5-FU prodrugs like capecitabine). Whether PN401 would be effective in protecting against 5-FU induced toxicity in patients with the autosomal co-dominantly inherited DPD deficiency (detected in 3–5% of the general population, still needs to be investigated.
Conclusion
In conclusion, DPD deficiency is a relatively common, enzyme disorder to be aware of when considering 5-FU chemotherapy administration. Findings to look for include mucositis, granulocytopenia, and neuropathy. If undiagnosed, DPD deficiency can lead to death. Treatment consists of stopping 5-FU and is otherwise largely supportive. The knowledge of this true pharmacogenetic syndrome is important as 5-FU remains the third most commonly used chemotherapy worldwide. To date, screening of patients for the presence of a DPD deficiency prior to the treatment with 5-FU is not yet routinely performed. We suggest that patients should be informed about the risks of the therapy and DPD testing should be performed upon manifestations of severe untoward toxicity.
References
Allegra CJ, Grem JL (1997) Antimetabolites. In: DeVita VT Jr, Hellman S, Rosenberg SA (eds) Cancer: principles and practice of oncology, 5th edn. Lippincott-Raven, Philadelphia, pp 432–451
Sobrero AF, Aschele C, Bertino JR (1997) Fluorouracil in colorectal cancer: a tale of two drugs—implications for biochemical modulation. J Clin Oncol 15:368–381
Grem JL (1996) 5-Fluoropyrimidines In: Chabner BA, Longo DL (eds) Cancer chemotherapy and biotherapy: principles and practice. Lippincott-Raven, Philadelphia, pp 149–211
Ezzeldin H, Diasio R (2004) Dihydropyrimidine dehydrogenase deficiency, a pharmacogenetic syndrome associated with potentially life-threatening toxicity following 5-fluorouracil administration. Clin Colorectal Cancer 4:181–189
Johnson MR, Diasio R (2001) Importance of dihydropyrimidine dehydrogenase (DPD) deficiency in patients exhibiting toxicity following treatment with 5-fluorouracil. Adv Enzyme Regul 41:151–157
Van Kuilenburg AB, Haasjes J, Richel DJ, Zoetekouw L, Van Lenthe H, DeAbreu RA, Maring JG, Vreken P, Van Gennip AH (2000) Clinical implications of dihydropyrimidine dehydrogenase (DPD) deficiency in patients with severe 5-fluorouracil-associated toxicity; identification of new mutations in the DPD gene. Clin Cancer Res 12:4705–4012
Saif MW, Mattison L, Carollo T, Ezzeldin H, Diasio RB (2006) Dihydropyrimidine dehydrogenase deficiency in an Indian population. Cancer Chemother Pharmacol 58(3):396–401
Saif MW, Diasio R (2006) Is capecitabine safe in patients with gastrointestinal cancer and dihydropyrimidine dehydrogenase deficiency? Clin Colorectal Cancer 5(5):359–362
Ezzeldin H, Okamoto Y, Johnson MR, Diasio RB (2002) A high-throughput denaturing high-performance liquid chromatography method for the identification of variant alleles associated with dihydropyrimidine dehydrogenase deficiency. Anal Biochem 306:63–73
Ezzeldin H, Johnson MR, Okamoto Y, Diasio RB (2003) Denaturing high performance liquid chromatography (DHPLC) analysis of the DPYD gene in patients with lethal 5-fluorouracil (5-FU) toxicity. Clin Cancer Res 9:3021–3028
Raida M et al (2001) Prevalence of a common point mutation in the dihydropyrimidine dehydrogenase (DPD) gene within the 5′-splice donor site of intron 14 in patients with severe 5-fluorouracil (5-FU)-related toxicity compared with controls. Clin Cancer Res 7(9): 2832–2839
Johnson MR, Yan J, Shao L, Albin N, Diasio RB (1997) Semi-automated radioassay for determination of dihydropyrimidine dehydrogenase (DPD) activity. Screening cancer patients for DPD deficiency, a condition associated with 5-fluorouracil toxicity. J Chromatogr B Biomed Sci Appl 696:183–191
Mattison LK, Ezzeldin H, Carpenter M, Modak A, Johnson MR, Diasio RB (2004) Rapid identification of dihydropyrimidine dehydrogenase deficiency by using a novel 2-13C-uracil breath test. Clin Cancer Res 10(8):2652–2658
Martin DS, Stolfi RL, Sawyer RC et al (1982) High-dose 5 fluorouracil with delayed “uridine” rescue in mice. Res 42:3964–3970
Saif MW, von Borstel R (2005) 5-Fluorouracil dose escalation enabled with PN401 (triacetyluridine): toxicity reduction and increased antitumor activity in mice. Cancer Chemother Pharmacol 27:1–7
Kelsen DP, Martin D, O’Neil J et al (1997) Phase I trial of PN401, an oral prodrug of uridine, to prevent toxicity from fluorouracil in patients with advanced cancer. J Clin Oncol 15:1511–1517
Hidalgo M, Villalona-Calero MA, Eckhardt SG, Drengler RL, Rodriguez G, Hammond LA, Diab SG, Weiss G, Garner AM, Campbell E, Davidson K, Louie A, O’Neil JD, von Borstel R, Von Hoff DD, Rowinsky EK (2000) Phase I and pharmacologic study of PN401 and fluorouracil in patients with advanced solid malignancies. J Clin Oncol 18(1):167–177
Ashour OM, Naguib FN, Panzica RP, Al Safarjalani ON, el Kouni MH (2000) Modulation of 5-fluorouracil host toxicity by 5-(benzyloxybenzyl)barbituric acid acyclonucleoside, a uridine phosphorylase inhibitor, and 2′,3′,5′-tri-O-acetyluridine, a prodrug of uridine. Biochem Pharmacol 60:427–431
Author information
Authors and Affiliations
Corresponding author
Additional information
This work was supported in part by NIH grant CA 62164.
Rights and permissions
About this article
Cite this article
Saif, M.W., Ezzeldin, H., Vance, K. et al. DPYD*2A mutation: the most common mutation associated with DPD deficiency. Cancer Chemother Pharmacol 60, 503–507 (2007). https://doi.org/10.1007/s00280-006-0392-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-006-0392-5