
Abstract
Purpose
To evaluate the usefulness and pharmacokinetics of docetaxel in the treatment of elderly patients with advanced non-small-cell lung cancer.
Patients and methods
Chemotherapy-naive elderly patients (aged at least 76 years) with locally advanced or metastatic non-small-cell lung cancer were accrued. Eligible patients received at least two cycles of docetaxel at a dose of 60 mg/m2 on day 1 over 1 h every 3 weeks. Patients who were considered ineligible for this study were also registered. Symptom control was assessed using a questionnaire during the treatment period. The pharmacokinetics of docetaxel were evaluated in the first cycle of chemotherapy.
Results
Of 35 elderly patients, 15 (43%) met the study eligibility criteria. The reasons for ineligibility consisted mainly of poor performance status, poor bone marrow function, and hypoxemia (six patients each). A total of 49 cycles of chemotherapy (median 2 cycles, range 1–12 cycles) were administered to the eligible patients, six of whom achieved a partial response (overall response rate 40%, 95% confidence interval 15–65%). The major toxicity was hematologic, with grade 3 or greater neutropenia and grade 3 neutropenic fever developing in 13 patients (87%) and five patients (33%), respectively. Symptoms, as assessed in terms of the symptom control score, did not clearly decline during the treatment period. The values (mean±SD) of Cmax, AUC0→inf, and t1/2 were 1.35±0.32 μg/ml, 1.79±0.52 μg h/ml, and 4.1±2.3 h, respectively.
Conclusions
Although the validity of the results of this study is limited due to the small sample size, docetaxel appears effective in selected elderly patients with advanced non-small-cell lung cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence and mortality rate of lung cancer are increasing in Western countries and Japan. In the United States, the incidences of lung cancer per 100,000 persons from 1994 through 1997 were 565.5 for men and 294.1 for women, and peaked between the ages of 75 and 79 years [18]. In Osaka prefecture, Japan, the incidence also peaked above 74 years of age in the same period [18]. In addition, the mortality rates of lung cancer patients older than 74 years were 42.2% for men and 53.4% for women in Japan in 1999 [14]. Accordingly, treatment of elderly patients with lung cancer is of particular concern.
Cisplatin-based chemotherapy has been proven to improve survival of patients with advanced non-small-cell lung cancer (NSCLC) compared to best supportive care [11]. However, this benefit is modest and is limited to patients who have favorable conditions such as good performance status (PS) and younger age. In clinical trial, the upper age limit is usually set at 65 or 70 years, or 75 years at most; therefore, patients older than 75 years have been excluded from clinical trials. The diversity of the elderly population makes it particularly difficult to determine the appropriateness of chemotherapy. The prevalence of comorbidity, functional limitations, socioeconomic restrictions, and geriatric syndromes appears to increase in patients greater than 74 years of age. Although no precise formulae are available for determining the physiologic age of patients, Balducci and Extermann have noted that an age of 75 years might represent a reasonable cut-off point to define older individuals [1]. In addition, it remains unclear how many patients can be treated with chemotherapy among all elderly patients with NSCLC, since there have been few reports on the proportion of patients eligible for chemotherapy among all elderly individuals with advanced NSCLC.
New anticancer agents such as vinorelbine, gemcitabine, and taxanes were developed and introduced for the treatment of NSCLC in the 1990s [2]. Among these agents, docetaxel is the first agent to be approved in Japan. The approved dose (60 mg/m2) in Japan is lower than that (100 mg/m2) in the United States and European countries [4]. However, this low dose of docetaxel is sufficiently effective with a low incidence of toxicities such as hypersensitivity and peripheral edema [4, 9].
On the basis of these considerations, a phase II study of docetaxel in elderly patients with advanced NSCLC was conducted in order to (1) evaluate the proportion of patients eligible for this study among all elderly patients with advanced NSCLC, (2) assess the efficacy and safety of docetaxel in the treatment of selected elderly patients, (3) examine the tolerability of this treatment from the view point of symptom control assessment during the treatment period, and (4) examine the pharmacokinetic profile of docetaxel in the elderly.
Patients and methods
Eligibility criteria
Chemotherapy-naive elderly patients (aged at least 76 years) with histologically or cytologically confirmed locally advanced (stage IIIA with N2 or IIIB) or metastatic (stage IV) NSCLC were accrued to this study. Eligibility criteria included an Eastern Cooperative Oncology Group PS of two or less, at least one measurable or assessable lesion, and life expectancy of 3 months or longer. Before enrollment, a complete medical history was obtained from each patient, and each underwent physical, laboratory, and staging work-up examinations. Laboratory examinations included complete blood cell counts with differential, routine serum chemistry and tumor marker analyses, 24-h creatinine clearance evaluation, arterial blood gas analysis, urinalysis, electrocardiogram, and pulmonary function tests. Staging work-up examination consisted of chest radiograph, computerized tomography (CT) of the chest and abdomen, magnetic resonance imaging of the brain, radionucleotide bone scan, and fiberoptic bronchoscopy. On laboratory examination, patients were required to have adequate organ function, as evidenced by a leukocyte count between 4000 and 12,000/μl, a neutrophil count of 2000/μl, a hemoglobin level of 9.5 g/dl, a platelet count of 100,000/μl, a total bilirubin level of 1.5 mg/dl, AST and ALT levels 2.5 times the upper limit of the normal range, a serum creatinine level not more than the upper limit of the normal range, and a PaO2 of 65 mmHg. Patients with active infection, interstitial pneumonia, peripheral edema, or pleural or pericardial effusion that required drainage (patients with pleural effusion who had been successfully treated with agents other than anticancer drugs were eligible), a history of severe hypersensitivity, symptomatic brain metastasis, or active concomitant malignancy were excluded. Patients who were for other reasons considered not suited for study entry by the treating physician were also excluded. In addition, concomitant use of ketoconazole, miconazole, erythromycin, or clarithromycin was not permitted in this study, because it is possible that docetaxel metabolism is inhibited by these agents via liver cytochrome P450 isozyme CYP3A [7].
Written informed consent was obtained from all patients. Three institutions participated in this study, and each of their Institutional Review Boards approved this study. The registration office (National Shikoku Cancer Center) entered the patients after verification of eligibility. Patients who were considered ineligible for this study were also registered in order to assess the reasons for ineligibility and estimate the proportion of eligible patients among the entire elderly population with advanced NSCLC.
Chemotherapy
Eligible patients received at least two cycles of docetaxel monotherapy. Docetaxel was given at a dose of 60 mg/m2 on day 1 and repeated every 3 weeks. It was diluted in 500 ml 5% glucose or 0.9% saline solution, and was infused over a 1-h period. Antiemetic treatment was left to the treating physician. Prophylactic administration of dexamethasone was used to prevent fluid retention or hypersensitivity reaction, as well as for the prevention of emesis. Administration of granulocyte-colony stimulating factor (G-CSF) was allowed when grade 4 neutropenia or grade 3 neutropenic fever occurred. This administration was continued until the neutrophil count recovered to 5000/μl. The dose of docetaxel was reduced to 50 mg/m2 in the presence of grade 4 hematologic toxicities lasting 3 days or when grade 3 non-hematologic toxicities had developed in the prior cycle of chemotherapy. Chemotherapy was withdrawn when similar toxicities were observed at this reduced dose level. In addition, docetaxel administration was postponed for up to 2 weeks (a maximum 6 weeks between administrations) when leukocyte, neutrophil, and platelet counts were less than 4000, 2000, and 100,000/μl, respectively. Chemotherapy was discontinued when delay of hematologic recovery continued for over 2 weeks. Other criteria for early interruption of this protocol treatment included progression of disease, emergence of intolerable toxicities, and withdrawal of consent. In addition, chemotherapy was discontinued for patients who were assessed as having stable disease after completion of two cycles of chemotherapy. Responders were allowed to continue this treatment until disease progression or the emergence of intolerable toxicities.
Toxicity and response evaluation
For evaluation of response and toxicity, all patients underwent as inpatients a series of examinations consisting of complete blood cell counts with differential, routine chemistry profiles, and chest radiograph on at least a weekly basis during the treatment period and then on a monthly basis. In addition, the patients’ clinical characteristics such as symptoms, body temperature, and weight were periodically recorded. Evaluation of target lesions was performed after each cycle of chemotherapy, and the same examinations as for the staging work-up study were performed after completion of treatment.
Responses were assessed using the World Health Organization criteria [8]. The response to treatment, including eligibility and assessability, was determined for each patient by extramural reviewers. Complete response was defined as the disappearance of all measurable lesions for at least 4 weeks. Partial response (PR) was defined as a 50% decrease in the sum of the products of the greatest perpendicular diameters of all measurable lesions for at least 4 weeks without the development of new lesions. Progressive disease (PD) was defined as a 25% increase in the sum of the products of the perpendicular diameters of all measurable disease or the appearance of new lesions. If no response or progression of disease occurred during therapy, treatment outcome was considered to be no change (NC). Toxicities were assessed and graded using the National Cancer Institute Common Toxicity Criteria, version 2.0 (the Japan Clinical Oncology Group version) [10]. The worst degree of toxicity experienced throughout the treatment was computed for each patient.
Symptom control assessment
A quality-of-life (QOL) questionnaire for cancer patients treated with anticancer drugs (QOL-ACD) has been developed in Japan [5]. It is a 22-item questionnaire that covers four domains consisting of functional, physical, mental, and psychosocial well-being. In addition, global QOL is assessed using a face scale. In this study, assessment of symptoms during chemotherapy was performed using a questionnaire that consisted of four items selected from the QOL-ACD questionnaire (feeling, appetite, vomiting, and sleep) and an additional item concerning respiratory condition (cough and sputum). Assessment of global QOL using the face scale was also performed. Each patient was asked to fill in this questionnaire at the time of study entry (baseline symptom score) and immediately before each cycle of chemotherapy. Severity of each symptom during chemotherapy was scored using a visual analogue scale and was assessed compared with the baseline value.
Pharmacokinetic evaluation
The pharmacokinetics of docetaxel were studied in the first cycle of chemotherapy. Samples were taken at the following time points: predose, midinfusion, end of infusion, and 30 min and 2, 3, 5, 7, 23, 47 and 71 h after infusion. All blood samples were immediately centrifuged and the heparinized plasma was stored at −20°C until analysis. Subsequent assays and pharmacokinetic analysis were performed based on a previously described method [13]. Briefly, docetaxel concentrations in plasma were determined by high-performance liquid chromatography with UV detection. Docetaxel and internal standard were determined by a UV detector adjusted to 225 nm, and peak heights were used for quantification. Pharmacokinetic parameters were calculated using WinNonlin computer software (Pharsight, Mountain View, Calif.). The maximum plasma concentration (Cmax) was obtained from the actual value. The terminal rate constant (k) was determined by log-linear regression analysis of the terminal phase of the plasma concentration vs time curve. The terminal half-life time (t1/2) was calculated by the equation t1/2=0.693/k. The area under the concentration vs time curve (AUC) was calculated by the linear trapezoidal rule up to the last measurable data points with extrapolation to infinity. The clearance (CL) was calculated by dividing the dose received by the AUC.
Statistical considerations
The sample size of this study was determined with the assumption of an expected response rate of 20%, with a 95% confidence interval (CI) of ±10%. Accrual of 61 patients was therefore required for this study. Statistical analyses were performed using the SPSS Base System and Advanced Statistics programs (SPSS, Chicago, Ill.). The significances of differences between baseline and during-treatment or post-treatment symptom scores were determined using Student’s paired t-test. The global QOL score was similarly analyzed. Survival time was defined as the period from initiation of treatment to death or last follow-up evaluation. In addition, time to progression was defined as the period from initiation of treatment to PD. Patients who received additional thoracic radiotherapy were censored at the start of irradiation. Survival curves were calculated using the method of Kaplan and Meier.
Results
Patient characteristics
Between November 1999 and December 2001, 35 elderly patients with advanced NSCLC were accrued to this study. Of these, 15 (43%) met the study eligibility criteria. Although the sample size of this study was designed to be 61 patients on an eligible patient basis, the study was terminated early due mainly to the slow rate of accrual of patients.
The characteristics of the entire group of patients and eligible patients are listed in Table 1. The median ages and age ranges were similar for the two groups. However, the proportions of patients with a poor PS, adenocarcinoma, or metastatic disease were higher in the entire group than in the eligible group. The proportion of patients with weight loss was not determined in the entire group, since assessment of weight loss was not required for registration of patients ineligible for this study. The reasons for ineligibility for study entry were poor PS (n=6), poor bone marrow function (n=6), hypoxemia (n=6), life expectancy less than 3 months (n=4), physician’s discretion (n=4), symptomatic brain metastasis (n=2), double cancer (n=2), poor renal function (n=1), infection (n=1), and interstitial lung disease (n=1). More than one reason was noted in seven patients. In addition, two patients refused chemotherapy. Among ineligible patients, two received chemotherapy; one with anemia received docetaxel at a dose of 60 mg/m2, and the other with anemia and hypoxemia received vinorelbine monotherapy. The serum albumin values (means±SD) were 3.6±0.30 g/dl in 15 eligible patients and 3.9±0.39 g/dl in 20 ineligible patients. In addition, the value of plasma alpha-1 acid glycoprotein (AAG), which was measured in ten eligible patients, was 1.22±0.39 g/l.
Chemotherapy outcome
A total of 49 cycles of chemotherapy were administered to 15 eligible patients. The median number of chemotherapy cycles was two (1 cycle in two patients, 2 cycles in six, 3 cycles in four, 5 cycles in one, 6 cycles in one, and 12 cycles in one). Two patients who had disease progression or developed docetaxel-related interstitial lung toxicity received only one cycle of chemotherapy. Four patients underwent reduction of dose of docetaxel because of grade 4 neutropenia lasting for 3 days (n=3), grade 3 neutropenic fever (n=1), or grade 3 nausea (n=1). One patient developed both grade 4 neutropenia and grade 3 nausea. In addition, the median interval between each cycle of chemotherapy was 22 days (range 19–30 days).
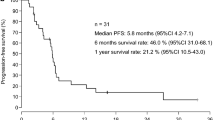
Of the 15 patients, 6 achieved PR, 6 NC, and 2 PD. Response was not evaluated for one patient who developed docetaxel-related interstitial pneumonia. The overall response rate was 40%, with a 95% CI of 15–65%. Four patients with stage IIIA (n=3) or IIIB disease (n=1) received additional thoracic radiotherapy. The plasma AAG levels of two patients with PD were 1.85 and 1.79 g/l, respectively, which were the highest and the second highest values in this study. With a median follow-up period of 27.9 months (range 16.2–42.5 months), median progression-free survival time was 6.1 months (95% CI 5.6–6.6 months). At the time of analysis, 11 patients had died and four were still alive. The cause of death was directly related to NSCLC in ten patients and unrelated in one (interstitial pneumonia). This complication of interstitial pneumonia, occurring in another patient who developed docetaxel-related lung toxicity, was observed more than 12 months after completion of chemotherapy. The median survival time was 15.6 months (95% CI 11.4–19.8 months), with 1-year and 2-year survival rates of 73.3% and 37.3%, respectively.
The toxicities observed in the 15 patients during treatment and the follow-up period are listed in Table 2. The major toxicity was myelosuppression, with grade 3 or higher leukopenia and neutropenia observed in 9 patients (60%) and 13 patients (87%), respectively. Grade 3 neutropenic fever occurred in five patients (33%). G-CSF was administered to 13 patients (87%) over a median duration of 4 days (range 2–6 days). Grade 3 nonhematologic toxicities observed in this study included fatigue (33%), dyspnea (13%), electrolyte disturbance (13%), nausea (13%), and vomiting (7%). Grade 3 dyspnea observed in two patients was associated with bacterial pneumonia and docetaxel-related interstitial lung toxicity. No patients experienced hypersensitivity reactions or peripheral edema. Overall, grade 3 or higher hematologic and nonhematologic toxicities were observed in 14 patients (93%) and 8 patients (53%), respectively. No treatment-related death occurred.
Changes in symptom scores during chemotherapy
A total of 39 questionnaires were collected throughout the study. The overall collection rate was 61% (39/64), with rates after the first, second, and third cycle of chemotherapy of 87% (13/15), 38% (5/13), and 43% (3/7), respectively. Changes in symptom and global QOL (face scale) scores up to the third assessment are shown in Fig. 1, where individual scores are presented as relative values as compared with the baseline value. At each assessment, patients exhibited improvement in feeling, appetite, and global QOL; whereas slight deterioration was found in vomiting, cough and sputum. However, there were no significant differences in the changes in these scores during the treatment period. In addition, no relationship was found between relative symptom score and response to treatment.

Changes in relative symptom scores during the treatment period. The histograms represent mean and standard deviation
Pharmacokinetic results
Blood sampling for pharmacokinetic analysis was not performed in three patients because of patient refusal. The Cmax (1.35±0.32 μg/ml, mean±SD), AUC0→inf (1.79±0.52 μg h/ml), and t1/2 (4.1±2.3 h) in the 12 elderly patients were somewhat lower than those (Cmax, 1.61±0.59 μg/ml; AUC0→inf, 2.44±0.83 μg·h/ml; t1/2, 7.5±6.3 h; n=6) in non-elderly patients in a phase I study in Japan (docetaxel dose 60 mg/m2; infusion time 60–160 min) [15]. Conversely, the CL (38.5±8.5 l/h/m2) in this study was somewhat higher than that (27.8±11.6 l/h/m2) in the phase I study. The non-elderly pharmacokinetic participants were required to have an Eastern Cooperative Oncology Group PS of two or less, to be aged between 15 and 75 years old, and to have a leukocyte count ≥4000/μl, a neutrophil count ≥1500/μl, a hemoglobin level ≥9.5 g/dl, a total bilirubin level ≤1.5 mg/dl, AST and ALT levels not more than two times the upper limit of the normal range, and a serum creatinine level not more than the upper limit of the normal range [15].
Discussion
This is, to our knowledge, the first study of an every 3-weeks schedule of docetaxel in chemotherapy-naive elderly patients with advanced NSCLC. The percentage of patients who are reluctant to receive chemotherapy or who should not be treated with chemotherapy due to poor PS or comorbidity appears to be much higher among elderly patients than among younger patients [3]. In this study, we attempted to estimate the proportion of patients eligible for docetaxel among all elderly patients with advanced NSCLC who visited our hospitals. In a previous study by Oshita et al., 10 of 34 elderly (aged at least 75 years) patients (29%) with lung cancer were eligible for cisplatin-based chemotherapy [12]. In addition, in our retrospective series, 37% of elderly patients with advanced NSCLC underwent either cisplatin-based or non-platinum combination chemotherapy [16]. The results of these studies as well as that (proportion of eligible patients, 43%) of our own suggest that chemotherapy can be administered to approximately 30–40% of elderly patients with advanced NSCLC. However, these findings should be cautiously interpreted because the figures might include a considerable degree of physician discretion with regard to chemotherapy drug and dosing in the elderly.
The initial estimated sample size was 61 patients, which was determined with the efficacy endpoint (one of four primary endpoints) of this study. However, this study was terminated early due to the slow rate of patient accrual. Although the sample size was extremely small, the response rate (40%, 95% CI 15–65%) can be considered at least comparable to that (19%, 95% CI 11–29%) in a phase II study of docetaxel, which was conducted for the application for approval of docetaxel in Japan [4]. In that study, advanced NSCLC patients with a median age of 67 years (range 40–80 years) received docetaxel at a dose of 60 mg/m2. In addition, the median survival time (15.6 months) in the present study is superior to that in the previous phase II study (9.8 months) [4], although four of nine patients with stage III disease underwent additional thoracic radiotherapy.
The major toxicity in our study was myelosuppression, with grade 3 or higher leukopenia and neutropenia, and grade 3 neutropenic fever observed in 60%, 87%, and 33% of patients, respectively. The incidence and severity of myelosuppression in our study were similar to those (49%, 87%, and 11%, respectively) in the Japanese phase II study [4]. However, hematologic toxicity was easily manageable, and did not lead to treatment-related death. Concerning non-hematologic toxicities, grade 3 or higher fatigue was more frequently observed in our study (20%) than in the phase II study (4%). However, there were no differences in the incidences of other non-hematologic toxicities between the two studies. In this study, relative symptom and global QOL scores did not decline during the treatment period. However, particularly after the second cycle of chemotherapy, only a small number of patients answered the questionnaire, adding limited information to this assessment.
It is believed that the pharmacokinetic profiles of docetaxel are not affected by patient age [6]. Compared with the result of a Japanese phase I study of docetaxel conducted in non-elderly patients [15], the values of Cmax, AUC0→inf, and t1/2 were slightly lower in our study, with a slight increase in CL. We cannot explain why docetaxel was cleared more rapidly in this study population. In addition, we have no clear explanation for the relationship between relatively increased total body clearance of docetaxel and high incidence of severe neutropenia. It seems difficult to compare the pharmacokinetic profiles of docetaxel between these studies, since docetaxel in the phase I study was infused at a dose of 60 mg/m2 over 60–160 min.
In conclusion, 43% of elderly patients with advanced NSCLC received single-agent docetaxel without a reduction in their symptoms in our study, although careful attention should be paid to the physiologic changes associated with ageing to ensure safe administration of anticancer drugs to the elderly. Based on the result of the “ELVIS” study, vinorelbine monotherapy has been considered the treatment of choice for elderly patients with advanced NSCLC [17]. Docetaxel monotherapy also appears to be useful for the treatment of elderly patients with advanced NSCLC, although the validity of the results is limited due to the small sample size. In future studies the endpoint should be limited and the age range should be reconsidered (e.g., 70 years or more). In addition, comorbidity, number of medications, and functional and cognitive status should be evaluated to ascertain the “physiologic age” of the elderly.
References
Balducci L, Extermann M (1997) Cancer chemotherapy in the older patient: what the medical oncologist needs to know. Cancer 80:1317–1322
Bunn PA, Kelly K (1998) New chemotherapeutic agents prolong survival and improve quality of life in non-small cell lung cancer: a review of the literature and future directions. Clin Cancer Res 4:1087–1100
Hutchins LF, Unger JM, Crowley JJ, Coltman CA Jr, Albain KS (1999) Under representation of patients 65 years of age or older in cancer-treatment trials. N Engl J Med 30:2061–2067
Kunitoh H, Watanabe K, Onoshi T, Furuse K, Niitani H, Taguchi T (1996) Phase II trial of docetaxel in previously untreated advanced non-small-cell lung cancer: a Japanese cooperative study. J Clin Oncol 14:1649–1655
Kurihara M, Shimizu H, Tsuboi K, Kobayashi K, Murakami M, Eguchi K, Shimozuma K (1999) Development of quality of life questionnaire in Japan: quality of life assessment of cancer patients receiving chemotherapy. Psychooncology 8:355–363
Lichtman SM, Villani G (2000) Chemotherapy in the elderly: pharmacologic considerations. Cancer Control 7:548–556
Marre F, Sanderink G, de Sousa G, Gaillard C, Martinet M, Rahmani R (1996) Hepatic biotransformation of docetaxel (Taxotere) in vitro: involvement of the CYP3A subfamily in humans. Cancer Res 56:1296–1302
Miller AB, Hoogstraten B, Staquet M, Winkler A (1981) Reporting results of cancer treatment. Cancer 47:207–214
Mukohara T, Takeda K, Miyazaki M, Takifuji N, Terakawa K, Negoro S (2001) Japanese experience with second-line chemotherapy with low-dose (60 mg/m2) docetaxel in patients with advanced non-small-cell lung cancer. Cancer Chemother Pharmacol 48:356–360
National Cancer Institute—Common Toxicity Criteria, version 2.0: the Japan Clinical Oncology Group version (1999) Gan To Kagaku Ryoho 26:1084–1144
Non-small Cell Lung Cancer Collaborative Group (1995) Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. BMJ 311:899–909
Oshita F, Kurata T, Kasai T, Fakuda M, Yamamoto N, Ohe Y, Tamura T, Eguchi K, Shinkai T, Saijo N (1995) Prospective evaluation of the feasibility of cisplatin-based chemotherapy for elderly lung cancer patients with normal organ functions. Jpn J Cancer Res 86:1198–1202
Segawa Y, Watanabe K, Hiraki S, Tominaga K, Hayashi I, Harada M, Yamakido M, Ueda N, Kashimura I, Niitani H (2000) Phase I study of docetaxel and cisplatin for patients with previously untreated metastatic non-small-cell lung cancer: a Japanese cooperative study. Int J Clin Oncol 5:308–315
Sobue T (2001) Lung cancer. Gan To Kagaku Ryoho 28:163–167
Taguchi T, Furue H, Niitani H, Ishitani K, Kanamaru R, Hasegawa K, Ariyoshi Y, Noda K, Furuse K, Fukuoka M (1994) Phase I clinical trial of RP56976 (docetaxel) a new anticancer drug. Gan To Kagaku Ryoho 21:1997–2005
Takigawa N, Segawa Y, Kishino D, Fujiwara K, Ida M, Eguchi K (2000) Combination chemotherapy consisting of ifosfamide and vindesine for non-small cell lung cancer in the elderly. Nippon Kokyuki Gakkai Zasshi 38:273–277
The Elderly Lung Cancer Vinorelbine Italian Study group (1999) Effects of vinorelbine on quality of life and survival of elderly patients with advanced non-small-cell lung cancer. J Natl Cancer Inst 91:66–72
Yoshimi I, Ohshima A, Ajiki W, Tsukuma H, Sobue T (2003) A comparison of trends in the incidence rate of lung cancer by histological type in the Osaka Cancer Registry, Japan and in the Surveillance, Epidemiology and End Results Program, USA. Jpn J Clin Oncol 33:98–104
Acknowledgement
This study was supported in part by a grant from the Ministry of Health, Labor and Welfare of Japan (no. 9-25).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Takigawa, N., Segawa, Y., Kishino, D. et al. Clinical and pharmacokinetic study of docetaxel in elderly non-small-cell lung cancer patients. Cancer Chemother Pharmacol 54, 230–236 (2004). https://doi.org/10.1007/s00280-004-0826-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-004-0826-x