
Abstract
The anti-CD20 antibody rituximab improves the results of first-line therapy in aggressive non-Hodgkin’s lymphoma (NHL) of B cell lineage. The purpose of this retrospective study was to evaluate its efficacy and toxicity in combination with the doxorubicine, methylprednisolone, high-dose cytarabine, cisplatin (ASHAP) protocol, an established treatment regimen for relapsed or refractory aggressive NHL. After a median of four cycles, 9 of 20 patients treated achieved a complete remission and 6 a partial remission, resulting in a total response rate of 75%. Remissions were not only seen in patients with relapsed lymphomas but also in patients with primary refractory or transformed indolent lymphomas. The outcome in cases with an international prognostic index score ≥2 was poor. Five of 15 responders received consolidating high-dose therapy with autologous stem cell transplantation. All of them are in ongoing remission. The main toxicity was myelosuppression, with neutropenias or thrombocytopenias of World Health Organization (WHO) grades III or IV developing in more than 90% of the cycles. There was one therapy-related death due to neutropenic sepsis. Non-hematologic toxicity was generally mild. At the time of analysis, six patients have died. After a median observation time of 17.5 months, the 2-year overall survival rate is 62%. ASHAP plus rituximab is an active and well-tolerated salvage protocol for patients with relapsed or refractory aggressive NHL, which compares favourably with other immuno-chemotherapy regimens, especially in patients with primary refractory or transformed indolent lymphomas.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Using modern treatment strategies, long-term remissions are achieved in a large fraction of patients with aggressive non-Hodgkin’s lymphomas (NHL). However, there is a significant proportion of patients (30–50%) who either fail to attain complete remission or suffer relapse of their disease. High-dose chemotherapy with stem cell transplantation has become the standard treatment for relapsed or refractory aggressive NHL, but no salvage therapy is accepted as the standard regimen before transplantation [1–4].
The doxorubicine, methylprednisolone, high-dose cytarabine, cisplatin (ASHAP) regimen, which consists of doxorubicin (=adriamycine, ‘A’), methylprednisolone (=solumedrol, ‘S’), high-dose cytarabine (‘Ara-C’, ‘HA’), and cisplatin (‘P’), is an effective dose-intensive regimen with mild extramedullary toxicity capable of mobilizing peripheral blood progenitor cells. Recently, we reported the treatment results of this regimen, which compared favourably with those of other established protocols for relapsed or refractory aggressive NHL [5]. The overall response rate of ASHAP in patients with relapsed or refractory aggressive NHL is approximately 70%, with a complete remission rate of 40–50%. However, similar to other salvage regimens, the ASHAP protocol appears inadequate for the treatment of most patients with primary refractory or transformed indolent lymphomas [5–8].
The addition of rituximab, a chimeric anti-CD20 monoclonal antibody, to the cyclophosphamid–doxorubicin–vincristine–prednisone (CHOP) regimen significantly improved the remission rate and survival in patients with untreated aggressive B cell lymphoma [9]. In patients with aggressive lymphoma relapsing after or refractory to chemotherapy, single-agent rituximab yielded an objective response rate of 30–35% [10–12].
The objective of this retrospective study was to investigate the effectiveness of rituximab in conjunction with the ASHAP protocol (R-ASHAP) in patients with relapsed or refractory aggressive B cell NHL.
Materials and methods
Between June 2002 and December 2004, 20 patients with relapsed or refractory aggressive NHL were treated with a recently reported variant of the ASHAP regimen consisting of doxorubicin (10mg/m2/day), cisplatin (25mg/m2/day, both by continuous intravenous [IV] infusion via a central venous catheter, days 1 to 4), cytarabine (2 g/m2 IV over 2 h after completion of doxorubicin and cisplatin, day 5), and methylprednisolone (500 mg/day IV over 15 min, days 1 to 5) [5, 6]. Rituximab (375 mg/m2) was infused according to standard prescribing guidelines on day 1 of each cycle after administration of oral paracetamol and i.v. diphenhydramine.
Therapy was repeated on day 21, provided that the leukocyte and platelet counts had recovered to more than 3.0/nl and 100/nl, respectively.
Response was evaluated after two to three cycles of therapy. Complete response was defined as complete disappearance of all measurable or evaluable disease, as assessed by physical examination and radiographic studies. Partial response was defined as ≥50% but <100% improvement. In patients with complete or partial remission, subsequent therapy was scheduled according to the patient’s age and risk profile as defined by the International Prognostic Index (IPI). In patients with stable or progressive disease, alternative types of treatment were initiated.
Overall survival and progression-free survival were measured from the time of diagnosis of relapse until death or disease progression. Survival curves were generated using the method of Kaplan and Meier and compared using the log-rank test. The effect of pre-treatment variables on therapy response was assessed using Fisher’s exact test and the Mann–Whitney U test. The results were analysed using SPSS for Windows® 11.0 (SPSS, Chicago, IL, USA).
Results
Patient characteristics and treatment details
Twenty patients, ten men and ten women, with a median age of 63 years (range 39–72) were treated with a median of four cycles (range 1–6) of the R-ASHAP regimen. Four patients had primary refractory disease, 13 had first, and three had second relapse after achieving complete remission.
All patients were intensively pre-treated. Thirteen patients had received one, four patients two and three patients more than two lines of chemotherapy. All patients had received anthracyclines, and three had been pre-treated with rituximab (Table 1).
Four to eight cycles of the CHOP regimen were performed in a total of 14 patients, whereas six to eight cycles of the CHOEP regimen were administered in five patients. Only in one patient the total dose of doxorubicin had to be reduced. This patient suffered from an initial mediastinal diffuse large B cell lymphoma and had undergone eight cycles of the CHOEP regimen with consecutive mediastinal radiation. Because of present reduction in the ejection fraction to 45%, we cancelled doxorubicin in the last three cycles of R-ASHAP from a total of six cycles. In all other cases, doxorubicin-related cardiac toxicity was not observed.
Eleven patients presented with Ann Arbor stage III or IV, six with an elevated lactate dehydrogenase activity, and seven with an IPI score ≥2 (Table 2).
All in all, 83 cycles of R-ASHAP were administered. One patient received only 1 cycle because of death due to lymphoma progression. Of the remaining 19 patients, 1 completed two cycles, 3 completed three cycles, 9 completed four cycles, 1 completed five cycles, and 5 completed six cycles. The doses of doxorubicin, cisplatin, or cytarabine had to be reduced in a total of 21 cycles because of prolonged neutropenia or elevated liver enzymes during the preceding cycle.
Three patients received granulocyte colony stimulating factor (G-CSF) to shorten the period of neutropenia, and in seven, G-CSF was used for stem cell mobilization.
Response to R-ASHAP and long-term outcome
Nine patients (45%) achieved a complete remission and six (30%) a partial remission. Two patients had stable disease, and three progressed. Of the four patients with primary refractory lymphoma, two achieved a partial response, and two had stable disease. Of the eight patients with transformed indolent lymphoma, two demonstrated a complete response (25%), five a partial response (62.5%), and one developed a progressive disease (12.5%).
Of the three patients who had received rituximab during their previous therapies, one achieved a partial remission, one showed stable disease, and one progressed after treatment with R-ASHAP.
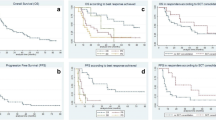
After a median follow-up of 17.5 months, the median survival and progression-free survival times have not been reached (Figs. 1 and 2). The actuarial 2-year overall survival and progression-free survival is 62% and 63%, respectively. Thirteen patients (65%) are in ongoing remission. Six patients (30%) have died, four of progression of lymphoma (two with primary refractory disease and two with transformed indolent lymphoma), one of therapy-related neutropenic sepsis, and one of a bleeding stomach ulcer unrelated to lymphoma or therapy.

Progression-free survival of 20 patients treated with R-ASHAP in comparison to 24 patients receiving ASHAP without rituximab

Overall survival of 20 patients treated with R-ASHAP in comparison to 24 patients receiving ASHAP without rituximab
Subsequent therapy
In the 15 responding patients, therapy after completion of the R-ASHAP protocol varied according to pre-treatment, disease stage at relapse, age, comorbidity, and availability of autologous or allogeneic blood stem cells.
One patient below the age of 60 with a low risk profile (IPI score of 0), and three patients above the age of 60 (all with an IPI score ≥1) received involved-field radiotherapy for consolidation of remission. One patient with an acoustic neurinoma requiring urgent surgery received two cycles of the DexaBEAM protocol after remission induction by R-ASHAP.
Peripheral blood stem cell mobilization was successful in five of seven patients treated with G-CSF after the second cycle of R-ASHAP. In these patients, complete or partial remissions were consolidated with high-dose chemotherapy according to the BEAM regimen followed by stem cell transplantation. After a median observation time of 18 months, all five patients are in ongoing remission.
In three patients, autologous transplantation was not envisaged because they had already undergone this procedure before. One of these patients achieved a partial remission, which was consolidated by allogeneic transplantation. The others achieved complete remissions, which were left unconsolidated.
Two patients received no further treatment after remission induction by R-ASHAP because of failure to harvest adequate numbers of blood stem cells or patient’s choice, respectively.
Prognostic factors
The prognostic value of the parameters listed in Tables 1 and 2 was analysed using the Kaplan–Meier method. An IPI score ≥2 was correlated with poor overall survival (p = 0.049). By contrast, elevated lactate dehydrogenase activities or refractoriness to first-line therapy were not correlated with poor survival (p = 0.35 and p = 0.25, respectively). Patients with transformed indolent lymphomas fared equally well as patients with de novo aggressive lymphomas (p = 0.62). Other parameters like age, extranodal manifestations or prior radiotherapy showed no impact on the effectiveness of R-ASHAP.
Toxicity
The major toxicity was myelosuppression (Table 3). Grade III or IV neutropenia was observed in 18 patients (90%). Six of them (30%) developed infections that required hospitalization (4 patients) or were life-threatening (2 patients). One patient died of therapy-related neutropenic sepsis and pneumonia. Except for one, all patients received red blood cell or platelet transfusions for grade III or IV anemia (40 and 10%, respectively) or thrombocytopenia (50 and 45%, respectively).
Non-hematological side effects like nausea, diarrhea, and nephrotoxicity, all grade III, or elevation of liver enzymes were observed in one patient each (5%).
One patient with leukemic mantle cell lymphoma developed an allergic reaction to rituximab (5%) with hypotonia, throat discomfort, and headache, despite prophylactic medication of paracetamol, diphenhydramine, and methylprednisolone, which resolved within hours after further addition of antihistamines and steroids.
Comparison of the R-ASHAP regimen with the historical ASHAP regimen
Table 4 compares the treatment results of the R-ASHAP protocol and the original ASHAP regimen without rituximab reported by us previously [5]. Although statistically significant differences were not observed in any of the parameters listed, a trend was observed towards an improved outcome in patients with primary refractory or transformed indolent lymphomas when rituximab was added to the treatment schedule. Also, the proportion of patients surviving without disease progression for 2 years tended to be higher in the R-ASHAP as compared to the ASHAP group.
Discussion
The value of multi-agent chemotherapy in the treatment of patients with aggressive NHL who have relapsed after an anthracycline-containing induction regimen is well established [4, 12]. However, the treatment remains problematic, with the majority of patients showing incomplete or only temporary response. The monoclonal antibody rituximab alone induces responses in approximately 30–35% of patients with relapsed or primary refractory aggressive B cell lymphomas [10–12].
The response rate in our group of patients was comparable to that of other rituximab-containing salvage chemotherapy regimens for patients with relapsed or refractory aggressive lymphomas, such as immuno-chemotherapy with the rituximab plus ifosfamide, carboplatin, etoposide (R-ICE), rituximab plus dexamethasone, high-dose cytarabine, cisplatin (R-DHAP), or rituximab plus etoposide, methylprednisolone, high-dose cytarabine, cisplatin (R-ESHAP) regimen with overall response rates between 54 and 93% (Table 5). No significant differences were observed between the treatment results reported previously of the original ASHAP protocol (without rituximab) and the R-ASHAP regimen presented here. The selection of patients, however, was not identical in these studies. In comparison to our previous series, the present cohort of patients displayed more adverse characteristics, with a higher proportion of patients with transformed indolent lymphoma (40% vs 25%), a lower proportion of stage I patients (5% vs 21%), and a higher proportion of patients relapsing after high-dose therapy with autologous transplantation (15% vs 0%). In spite of these adverse features, the group of patients treated with ASHAP plus rituximab demonstrated a trend towards a higher response rate and a prolonged progression-free survival. This was particularly noticeable in patients who are characterized by a particularly poor prognosis, with primary refractory or transformed indolent lymphomas (overall response 50 or 88% for R-ASHAP vs 25 or 33% for ASHAP). It appears possible that these differences would become more convincing with a larger number of patients studied in each group.
The major toxicity observed in our study was myelosuppression. About 90% of the patients developed grade III or IV neutropenia or thrombocytopenia after treatment with R-ASHAP. One therapy-related death was observed due to neutropenic sepsis. This patient suffered from leukemic mantle cell lymphoma and had been treated with four different lines of therapy before receiving R-ASHAP. He was also the only one to show a grade IV allergic reaction to the infusion of rituximab. Comparing the toxicity of R-ASHAP with that of ASHAP alone [5], more infections and more impairment of renal function were observed among the patients receiving rituximab. ASHAP alone caused grade II–IV infections in 33% of the patients, whereas, with the R-ASHAP protocol, such infections were seen in 60% (30% WHO grade II and 30% WHO grade III or IV). A deterioration of renal function occurred in 40% of patients receiving R-ASHAP as compared to 4% in patients treated with ASHAP. Nephrotoxicity, however, may have been unrelated to rituximab because the median number of chemotherapy cycles administered was considerably higher in patients treated with R-ASHAP as compared to patients treated with ASHAP (4, 0 vs 2, 8 cycles). Therefore, the group of patients receiving R-ASHAP had a higher exposure to the nephrotoxic agent cisplatin than the group treated with ASHAP alone.
In summary, ASHAP plus rituximab is a well-tolerated regimen in extensively pre-treated patients with relapsed or refractory NHLs. The protocol led to complete or partial remissions in 75% of all patients. Side effects were similar to those seen with the ASHAP protocol alone, although addition of rituximab may confer an increased risk of infections. Particularly promising results were obtained in patients who are generally characterized by a dire prognosis, with primary refractory or transformed indolent lymphomas.
However, the role of rituximab in salvage therapy regimens must be determined in future studies, as rituximab in combination with chemotherapy will be administered in first-line therapy.
References
Philip T, Guglielmi C, Hagenbeek A et al (1995) Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin’s lymphoma. N Engl J Med 333:1540–1545
Philip T, Armitage JO, Spitzer G et al (1987) High-dose therapy and autologous bone marrow transplantation after failure of conventional chemotherapy in adults with intermediate-grade or high-grade non-Hodgkin’s lymphoma. N Engl J Med 316:1493–1498
Press OW, Livingston R, Mortimer J, Collins C, Appelbaum F (1991) Treatment of relapsed non-Hodgkin’s lymphomas with dexamethasone, high-dose cytarabine, and cisplatin before marrow transplantation. J Clin Oncol 9:423–431
Velasquez WS, Cabanillas F, Salvador P et al (1988) Effective salvage therapy for lymphoma with cisplatin in combination with high-dose Ara-C and dexamethasone (DHAP). Blood 71:117–122
Nückel H, Dürig J, Dührsen U (2003) Salvage chemotherapy according to the ASHAP protocol: a single-center study of 24 patients with relapsed or refractory aggressive non-Hodgkin’s lymphomas. Ann Hematol 82:481–486
Hänel M, Kröger N, Hoffknecht MM et al (2000) ASHAP—an effective salvage therapy for recurrent and refractory malignant lymphomas. Ann Hematol 79:304–311
Velasquez W, Dunphy F, Petruska PJ, Adkins D, Broun GO Jr, Spitzer G (1995) ASHAP with or without ABMT for high risk non-Hodgkin’s lymphoma (NHL). Proc Am Soc Clin Oncol 14:387 (Abstr 1205)
Velasquez W, Dunphy F, Santillana S, Adkins D, Browers C, Broun GO Jr, Petruska PJ, Spitzer G (1993) ASHAP, an effective treatment for relapsing and refractory Hodgkin’s disease (HD) and non-Hodgkin’s lymphoma (NHL). Blood 82(Suppl 1):138a (Abstr 538)
Coiffier B, Lepage E, Briere J et al (2002) CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med 346:235–242
Coiffier B, Haioun C, Ketterer N et al (1998) Rituximab (anti-CD20 monoclonal antibody) for the treatment of patients with relapsing or refractory aggressive lymphoma: a multicenter phase II study. Blood 92:1927–1932
Tobinai K, Igarashi T, Itoh K et al (2004) Japanese multicenter phase II and pharmacokinetic study of rituximab in relapsed or refractory patients with aggressive B-cell lymphoma. Ann Oncol 15:821–830
Rothe A, Schulz H, Elter T, Engert A, Reiser M (2004) Rituximab monotherapy is effective in patients with poor risk refractory aggressive non-Hodgkin’s lymphoma. Haematologica 89:875–876
Kewalramani T, Zelenetz AD, Nimer SD et al (2004) Rituximab and ICE as second-line therapy before autologous stem cell transplantation for relapsed or primary refractory diffuse large B-cell lymphoma. Blood 103:3684–3688
Venugopal P, Gretory S, Showel J et al (2004) Rituximab (Rituxan) combined with ESHAP chemotherapy is highly active in relapsed/refractory aggressive non-Hodgkin’s lymphoma. Blood (ASH Annual Meeting Abstracts) 104:4636, (Abstract)
Hicks L, Buckstein R, Piliotis E et al (2004) Rituximab + ESHAP as salvage chemotherapy for relapsed/refractory aggressive non-Hodgkins lymphoma: a phase II trial. Blood (ASH Annual Meeting Abstracts) 104:5230, (Abstract)
Mey U, Strehl J, Orlopp KS et al (2004) A phase II trial of dexamethasone, high-dose cytarabine, and cisplatin (DHAP) in combination with rituximab as salvage treatment for patients with refractory or relapsed aggressive non-Hodgkin’s lymphoma. Blood (ASH Annual Meeting Abstracts) 104:4618, (Abstract)
Rupolo M, Spina M, Michieli M et al (2004) R-DHAOX as salvage regimen in patients (pts) with relapsed/resistant non-Hodgkins lymphoma (NHL). Blood (ASH Annual Meeting Abstracts) 104:1323, (Abstract)
Wenger C, Stern M, Herrmann R, Rochlitz C, Pless M (2005) Rituximab plus gemcitabine: a therapeutic option for elderly or frail patients with aggressive non Hodgkin’s lymphoma? Leuk Lymphoma 46:71–75
Gnaoui T, Dupuis J, Joly B et al (2004) Rituximab, gemcitabine and oxaliplatin (R-GEMOX): a promising regimen for refractory/relapsed B-cell lymphoma. Blood (ASH Annual Meeting Abstracts) 104:2483, (Abstract)
Acknowledgement
This paper is dedicated to Professor Günter Brittinger on the occasion of his 75th birthday.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Aydin, S., Dührsen, U. & Nückel, H. Rituximab plus ASHAP for the treatment of patients with relapsed or refractory aggressive non-Hodgkin’s lymphoma: a single-centre study of 20 patients. Ann Hematol 86, 271–276 (2007). https://doi.org/10.1007/s00277-006-0243-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-006-0243-9