
Abstract
Plasmablastic lymphoma (PBL), an aggressive non-Hodgkin's lymphoma that carries a poor prognosis, previously has been identified almost exclusively in patients infected with the human immunodeficiency virus (HIV). We present a case of a 42-year-old HIV-negative patient presenting with an isolated nasal cavity mass, the typical presentation for PBL. The patient was given systemic chemotherapy, central nervous system prophylaxis, and consolidative locoregional radiotherapy and achieved a complete clinical response. This case suggests PBL should be considered in HIV-negative patients with characteristic findings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Plasmablastic lymphoma (PBL) is a lymphoproliferative disorder that is considered a diffuse large B-cell non-Hodgkin's lymphoma (NHL) morphologic variant by the currently proposed World Health Organization classification system [1]. Due to its recent recognition as a unique disease entity, the disorder has been only partially characterized, primarily on the basis of sporadic reports describing the condition in single or small patient series [2, 3, 4, 5, 6, 7, 8, 9, 10, 11]. To date, PBL has been found almost exclusively in patients infected with the human immunodeficiency virus (HIV), where a prevalence as high as 3% has been reported [3]. These patients characteristically present with extranodal disease involving the oral cavity. Unique laboratory features may aid in establishing a diagnosis. Various approaches to treatment have been described; however, responses are usually partial and of short duration, and survival is typically poor [3]. We describe an unusual case of PBL presenting in an HIV-negative patient and review the reported literature with respect to the pathophysiology, clinical features, and treatment of this uncommon disease.
Case history
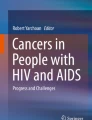
A previously healthy 42-year-old man presented for evaluation following the onset of rapidly progressive right-sided otalgia and hearing loss. He reported nasal obstructive symptoms of 3 months duration, which had not resolved with several courses of antibiotic therapy. He reported no fever, night sweats, or weight loss. The patient worked as a machinist and had no prior history of recreational drug use or homosexuality. On physical examination, the patient was found to have an obstructing mass lesion in the right nasal vestibule which completely obscured the nasal cavity (Fig. 1). He had no peripheral lymphadenopathy, organomegaly, or other remarkable findings.

Physical examination findings. The right intranasal mass presented with mass effect demonstrated by a bulge at the right nasal ala
Magnetic resonance imaging (MRI) of the brain revealed a diffusely enhancing soft tissue mass involving the right nasal cavity with partial destruction of the right nasal bone (Fig. 2). The right nasal mass, measuring 3.0×7.5×5.2 cm, extended to involve the right maxillary, sphenoid, and ethmoid sinuses, with associated post-obstructive sinus opacification. No intracranial extension was seen.

Magnetic resonance imaging of brain prior to therapy. Shown are transverse (A) and coronal views (B) of the brain demonstrating an expansile soft tissue mass involving the right nasal cavity and post-obstructive opacification of sphenoid, ethmoid, and maxillary sinuses
An intranasal biopsy of the right nasal mass was obtained for histopathologic, immunohistochemistry, and in situ hybridization studies [12, 13]. Hematoxylin and eosin-stained sections of the mass showed a variably cellular proliferation with clusters and diffuse sheets of highly atypical large cells with moderate to abundant eosinophilic cytoplasm surrounding pleomorphic nuclear profiles and prominent nucleoli (Fig. 3). Immunohistochemistry staining demonstrated reactivity for CD138, CD45, and kappa light chains; there was lack of immunoreactivity for CD30, cytokeratins, S100, CD20, CD79a, CD56, Bcl-1, and lambda light chains. These morphologic and immunophenotypic findings were consistent with a plasmablastic lymphoma [2, 10]. Furthermore, immunohistochemistry staining using a monoclonal antibody directed against the latent nuclear antigen 1 of human herpesvirus type 8 (HHV-8) showed no evidence of HHV-8 within lymphoma cells. In situ hybridization for Epstein-Barr virus (EBV) using the EBER-1 probe demonstrated EBV-specific RNA within atypical plasma cell nuclei.

Histopathologic examination of nasal mass biopsy specimen. A H&E-stained sections show a diffuse proliferation of atypical plasma cells with pleomorphic nuclear outlines and prominent nucleoli. B Immunohistochemistry for CD138 highlights membrane staining of the atypical plasma cells. C The stain for Ki-67 demonstrates nuclear staining in approximately 90% of the atypical cells. D Kappa light chain reactivity is seen in virtually all atypical cells. E Lambda light chain reactivity is restricted to rare scattered normal plasma cells. F In situ hybridization studies show EBV-specific RNA within numerous tumor cell nuclei. (×250)
Testing for HIV by a p24 antigen immunoassay was negative. A complete blood count revealed a white blood cell count of 8.4×109/l, hemoglobin of 14.0 g/dl, and platelet count 335×109/l. The serum lactate dehydrogenase level was normal. Serum and urine protein electrophoresis revealed no abnormal immunoglobulins. A complete radiographic skeletal survey was unremarkable. Computed tomography scans of the chest, abdomen, and pelvis revealed no significant abnormalities other than incidental findings of post-obstructive uropathy from prior bladder injury. Cytocentrifuged cerebrospinal fluid from a lumbar puncture was negative for malignant cells. A bone marrow biopsy was free of lymphoma. He was clinically staged as having a stage IEA neoplasm.
The patient was treated with three monthly courses of hyper-CVAD [14] chemotherapy at the following doses: cyclophosphamide 300 mg/m2 intravenously over 2 h every 12 h for a total of six doses given on days 1–3; vincristine 2 mg intravenous push on days 4 and 11; doxorubicin 50 mg/m2 intravenous push on day 4; and dexamethasone 40 mg/day orally on days 1–4 and days 11–14 [14]. Mesna 1000 mg/day by 24-h continuous infusion was given for 4 days with a 250-mg bolus prior to the first dose of cyclophosphamide. Prophylaxis against central nervous system relapse with intrathecal methotrexate (12 mg) was given with each chemotherapy cycle. Granulocyte colony-stimulating factor was administered starting on the 5th day of each course until adequate resolution of neutropenia.
The patient noted complete resolution of his presenting symptoms, including the hearing loss, after the first course of chemotherapy. Physical examination revealed near resolution of the right nasal mass. After three courses of chemotherapy, repeat MRI of the brain revealed substantial reduction in the dimensions of the nasal mass which now measured 1.5×1.9×1.3 cm (Fig. 4). A biopsy of the remaining tissue demonstrated inflammation and granulation without evidence of residual tumor.

Magnetic resonance imaging of brain following chemotherapy. Shown are transverse (A) and coronal views (B) of the brain demonstrating interval decrease in tumor bulk of right nasal mass
Consolidative locoregional radiation therapy followed. A total of 40 Gy was delivered to the right nasal cavity, ethmoid, and maxillary sinuses, and 36 Gy to the bilateral superior cervical areas using a three-dimensional conformal technique. Two weeks after completing radiation therapy, re-examination with MRI again revealed a persistent 1.5×1.5×1.0 cm soft tissue prominence. Another biopsy of this lesion revealed chronic inflammatory and granulating changes, similar to findings observed following the completion of chemotherapy as described above.
The patient tolerated treatment well with no grade 3 or 4 toxicity. Treatment concluded in September of 2002. His recent examination at 6 months showed no evidence of recurrence.
Discussion
PBL may be considered an HIV-related NHL, which is itself a heterogeneous group of diagnoses. Due to the paucity of patients that have been diagnosed with PBL, the pathophysiology is not well understood but may share common mechanisms with other HIV-related NHL. In contrast to an advanced stage presentation typical of these lymphomas, patients with PBL usually have localized oral disease as a first manifestation. Previously reported treatment for PBL has included administration of systemic chemotherapy, irradiation, and/or antiretroviral therapy. Responses are variable, but rapid progression has been described and long-term survival is uncommon.
A broad range of lymphomas has been described in HIV patients, where they collectively represent an acquired immunodeficiency syndrome-defining condition in about 3% [15, 16]. These include aggressive NHL such as Burkitt's lymphoma and immunoblastic lymphoma, as well as rare entities such as primary effusion lymphoma (PEL), lymphomatoid granulomatosis, and PBL [17, 18, 19]. Oncogenic aberrations have been identified in cases of HIV-related NHL. These include bcl-6 gene rearrangements, deregulated expression of c-myc, and loss of tumor suppressors such as p53 [20, 21, 22]. Immunoglobulin heavy chain variable genes bearing both germline as well as somatically hypermutated nucleotide sequences have also been observed [23].
Evidence supporting a pathogenic role for HHV-8 (Kaposi's sarcoma-associated herpesvirus) in promoting tumor formation has been described almost exclusively in HIV-related cases of PEL, multicentric Castleman disease (MCD), and MCD-associated plasmablastic lymphoma [24, 25, 26, 27]. In these diseases, an interaction between HIV and HHV-8 has been suggested whereby viral interleukin-6 (IL-6) may provide a potent mitogenic stimulus resulting in enhanced proliferation of HIV in patients co-infected with both viruses [27, 28, 29, 30]. Our HIV-negative patient had no evidence for infection by this virus.
Moreover, Epstein-Barr viral gene transcripts and products are commonly detected by molecular assays in HIV-related NHL. These include the EBV nuclear antigen 1 and latency membrane protein 1 gene products, which have been shown to contribute to cellular transformation in in vitro studies and the establishment of tumors in mouse models [31, 32]. In our patient, though HIV-negative, in situ hybridization for EBV demonstrated EBV-specific RNA within atypical plasma cell nuclei.
Much of what is known about the clinical features of PBL is derived from single patient cases and one reported series involving 16 patients [2, 3, 4, 5, 6, 7, 8, 9, 10, 11]. Almost all cases have been diagnosed in HIV-positive patients, although PBL arising as transformation from antecedent B-cell chronic lymphocytic leukemia has been described [33]. The most common presentation is an isolated extranodal mass in the oropharyngeal cavity, although unusual sites of initial disease involving the stomach, lung, testicles, and perianal area have been reported [6, 9, 34]. Complaints at presentation vary: asymptomatic mass, painful lesion, or nasal and sinus obstructive symptoms similar to those that prompted evaluation in our patient. Diagnostic tissue biopsy specimens ordinarily reveal a highly mitotic tumor composed of large neoplastic cells with abundant cytoplasm and eccentrically placed nuclei bearing prominent nucleoli, thus resembling the malignant cell found in multiple myeloma. Characteristic immunohistochemical findings include expression of CD138, VS38c, cytoplasmic CD79a, occasionally surface immunoglobulin, and absence of CD20 and other T-lineage markers.
An optimal chemotherapy regimen has not been established, and various modalities have been evaluated. Initial therapy has included administration of multiagent systemic chemotherapy or, alternatively, local irradiation alone [2]. Additionally, antiretroviral therapy alone has been reported to yield a remission of 3 months duration in a case of HIV-positive PBL [3]. Responses are variable and for the most part short-lived, including several descriptions of kinetically aggressive progressions during ongoing therapy [4, 9, 33]. In contrast to the localized nature at presentation, disease sites at progression are frequently widespread and have reportedly involved the central nervous system, abdominal viscera, and musculoskeletal soft tissue. No long-term survivors have been reported.
Our patient achieved an excellent response to initial therapy with an alkylator-based combination chemotherapy regimen and central nervous prophylaxis, followed by consolidative local irradiation. This case highlights an unusual presentation of a rare HIV-related NHL in an uninfected patient. Hence, the diagnosis of PBL should also be considered in HIV-negative individuals who present with characteristic features and findings.
References
Harris NL, Jaffe ES, Diebold J, et al. (2000) The World Health Organization classification of neoplasms of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting—Airlie House, Virginia, November 1997. Hematol J 1:53–66
Delecluse HJ, Anagnostopoulos I, Dallenbach F, et al. (1997) Plasmablastic lymphomas of the oral cavity: a new entity associated with the human immunodeficiency virus infection. Blood 89:1413–1420
Nasta SD, Carrum GM, Shahab I, Hanania NA, Udden MM (2002) Regression of a plasmablastic lymphoma in a patient with HIV on highly active antiretroviral therapy. Leuk Lymphoma 43:423–426
Flaitz CM, Nichols CM, Walling DM, Hicks MJ (2002) Plasmablastic lymphoma: an HIV-associated entity with primary oral manifestations. Oral Oncol 38:96–102
Borrero JJ, Pujol E, Perez S, Merino D, Montano A, Rodriguez FJ (2002) Plasmablastic lymphoma of the oral cavity and jaws. AIDS 16:1979–1980
Lin Y, Rodrigues GD, Turner JF, Vasef MA (2001) Plasmablastic lymphoma of the lung: report of a unique case and review of the literature. Arch Pathol Lab Med 125:282–285
Porter SR, Diz Dios P, Kumar N, Stock C, Barrett AW, Scully C (1999) Oral plasmablastic lymphoma in previously undiagnosed HIV disease. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 87:730–734
Carbone A, Gaidano G, Gloghini A, Ferlito A, Rinaldo A, Stein H (1999) AIDS-related plasmablastic lymphomas of the oral cavity and jaws: a diagnostic dilemma. Ann Otol Rhinol Laryngol 108:95–99
Pruneri G, Graziadei G, Ermellino L, Baldini L, Neri A, Buffa R (1998) Plasmablastic lymphoma of the stomach. A case report. Haematologica 83:87–89
Brown RS, Campbell C, Lishman SC, Spittle MF, Miller RF (1998) Plasmablastic lymphoma: a new subcategory of human immunodeficiency virus-related non-Hodgkin's lymphoma. Clin Oncol (R Coll Radiol) 10:327–329
Kochling G, Ochs A, Hauke G, Engelhardt R (1988) Plasmablastic immunoglobulin-secreting lymphoma. Report of a case and a glimpse at the prognosis. Klin Wochenschr 66:990–994
Natkunam Y, Smoller BR, Zehnder JL, Dorfman RF, Warnke RA (1999) Aggressive cutaneous NK and NK-like T-cell lymphomas: clinicopathologic, immunohistochemical, and molecular analyses of 12 cases. Am J Surg Pathol 23:571–581
van de Rijn M, Cleary ML, Variakojis D, Warnke RA, Chang PP, Kamel OW (1996) Epstein-Barr virus clonality in lymphomas occurring in patients with rheumatoid arthritis. Arthritis Rheum 39:638–642
Khouri IF, Romaguera J, Kantarjian H, et al. (1998) Hyper-CVAD and high-dose methotrexate/cytarabine followed by stem-cell transplantation: an active regimen for aggressive mantle-cell lymphoma. J Clin Oncol 16:3803–3809
Beral V, Peterman T, Berkelman R, Jaffe H (1991) AIDS-associated non-Hodgkin lymphoma. Lancet 337:805-809
Levine AM (1993) AIDS-related malignancies: the emerging epidemic. J Natl Cancer Inst 85:1382–1397
Carbone A (2002) AIDS-related non-Hodgkin's lymphomas: from pathology and molecular pathogenesis to treatment. Hum Pathol 33:392–404
Little RF, Gutierrez M, Jaffe ES, Pau A, Horne M, Wilson W (2001) HIV-associated non-Hodgkin lymphoma: incidence, presentation, and prognosis. JAMA 285:1880–1885
Jaffe ES, Wilson WH (1997) Lymphomatoid granulomatosis: pathogenesis, pathology and clinical implications. Cancer Surv 30:233–248
Gaidano G, Capello D, Gloghini A, et al. (1998) BCL-6 in aids-related lymphomas: pathogenetic and histogenetic implications. Leuk Lymphoma 31:39–46
Gaidano G, Carbone A, Dalla-Favera R (1998) Genetic basis of acquired immunodeficiency syndrome-related lymphomagenesis. J Natl Cancer Inst Monogr 23:95–100
Martin A, Flaman JM, Frebourg T, et al. (1998) Functional analysis of the p53 protein in AIDS-related non-Hodgkin's lymphomas and polymorphic lymphoproliferations. Br J Haematol 101:311–317
Cerri M, Capello D, Berra E, et al. (2002) Molecular histogenesis of plasmablastic lymphoma of the oral cavity (abstract). Blood 100:1813a
Boulanger E, Agbalika F, Maarek O, et al. (2001) A clinical, molecular and cytogenetic study of 12 cases of human herpesvirus 8 associated primary effusion lymphoma in HIV-infected patients. Hematol J 2:172–179
Du MQ, Diss TC, Liu H, et al. (2002) KSHV- and EBV-associated germinotropic lymphoproliferative disorder. Blood 100:3415–3418
Dupin N, Diss TL, Kellam P, et al. (2000) HHV-8 is associated with a plasmablastic variant of Castleman disease that is linked to HHV-8-positive plasmablastic lymphoma. Blood 95:1406–1412
Song J, Ohkura T, Sugimoto M, et al. (2002) Human interleukin-6 induces human herpesvirus-8 replication in a body cavity-based lymphoma cell line. J Med Virol 68:404–411
Gage JR, Breen EC, Echeverri A, et al. (1999) Human herpesvirus 8-encoded interleukin 6 activates HIV-1 in the U1 monocytic cell line. AIDS 13:1851–1855
Li H, Wang H, Nicholas J (2001) Detection of direct binding of human herpesvirus 8-encoded interleukin-6 (vIL-6) to both gp130 and IL-6 receptor (IL-6R) and identification of amino acid residues of vIL-6 important for IL-6R-dependent and -independent signaling. J Virol 75:3325–3334
Chatterjee M, Osborne J, Bestetti G, Chang Y, Moore PS (2002) Viral IL-6-induced cell proliferation and immune evasion of interferon activity. Science 298:1432–1435
Ambinder RF (2001) Epstein-Barr virus associated lymphoproliferations in the AIDS setting. Eur J Cancer 37:1209–1216
Crawford DH (2001) Biology and disease associations of Epstein-Barr virus. Philos Trans R Soc Lond B Biol Sci 356:461–473
Robak T, Urbanska-Rys H, Strzelecka B, et al. (2001) Plasmablastic lymphoma in a patient with chronic lymphocytic leukemia heavily pretreated with cladribine (2-CdA): an unusual variant of Richter's syndrome. Eur J Haematol 67:322–327
Podrumar A, Sanmugarajah J, Levine R (2002) Plasmablastic lymphoma of the testicles in a patient with acquired immunodeficiency (abstract). Blood 100:4645a
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nguyen, D.D., Loo, B.W., Tillman, G. et al. Plasmablastic lymphoma presenting in a human immunodeficiency virus-negative patient: a case report. Ann Hematol 82, 521–525 (2003). https://doi.org/10.1007/s00277-003-0684-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-003-0684-3