
Abstract
Purpose
This study aimed to quantify mandibular ramus height and condylar distances asymmetry indexes in adult patients with different vertical facial growth pattern using Cone Beam computed tomography (CBCT).
Methods
An observational cross-sectional study was conducted by using CBCT of 159 patients (mean age 26.36 ± 5.32 years). Vistadent 3D® software was used to determine the facial pattern in 3 groups (N = 53): hypodivergent, normodivergent and hyperdivergent—by Ricketts VERT index. Mandibular ramus height and the condylar linear distance in relation to the median sagittal plane were evaluated. The asymmetry index was calculated considering the right and left sides. Data were analyzed by generalized linear models and Tukey post-hoc test (α = 0.05).
Results
Significantly lower values were found for the left and right mandibular ramus height in the hyperdivergent skeletal pattern (P < 0.05). There was no statistically significant difference for condylar and intercondylar distances among the facial groups (P > 0.05). Asymmetry indexes (mandibular ramus height and condylar distance) were similar, and no statistically significant differences were found among the skeletal patterns. In most subjects, the severity of mandibular ramus height asymmetry varied from light to not clinically significant independently of the facial type.
Conclusion
The findings suggest that vertical facial growth pattern not affected the asymmetry index of mandibular ramus height and the intercondylar distance. The results also demonstrated significantly shorter mandibular ramus height for the hyperdivergent skeletal pattern individuals.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Craniofacial growth has no absolute lateral uniformity, and therefore, even faces considered pleasing may have some asymmetry [39]. Based on the classification proposed by Wolford, a normal facial asymmetry (nonpathological) may be due genetics defects, intrauterine molding and natural growth variance and also environmental factors [40]. Although controversial, linear, and volumetric mandibular asymmetries seem to be more prevalent among men. However, this condition appears to be strongly associated with the sagittal jaw relationship showing a predilection for Class III and hyperdivergent patterns [28, 37]. The asymmetric growth of mandible may increase the risk of facial asymmetry [17]. Although controversial, asymmetry of mandibular specific components such as the ramus height may be only characterized as a morphological predictor of risk not establishing a cause-effect relationship [22].
From a clinical perspective, both mandibular ramus height and condyle characteristics have been characterized as common causative factors for facial asymmetry and may be related to the vertical skeletal facial pattern [14, 39]. For instance, it is suggested that the mandibular ramus height is lower in individuals with a hyperdivergent pattern, however, discrepant data have been obtained relative to the prevalence of ramus height asymmetry among the different facial types [4, 28], and probably there was no significant difference in asymmetry between the right and left sides [6, 23].
Moreover, hyperdivergent faces have been associated with a more lateral condylar position in relation to the glenoid fossa [1]. Evidences based on experimental animal models have pointed out that during craniofacial development, the medial and lateral pterygoid muscles determine a preponderant effect on reduction in the medial movement of the mandibular ramus and, consequently, intercondylar distance [29].
The condyle plays an important role as a growth center in the mandible and abnormal stress distribution on its articular surfaces, caused by imbalanced occlusion, in patients with mandibular asymmetry may result in internal derangement and functional impairment of the temporomandibular joints (TMJs) [41]. References to possible normally occurring asymmetries in the TMJs, are much fewer than those concerning other asymmetries in the craniomandibular region however, vertical skeletal discrepancies influence the condylar position and may impact on positional asymmetries between the condyles and median sagittal plane [34]. Up to now, no study has evaluated the influence of the intercondylar distance on the degree of severity of facial asymmetries [6, 23].
Morphometric aspects such as the mandibular ramus and intercondylar distance may be associated with mandibular asymmetry can be considered as etiological or predisposing factors for the development of TMD conditions [12]. Therefore, establishing the morphometric differences among the different mandibular constituents could help with understanding the etiology of asymmetries of the inferior third of the face and the associated pathologies [28]. Moreover, the establishment of clinical patterns of asymmetries considered normal is of clinical interest, with the purpose of not characterizing acceptable discrepancies as pathologies. The aim of this study was to quantify, by means of cone beam computed tomography, the mandibular ramus height and condylar distance asymmetry indices in adult patients with different vertical facial patterns.
Materials and methods
Sample
This observational cross-sectional study was approved by the Research Ethics Committee of the University Center of the Hermínio Ometto Foundation—FHO (#01820118.8.0000.5385). Included in this study were 159 cone beam computed tomography (CBCT) images of patients with a mean age of 26.36 ± 5.32 years. The sample size was calculated assuming a mean difference of 0.5 mm and 1 mm in the intercondylar distance among groups based on a pilot-study (data not shown). To detect a significance level of 5%, test power of 80%, we obtained a final Group of 53 subjects per Group (N = 53) which guaranteed a mean effect size according to Cohen, 1992 [9]. Dimensioning was performed in the G*Power software (Version 3.1.9.2).
The CBCT images of patients of both sexes (sex ratio male–female of 1:1.94) were randomly selected and used for analyzing the craniofacial structures and mandibular morphology. This study included images of patients without history of previous orthodontic treatment, missing teeth, systemic diseases that can affect the maxillofacial bones, pathological conditions in the craniomaxillofacial complex, history of trauma or oral maxillofacial surgery, cross bite, or syndromes.
CBCT and image analysis protocols
All the CBCT images were previously obtained with the same apparatus (i-CAT unit, Imaging Sciences International, Hatfield, Pa) under the following conditions: 120 kVp, 8 mA; scanning time, 40 s, 0.3 mm3 voxel size and field of view (FOV) of 23 × 17 cm. The images were transformed into Dicom file format. Vistadent 3D 2.0 software (GAC Dentsply, New York, NY, USA) was used to perform all measurements. The tomographic analysis was made in accordance with the protocol previously established by Gribel e cols. (2011) [16]. Since during the acquisition of cone beam computed tomography images, the position of the patient’s head may vary from one exam to the other, of the patient does not remain in the correct position, therefore the tool “set natural head position” was used [36].
The cephalometric points for determining both the growth pattern and those for evaluating asymmetry were identified by a single, calibrated operator. After this, the planes of reference were determined, and the linear and angular measurements were automatically calculated by the software. The dolychofacial, mesofacial and brachyfacial facial growth patterns were established by means of the Ricketts VERT index [10, 26, 33]. The index is comprised of the arithmetic mean values of the following parameters: facial axis—Pt-Gn. Ba-Na; depth of the face—N-P.Po-Or; mandibular plane angle—Go-Me.Po-Or; lower anterior facial height—Xi-eNa.Xi-Pm and mandibular arch—Xi-Dc.Xi-Pm. In this study, the vertical facial growth pattern was categorized as follows: brachyfacial (hypodivergent) (VERT > + 0.5), dolychofacial (hyperdivergent) (VERT < − 0.5) and mesofacial (normodivergent) (0.5 ≤ VERT ≤ 0.5).
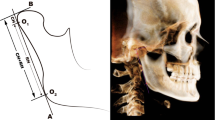
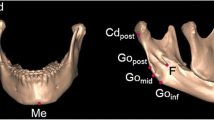
The measurements of the mandibular ramus heights (right and left) were determined in a multiplanar reconstruction by means of evaluation the distance between the condylar point (most posterior and superior of the condyle) and the gonial point (Co-Go) based on a methodology previously described by Habets (1988) and Celikoglu (2013) (Fig. 1) [5, 18]. To evaluate the asymmetry of the condylar distance in relation to the median sagittal plane, the following were established in the axial cut: the distance from the largest mesiodistal width of the condyle, the geometric center of the condylar process (intersection between the largest anteroposterior and mediolateral) distances and the median sagittal plane (ENA-ENP), perpendicular to the Frankfort (Po-Or) (Fig. 2) [5, 15].

Evaluation of mandibular ramus height

Evaluation of condylar distance in relation to the median sagittal plane based on the geometric centers of the mandibular condylar process (right and left) to the median sagittal plane
The mandibular ramus and condylar distance asymmetry indices (RHAI and CDAI, respectively) were calculated using the formula described previously, considering the right and left sides [18]. The indices were calculated based on the ratio between the differences of distances between the right and left sides over the sum of the right and left side differences. RHAI ratios were expressed in percentile and classified according to its severity as follows: not significant (≤ 2.99%); light (3% ≥ 5%); moderate (5.1% ≥ 10%); and severe (≤ 10.1%) [32]. Only the clinical levels of significance of asymmetries for the right and left condylar distances (CDAI) above 3% were considered relevant, according to the limit established previously [18].
Error of the method
All 159 CBTC were reevaluated by the same examiner with a 1-month interval in between the assessments. Casual error was calculated according to Dahlberg's formula ranging from 0.04 to 0.08 for the linear measurements. The resulting error was considered acceptable [3]. Systematic error was calculated based on the interclass correlation coefficient and ranged from 0.01 to 0.03, indicating a low risk of biases.
Statistical analysis
The asymmetry and ramus height data did not meet the presupposition of the analysis of variance (ANOVA) and were analyzed by generalized linear models. Analysis of the percentage of participants with asymmetries were performed by the Chi-square test. The analyses were carried out with a level of significance of 5%. All inferential tests were conducted by using the “R” software (R Core Team 2018. R Foundation for Statistical Computing, Vienna, Austria).
Results
The average linear distances of mandibular ramus height and condylar distances variables are shown in Table 1. The ramus height parameters of the hyperdivergent group were significantly shorter than the normodivergent and hypodivergent skeletal patterns (all P < 0.05). Whereas, there was no significant difference between the linear measurements in the ramus height of normodivergent and hypodivergent patterns (P > 0.05). With regard to the condylar distances (distances between the geometric centers of the condylar process of the mandible and the median sagittal plane on both TMJs) and the intercondylar distances of the TMJs), there was no significant difference among the different skeletal patterns (P > 0.05).
The results of RHAI and CDAI of the three different facial skeletal patterns are shown in Table 2. The effect of the facial growth pattern on RHAI was not statistically significant (P = 0.0822). For its asymmetry severity, we also found a nonsignificant correlation regarding the percentile distribution among the different skeletal types. Also, RHAI classified as nonsignificant and light were found in a high percentage of the subjects (90.5%, hypodivergent; 81.1%, hyperdivergent; 96.2%, normodivergent). Finally, the asymmetry of the geometric position of the condylar processes (distances between the geometric centers of the left and right mandibular condylar process and the median sagittal plane) (CDAI) showed no significant difference among the groups. The result of the Chi-square test (× 2), by means of which the prevalence of individuals with CDAI was analyzed at the cutoff point (> 3%), demonstrated that there was no statistical difference between the facial groups (P > 0.5). Regarding predilection for the right or left side, no significant differences were observed (data not presented).
Discussion
The morphometric equilibrium of craniofacial structures, such as the mandibular ramus and condylar distances may be associated with a condition of functional equilibrium, because there is correspondence of a dimensional nature and of disposition between the antimeric structures in relation to the median sagittal plane [13]. Decisions about intervention for mandibular asymmetry depend on different factors, such as vertical jaw imbalance. To date, published mandibular vertical asymmetry CBTC data have not considered vertical measurement of the face, although it represents an anatomical feature that is related with ramus height and other structural components of the mandible. The body of evidence generated in this study was based on a homogeneous population sample in terms of age and gender, using CBCT, the method considered the gold standard for this type of craniometric analysis, because it avoids errors of magnification and distortion [5, 18]. With the purpose of not affecting the results, individuals with the presence of cross bite, temporomandibular dysfunction, or those still at the stage of growth were excluded from this study.
Previous studies have suggested that there was a tendency for individuals with the hyperdivergent growth pattern to have more severe craniomandibular asymmetries [17, 28]. In the present study, the mandibular ramus height asymmetry index did not differ among the groups, and the mean asymmetry distance found ranged between 0–3 mm; that is, within a morpho functional limit without clinical impact [32, 35]. This indicated an almost symmetrical vertical mandibular ramus height in all the groups studied. Similarly, no statistically significant differences were observed in patients with the facial profile determined by the SN-MP angle [4]. Possibly, this premise that the hyperdivergent type showed more severe asymmetries could be due to the fact that observations were made in individuals during the stage of growth, or by observation of the asymmetry of other mandibular structures such as height of the condyle and mandibular plane angle [4, 8, 32].
Different methods could be proposed for assessing the ramus height. However, the measurement protocol applied in the current study based on distance between the most cranial point of the condyle (Co) and the gonial point (Go) enabled the comparison of the current results with studies that consider the same the same anatomical landmarks but uses different imaging procedures such as computed tomography, magnetic resonance imaging, orthopantomography, and lateral cephalometry [27]. The mandibular ramus height was significantly lower in the hyperdivergent group; this finding corroborates those of other studies that evaluated this vertical discrepancy by both CBCT and cephalometric analysis [2, 25]. The deficiency in the ramus height may possibly have contributed to the characterization of a more vertical face due to its association with the increase in anteroinferior facial height (AIFH) determined by the increase in the mandibular plane angle. It is of clinical interest, however, to emphasize that the increase in the posterior height of the face would be directly proportional to the increase in the ramus height [20]. The results presented contradicted the presupposition that individuals with a balanced face would have a larger ramus height than those with the hypodivergent facial pattern. Therefore, we suggest that a greater contribution to the vertical facial discrepancies would be determined by change in the mandibular plane angle, as well as in the other horizontal planes, rather than by the dimensional change in the mandibular ramus. Another possible hypothesis would be that in the present study included threshold cases, which may have led to the observation of statistical difference, because a higher percentage of facial asymmetry of skeletal Class III individuals was due to deviation of the chin and displacement of the mandibular body [6].
Therefore, when we evaluated the metric characteristics of the mandibular ramus height in conjunction with its asymmetry index according to the facial growth pattern, we suggest that although reduction in the mandibular ramus height promotes hemi-mandibular shortening associated with the hyperdivergent pattern [30], compensatory muscular mechanisms may be associated with more symmetrical ramus heights [19].
Whereas, other compensatory mechanisms, such as condylar and glenoid fossa remodeling, suggest that positional asymmetries may be an adaptive response to functional demands [13]. We expected that higher transcranial asymmetry indices in the axial plane would occur in the hyperdivergent growth pattern group due to the intra-articular characteristics associated with this facial type, such as the more superior positioning of the mandibular condyle in relation to the articular fossa and its smaller dimensions in the coronal plane [15, 31]. However, the results of the present study showed a predominance of slightly mandibular asymmetry for all patients irrespective of the facial type (P > 0.05). Previous studies have suggested that the condylar position varied according to the facial typology and they are associated with craniomandibular asymmetry, therefore, orthodontic and/or orthopedic intervention would be necessary for the prevention/redirection of vertical discrepancies of the face [20, 29, 36]. However, the main clinical implication that the present results suggest is that the condylar position may be the result of various dynamic changes of different anatomical structures, myofunctional adaptation and individual variations. Therefore, it is probably not directly associated with a specific facial growth pattern.
Asymmetric condylar distances from the mid sagittal plane may be a contributor factor for other pathological conditions such as temporomandibular joint disorders, and yet little research has been carried out into this field. The reference values of transcranial condylar distances obtained in this study by means of CBCT are complementary to the other dentoskeletal symmetry findings, such as those provided by clinical and model analyses [7, 11, 24, 38]. The present results demonstrated mean intercondylar distance values close to those reported in the literature [38], and that they do not vary according to the vertical facial typology, as has previously been suggested [11, 21]. Although the indices obtained in the population of the present study, by means of CBCT exams, may function as predictive values for identifying and measuring the ramus height and condylar positioning asymmetries during orthodontic and surgical planning, further studies need to be conducted to clarify whether other mandibular areas in these individuals can be considered causal factors in this condition, including mandibular condyle and mandibular body.
Conclusion
It was concluded that the ramus height and condylar distance asymmetry indices did not vary according to the facial typology and its severity, in the sample population, was characterized as not clinically significant. In additions, hyperdivergent individuals had lower mandibular ramus height values, and the intercondylar distance was not influenced by the vertical facial pattern.
References
Alhammadi MS, Fayed MMS, Labib A (2016) Comprehensive three-dimensional cone beam computed tomography analysis of the temporomandibular joint in different vertical skeletal facial patterns. J World Fed Orthod 5(1):9–17. https://doi.org/10.1016/j.ejwf.2016.02.001
Buschang PH, Jacob H, Carrillo R (2013) The morphological characteristics, growth, and etiology of the hyperdivergent phenotype. Semin Orthod 19(4):212–226. https://doi.org/10.1053/j.sodo.2013.07.002
Cançado RH, Lauris JR (2014) Error of the method: what is it for? Dental Press J Orthod 19(2):25–26. https://doi.org/10.1590/2176-9451.19.2.025-026.ebo
Celik S, Celikoglu M, Buyuk SK, Sekerci AE (2016) Mandibular vertical asymmetry in adult orthodontic patients with different vertical growth patterns: a cone beam computed tomography study. Angle Orthod 86(2):271–277. https://doi.org/10.2319/030515-135.1
Celikoglu M, Halicioglu K, Buyuk SK, Sekerci AE, Ucar FI (2013) Condylar and ramal vertical asymmetry in adolescent patients with cleft lip and palate evaluated with cone-beam computed tomography. Am J Orthod Dentofac Orthop 144(5):691–697. https://doi.org/10.1016/j.ajodo.2013.07.009
Chen YJ, Yao CC, Chang ZC, Lai HH, Lu SC, Kok SH (2016) A new classification of mandibular asymmetry and evaluation of surgical-orthodontic treatment outcomes in Class III malocclusion. J Craniomaxillofac Surg 44(6):676–683. https://doi.org/10.1016/j.jcms.2016.03.011
Christiansen EL, Chan TT, Thompson JR, Hasso AN, Hinshaw DB Jr, Kopp S (1987) Computed tomography of the normal temporomandibular joint. Scand J Dent Res 95(6):499–509. https://doi.org/10.1111/j.1600-0722.1987.tb01966.x
Chung CH, Mongiovi VD (2003) Craniofacial growth in untreated skeletal Class I subjects with low, average, and high MP-SN angles: a longitudinal study. Am J Orthod Dentofac Orthop 124(6):670–678. https://doi.org/10.1016/j.ajodo.2003.02.004
Cohen J (1992) A power primer. Psychol Bull 112(1):155–159. https://doi.org/10.1037/0033-2909.112.1.155
Costa EDD, Peyneau PD, Roque-Torres GD et al (2019) The relationship of articular eminence and mandibular fossa morphology to facial profile and gender determined by cone beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol 128(6):660–666. https://doi.org/10.1016/j.oooo.2019.07.007
Debnath N, Gupta R, Meenakshi A, Kumar S, Hota S, Rawat P (2014) Relationship of inter-condylar distance with inter-dental distance of maxillary arch and occlusal vertical dimension: a clinical anthropometric study. J Clin Diagn Res 8(12):ZC39–43. https://doi.org/10.7860/JCDR/2014/10194.5289
D'Ippolito S, Ursini R, Giuliante L, Deli R (2014) Correlations between mandibular asymmetries and temporomandibular disorders (TMD). Int Orthod 12(2):222–238. https://doi.org/10.1016/j.ortho.2014.03.013
Duthie J, Bharwani D, Tallents RH, Bellohusen R, Fishman L (2007) A longitudinal study of normal asymmetric mandibular growth and its relationship to skeletal maturation. Am J Orthod Dentofac Orthop 132(2):179–184. https://doi.org/10.1016/j.ajodo.2005.07.032
Fields HW, Proffit WR, Nixon WL, Phillips C, Stanek E (1984) Facial pattern differences in long-faced children and adults. Am J Orthod 85(3):217–223. https://doi.org/10.1016/0002-9416(84)90061-7
Ganugapanta VR, Ponnada SR, Gaddam KP, Perumalla K, Khan I, Mohammed NA (2017) Computed tomographic evaluation of condylar symmetry and condyle-fossa relationship of the temporomandibular joint in subjects with normal occlusion and malocclusion: a comparative study. J Clin Diagn Res 11(2):29–33. https://doi.org/10.7860/JCDR/2017/21678.932
Gribel BF, Gribel MN, Frazäo DC, McNamara JA Jr, Manzi FR (2011) Accuracy and reliability of craniometric measurements on lateral cephalometry and 3D measurements on CBCT scans. Angle Orthod 81(1):26–35. https://doi.org/10.2319/032210-166.1
Good S, Edler R, Wertheim D, Greenhill D (2006) A computerized photographic assessment of the relationship between skeletal discrepancy and mandibular outline asymmetry. Eur J Orthod 28(2):97–102. https://doi.org/10.1093/ejo/cji097
Habets LL, Bezuur JN, Naeiji M, Hansson TL (1988) The orthopantomogram, an aid in diagnosis of temporomandibular joint problems. II. The vertical symmetry. J Oral Rehabil 15(5):465–471. https://doi.org/10.1111/j.1365-2842.1988.tb00182.x
Kambylafkas P, Kyrkanides S, Tallents RH (2005) Mandibular asymmetry in adult patients with unilateral degenerative joint disease. Angle Orthod 75(3):305–310
Karlsen AT (1997) Association between facial height development and mandibular growth rotation in low and high MP-SN angle faces: a longitudinal study. Angle Orthod 67(2):103–110
Lazić B, Tepavcević B, Keros J, Komar D, Stanicić T, Azinović Z (2006) Intercondylar distances of the human temporomandibular joints. Coll Antropol 30(1):37–41
Leung MY, Leung YY (2018) Three-dimensional evaluation of mandibular asymmetry: a new classification and three-dimensional cephalometric analysis. Int J Oral Maxillofac Surg 47(8):1043–1051. https://doi.org/10.1016/j.ijom.2018.03.021
Lim YS, Chung DH, Lee JW, Lee SM (2018) Reliability and validity of mandibular posterior vertical asymmetry index in panoramic radiography compared with cone-beam computed tomography. Am J Orthod Dentofacial Orthop 153(4):558–567. https://doi.org/10.1016/j.ajodo.2017.08.019
Mandilaris CB, Beard CC, Clayton JA (1992) Comparison of the intercondylar distance and the interfacial width as used with the electronic pantograph. J Prosthet Dent 67(3):331–334. https://doi.org/10.1016/0022-3913(92)90241-2
Mangla R, Singh N, Dua V, Padmanabhan P, Khanna M (2011) Evaluation of mandibular morphology in different facial types. Contemp Clin Dent 2(3):200–206. https://doi.org/10.4103/0976-237X.86458
Manns A, Valdivieso C, Rojas V, Valdés C, Ramírez V (2018) Comparison of clinical and electromyographic rest vertical dimensions in dolichofacial and brachyfacial young adults: a cross-sectional study. J Prosthet Dent 120(4):513–519. https://doi.org/10.1016/j.prosdent.2017.11.017
Markic G, Müller L, Patcas R et al (2015) Assessing the length of the mandibular ramus and the condylar process: a comparison of OPG, CBCT, CT, MRI, and lateral cephalometric measurements. Eur J Orthod 37(1):13–21. https://doi.org/10.1093/ejo/cju008
Mendoza LV, Bellot-Arcís C, Montiel-Company JM, García-Sanz V, Almerich-Silla JM, Paredes-Gallardo V (2018) Linear and volumetric mandibular asymmetries in adult patients with different skeletal classes and vertical patterns: a cone-beam computed tomography study. Sci Rep 8:12319. https://doi.org/10.1038/s41598-018-30270-7
Monje F, Delgado E, Navarro MJ, Miralles C, Alonso del Hoyo JR (1994) Changes in the temporomandibular joint caused by the vertical facial pattern. Study on an experimental model. J Craniomaxillofac Surg 22(6):361–370. https://doi.org/10.1016/s1010-5182(05)80118-0
Obwegeser HL, Makek MS (1986) Hemimandibular hyperplasia–hemimandibular elongation. J Maxillofac Surg 14:183–208. https://doi.org/10.1016/s0301-0503(86)80290-9
Park IY, Kim JH, Park YH (2015) Three-dimensional cone-beam computed tomography-based comparison of condylar position and morphology according to the vertical skeletal pattern. Korean J Orthod 45(2):66–73. https://doi.org/10.4041/kjod.2015.45.2.66
Ramirez-Yañez GO, Stewart A, Franken E, Campos K (2011) Prevalence of mandibular asymmetries in growing patients. Eur J Orthod 33(3):236–242. https://doi.org/10.1093/ejo/cjq057
Ricketts RM, Roth RH, Chaconas SJ, Schulhof RJ, Engel GA (2011) Orthodontic diagnosis and planning: their roles in preventive and rehabilitative dentistry. Rock Mountain Data Systems, Denver
Roque-Torres GD, Peyneau PD, Dantas da Costa E, Bóscolo FN, Maria de Almeida S, Ribeiro LW (2018) Correlation between midline deviation and condylar position in patients with Class II malocclusion: a cone-beam computed tomography evaluation. Am J Orthod Dentofac Orthop 154(1):99–107. https://doi.org/10.1016/j.ajodo.2017.10.029
Skvarilová B (1993) Facial asymmetry: type, extent and range of normal values. Acta Chir Plast 35(3–4):173–180
Swasty D, Lee J, Huang JC, Maki K, Gansky SA, Hatcher D, Miller AJ (2011) Cross-sectional human mandibular morphology as assessed in vivo by cone-beam computed tomography in patients with different vertical facial dimensions. Am J Orthod Dentofac Orthop 139(4):e377–389. https://doi.org/10.1016/j.ajodo.2009.10.039
Thiesen G, Gribel BF, Kim KB, Pereira KCR, Freitas MPM (2017) Prevalence and associated factors of mandibular asymmetry in an adult population. J Craniofac Surg 28(3):e199–e203. https://doi.org/10.1097/SCS.0000000000003371
Tradowsy M (1990) Sex difference in intercondylar distance. J Prosthet Dent 63(3):301–302. https://doi.org/10.1016/0022-3913(90)90200-v
Wang MF, Otsuka T, Akimoto S, Sato S (2013) Vertical facial height and its correlation with facial width and depth: three-dimensional cone beam computed tomography evaluation based on dry skulls. Int J Stomatol Occlusion Med 6:120–129. https://doi.org/10.1007/s12548-013-0089-4
Wolford LM (2009) Facial asymmetry: diagnosis and treatment considerations. In: Turvey TA (ed) Oral and maxillofacial surgery, 2nd edn. Saunders, St. Louis, pp 272–315
Zhao C, Kurita H, Kurashina K, Hosoya A, Arai Y, Nakamura H (2010) Temporomandibular joint response to mandibular deviation in rabbits detected by 3D micro-CT imaging. Arch Oral Biol 55(12):929–937. https://doi.org/10.1016/j.archoralbio.2010.07.019
Funding
No research grants from funding agencies or financial supports were associated with this study.
Author information
Authors and Affiliations
Contributions
CRL: protocol/project development, manuscript writing/editing. CFT: manuscript writing/editing. SG: data collection. BFG: data collection. GCV: data analysis. CCM: data analysis, manuscript writing. WC: protocol/project development, manuscript writing/editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the Research Ethics Committee of the University Center of the Hermínio Ometto Foundation—FHO under protocol number CAAE 01820118.8.0000.5385, national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lemes, C.R., Tozzi, C.F., Gribel, S. et al. Mandibular ramus height and condyle distance asymmetries in individuals with different facial growth patterns: a cone-beam computed tomography study. Surg Radiol Anat 43, 267–274 (2021). https://doi.org/10.1007/s00276-020-02577-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-020-02577-6