
Abstract
We have found an interesting coincidental variation of the superficial branch of the radial nerve and the brachioradialis muscle in a male cadaver. The superficial branch of the radial nerve was duplicated with one branch taking an aberrant course between two bellies of the brachioradialis muscle. The variant brachioradialis muscle featured two muscle bellies, a superficial one and a deep one, with one common origin and one common insertional tendon. The accessory nerve branch was impinged by two blood vessels and pierced through muscle bundles connecting two bellies of the brachioradialis muscle. The knowledge of this neuromuscular variant is of clinical relevance for the differential diagnosis of pain and paresthesia on the dorsoradial aspect of the hand and for the surgical management of the Wartenberg’s syndrome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The superficial branch of the radial nerve (SBRN) is a sensory nerve innervating the dorsoradial aspect of the hand and the dorsal side of the thumb and index finger and a variable extent of the dorsal aspect of the middle finger and radial side of the ring finger. It usually originates within the cubital fossa as a branch of the radial nerve and continues distally underneath the belly of the brachioradialis muscle (BM), accompanied by the radial vessels. In the distal forearm, the SBRN emerges from under the tendon of the BM at a mean distance of 8.54 cm proximal to the styloid process of the radius [8]. It becomes subcutaneous at a mean distance of 9 cm [4] proximal to the styloid process of the radius, which is, on average, distal 36 % of the forearm (measured from the lateral humeral epicondyle to the styloid process of the radius) [4]. It bifurcates into its terminal branches at a mean distance of 5.1 cm proximal to the styloid process of the radius [4].
The usual course of the SBRN is well known and taken into consideration when performing various medical procedures, such as the treatment of De Quervain’s tenosynovitis, percutaneous fixation using Kirschner’s wires, cannulation of the cephalic vein, and regional nerve blockade. Variations of the SBRN, such as connections with the lateral antebrachial cutaneous nerve [2] and the dorsal branch of the ulnar nerve [2], can lead to medical complications when performing these procedures, unlike the complete absence of the SBRN, which is clinically silent [1].
The reported variation, an accessory superficial branch of the radial nerve, is a very rare variant, mentioned only indirectly by Murphy and Blair in their clinical case of the Wartenberg´s syndrome. They report that it was caused by an unusual branch of the radial nerve piercing the BM and joining the SBRN, without neither anatomical background nor description of the origin and course of the accessory branch [7]. The SBRN was reported in relation to the variant BM only by Turkof et al., when emerging from under the muscle between its two “slips”. According to the text and figures, the nerve emerged between the divided (split) insertional tendons of the BM. The incidence of the divided tendon was 6 % (9/150) and that of the SBRN passing between the tendons at the site of bifurcation was 3.3 % (5/150) [10]. The incidence of the BM variant concerning its supernumerary bellies is not available, there are only case reports, summarized and reported by Gruber [5].
Case report
A unique variation was found during a routine student dissection course (at the First Faculty of Medicine, Charles University in Prague) in the cadaver of a male donor (67 years) with a medical history without any reported sensory or motor defects in the upper limb. The forearm was 305 mm long (distance between the olecranon and the styloid process of the ulna) and the interepicondylar line (IL) was 68 mm. The radial nerve (RN) unusually divided in the cubital fossa into three branches: the deep branch of the radial nerve (DBRN), the SBRN (1.5 mm thick), and an accessory superficial branch of the radial nerve (ASBRN; 1 mm thick). The BM (342 mm long) featured two muscle bellies, superficial (192 mm long, 18 mm wide, 1 mm thick), and deep (164 mm long, 21 mm wide, 2 mm thick) with one common origin and one common insertional tendon. The SBRN ran under the deep belly and the ASBRN ran under the superficial belly. After these two nerves emerged from underneath the muscle, they fused together into one nerve trunk and continued distally. They again divided after 17 mm into two branches and innervated the dorsoradial aspect of the hand (see Fig. 1). After dissection of the nerve fibers, it was found that the ASBRN innervated the dorsoradial side of the thumb (having two branches) and the SBRN innervated the rest of the dorsoradial aspect of the hand as far as the radial side of the middle finger (having three branches) (see Fig. 2a). While running under the BM, the ASBRN was crossed by two muscular branches of the radial artery (22 mm and 73 mm distal to IL, respectively) before piercing muscle bundles interconnecting the two bellies of the BM (96–106 mm distal to IL) (see Fig. 2b). The nerves were artificially coloured by means of software GIMP 2 in all figures. As for the distances from anatomical landmarks, the distance between IL and the beginning of the common nerve trunk of the SBRN and ASBRN was 189 mm, the distance between IL and the origin of the ASBRN was 54 mm, the distance between IL and the origin of the SBRN was only 3 mm, the distance between IL and the point of emergence of the SBRN from underneath the BM was 155 mm, the distance between IL and the point of emergence of the ASBRN from underneath the BM was 129 mm, and finally, the distance between the styloid process of the radius and the point of division of the SBRN into its terminal branches was 13 mm.

Two-bellied brachioradialis muscle. The ASBRN (2) courses under the superficial belly of the BM (1) and the SBRN (4) runs under the deep belly of the BM (3). These nerve branches merge into one common nerve trunk (5)

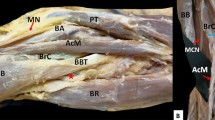
Branching of the superficial branch of the radial nerve (a) and potential entrapment sites of the accessory superficial branch of the radial nerve (b). The ASBRN innervates the dorsoradial side of the thumb, (2) while the SBRN innervates the dorsoradial aspect of the index finger and middle finger (1). The ASBRN is crossed by two muscular branches of the radial artery (3, 4) and pierces muscle bundles interconnecting the two bellies of the BM (5)
Discussion
The ASBRN is crossed by two blood vessels and pierces several muscle bundles, as it runs under the belly of the brachioradialis muscle. Muscle hypertrophy due to extensive exercise could be a possible cause of the entrapment syndrome of the SBRN (Wartenberg’s syndrome). This syndrome is often misdiagnosed as De Quervain’s tenosynovitis or is not diagnosed at all [6]. Some papers report entrapment of the SBRN between two slips of a split BM tendon [11] or compression due to an accessory BM [9]. Murphy and Blair described a clinical case of 28-year-old female with Wartenberg´s syndrome caused by an unusual branch of RN piercing the BM and joining the SBRN, seeming to be similar to our case [7]; however, they provided no anatomical description of the origin and course of the accessory branch.
There are quite a lot of variations of the SBRN described in papers and textbooks. These variations include its absence [1, 3], an aberrant course running superficially to the BM [9] or between the split tendons of the BM [10, 12], and its duplications [7]. However, to our knowledge, duplication of the SBRN coexisting with any variation of the BM directly related to the nerve has not been reported.
An accessory BM, accessory long supinator muscle, and brachioradialis brevis muscle inserting onto the radial tuberosity or even onto the ulna have been described [3, 5, 9]. The tendon of the BM is split in about 7 % of cases [3]. Cases of double BM and complete absence of the BM have also been reported [3]. The BM may originate as proximal as the deltoid tuberosity of the humerus and may insert into the supinator, the tendon of the pronator teres, or the radial aspect of the shaft of the ulna [3, 9]. Divided and supernumerary bellies of the BM have also been described; see Gruber and Turkof et al. for a large overview [5, 10]. Gruber summarized different cases and types of the BM variations and reported himself on some new cases. He was first to mention the two-bellied brachioradialis muscle, but his four cases are different from our one, as they insert on the radial tuberosity [5]. The BM may be coalesced or tethered to the brachialis muscle, extensor carpi radialis muscle, pronator teres muscle, or flexor carpi radialis muscle. It may also be inserted far more proximal than the suprastyloid crest of the radius. Rarely, it is innervated by the musculocutaneous nerve [4]. To our knowledge, a coincidence of the ASBRN and a double-bellied BM with three above-discussed potential sites of impingement has not previously been reported, and its incidence is unclear. It seems to be a rare situation; on the contrary, it can potentially cause an unexpected impingement.
References
Appleton AB (1911) A case of abnormal distribution of the n. musculo-cutaneus, with complete absence of the ramus cutaneus n. radialis. J Anat Physiol 46(Pt1):89
Auerbach DM, Collins ED, Kunkle KL, Monsanto EH (1994) The radial sensory nerve: an anatomic study. Clin Orthop Related Res 308:241–249
Bergman RA, Afifi AK, Miyauchi R. Opus II: Cardiovascular System: Arteries: Upper Limb. In: Illustrated Encyclopedia of Human Anatomic Variation; 1992–2004. Available via DIALOG: http://www.anatomyatlases.org/AnatomicVariants/NervousSystem/Text/RadialNerve.shtml (Accessed 3 June 2016)
Doyle JR, Botte MJ (2015) Surgical Anatomy of the Hand and Upper Extremity. Wolters Kluwer Health, Philadelphia
Gruber W (1868) Über die Varietäten des Musculus brachio-radialis. Bull Acad Imp Sci Saint-Pétersbourg 12:259–269
Lanzetta M, Foucher G (1993) Entrapment of the superficial branch of the radial nerve (Wartenberg’s syndrome). Int Orthop 17(6):342–345
Murphy AD, Blair JW (2012) An anatomical variant of the superficial branch of the radial nerve in Wartenberg’s syndrome. J Hand Surg 37(4):365–366
Samarakoon LB, Lakmal KC, Thillainathan S, Bataduwaarachchi VR, Anthony DJ, Jayasekara RW (2011) Anatomical relations of the superficial sensory branches of the radial nerve: a cadaveric study with clinical implications. Patient Saf Surg 5(1):1
Spinner RJ, Spinner M (1996) Superficial radial nerve compression at the elbow due to an accessory brachioradialis muscle: a case report. J Hand Surg 21(3):369–372
Turkof E, Puig S, Choi MSS, Schilhan R, Millesi H, Firbas W (1994) Superficial branch of the radial nerve emerging between two slips of a split brachioradialis muscle tendon: a variation of possible clinical relevance. Acta Anat 150:232–236
Turkof E, Puig S, Choi MSS, Zöch G, Dellon AL (1995) The radial sensory nerve entrapped between the two slips of a split brachioradialis tendon: a rare aspect of Wartenberg’s syndrome. J Hand Surg 20(4):676–678
Wood J (1867) Variations in human myology observed during the winter session of 1866-67 at King’s College London. Proc R Soc Lond 160:518–531
Acknowledgments
The authors kindly thank all the body donors for their gift to research. The authors sincerely thank Mirka Plecitá for bibliographic support. This research complies with the law of Czech Republic, where it was performed. This study was supported by the Charles University Project PRVOUK # 33.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest and no financial interests.
Rights and permissions
About this article

Cite this article
Herma, T., Baca, V., Yershov, D. et al. A case of a duplicated superficial branch of radial nerve and a two-bellied brachioradialis muscle presenting a potential entrapment syndrome. Surg Radiol Anat 39, 451–454 (2017). https://doi.org/10.1007/s00276-016-1732-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-016-1732-8