
Abstract
Objective
Tarsal coalitions are common in the middle talocalcaneal joints and prognosis of intracapsular fractures in the region is bad. So this study was done to know the size, shape and number of talar articular facets and the distance between the two anterior facets.
Materials and methods
A total of 300 (154 right and146 left) dry human calcanei of unknown sex were studied. The articular facets were marked with marker pen; the distance between the smaller anterior and middle facets was measured using a vernier calipers and they are classified into four types.
Results
After classification of the calcanei, we found that Type-1 was 67%, Type-2 was 28.66%, Type-3 was 3%, and Type-4 was 1.33%.
Conclusion
In our study, Type-1 was common followed by Type-2. Race appears to play a part in the determination of the type of facets and hence this study will be useful for the orthopedics surgeons during various surgical procedures.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The calcaneus is the longest and largest of the tarsal bones. It articulates with the overlying talus to form the talocalcaneal joint which together with the talocalcaneo-navicular joint are clinically referred to as the subtalar joint where the important movements of inversion and eversion of the foot occur. The middle third of the superior surface of the calcaneus carries the posterior talar facet for articulation with the body of the talus. In the anterior third of the calcaneus, distal and medial to the sulcus calcanei, an articular area covers the sustentaculum tali. This facet articulates with the head of the talus, and may be divided in about half the cases by a non-articular zone creating middle and anterior talar facets the incidence of which varies with race and sex [17]. This morphological variability of the facets could result from differences in the gait or other habits influencing these articular areas or it could be indicative of genetically determined variations.
The morphology of the articular facets of the calcaneus has been a subject of interest to anatomists. The articular facets of the sustentaculam tali have a variety of configurations and are functionally important because they influence subtalar joint stability [5].
In various diseases of foot, such as the talocalcaneal arthritis and coalition, intraarticular fractures and congenital dysmorphology, flatfoot, valgus deformities, the size and shape of the bones, the relationships of the talus and calcaneus with each other and other bones of the foot must be considered for the internal and external fixation and surgical procedure [19].
Materials and methods
The study was done on 300 normal adult human dry calcanei of unknown sex of which 154 were of right side and 146 were of left. The numbering of bones was done on the superior surface posteriorly. Each bone was marked with a marker pen by outlining the superior articular facets. A tracer paper was placed over the facets and was traced such that the topography of the facets and the distance between all the facets were maintained. From the tracer paper, facets were copied onto a white sheet using a carbon paper. All bones were classified into four groups based on the number of talar articular facets present on each calcaneus:
Type 1 Two articular facets present with anterior one either constricted or non-constricted. This was further subdivided into:
1a: If the anterior facet was non-constricted.
1b: If the anterior facet was constricted
Type 2 Three articular facets present, the distance between anterior and middle facet was measured with help of vernier calipers. This was further subdivided into:
2a: If the distance was <2 mm.
2b: If the distance was between 2 and 5 mm.
2c: If the distance was >5 mm and the size of the anterior facet was large.
2d: If the distance was more than 5 mm but the size of the anterior facet was quite small.
Type 3 Two articular facets present with anterior one restricted to sustentaculum tali
Type 4 One facet
Results
The facets on the superior surface of the calcaneus were classified into four types:
Type-1 had two facets (67%).
Type 1a was seen in 16.6% of cases (Fig. 1).

Showing two facets on the calcaneum. Type 1a The anterior facet was non-constricted. Type 1b The anterior facet was constricted
Type 1b was seen in 50.3% of cases (Fig. 1).
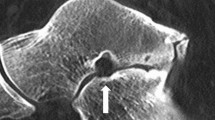
Type-2 had three facets (28.6%). Two facets were for the head of the talus, anterior and middle. However, the distance between these two facets was variable. It was measured and sub classified into four groups as below.
Type 2a was seen in 5.3% of cases (Fig. 2).

Showing three facets. Two facets were for the head of the talus, anterior and middle. Type 2a The distance between these 2 facets was <2 mm. Type 2b The distance between these two facets was between 2 and 5 mm. Type 2c The distance between these two facets was more than 5 mm but the anterior facet was large. Type 2d The distance between these two facets was more than 5 mm but the anterior facet was small
Type 2b was seen in 13.6% of cases (Fig. 2).
Type 2c was seen in 7.3% of cases (Fig. 2).
Type 2d was seen in 2.3% of cases (Fig. 2).
Type-3 (3%) had two facets but the anterior one was on the sustentaculum tali (Fig. 3).

Showing two facets but the anterior one was on the sustentaculum tali Type-3
Type-4 (1.3%) had a single fused facet (Fig. 4).

Showing single fused facet Type-4
Discussion
The number and arrangement of the articular facets on the superior surface of the calcaneus designated to carry the head of the talus have been described variously by different authors (Table 1). The result of our study was consistent with the studies done previously. For all studies, the first two types type 1 (201), type 2 (86) constitute the two most common varieties of facets for the articulation with the talus. The facets on the sustentaculum tali may be of equal sizes but if the anterior facet is very small, it can be totally overlooked.
The embryology of subtalar joint is very important for the facets to be formed on calcaneum for the talus. The first constitutive features of the subtalar joint start to clarify from the eighth week. At this stage, the talus and calcaneus look as cartilaginous precursors separated by mesenchymal tissue whose cells are rounded, packed and not yet positioned. At the ninth week, cavitation of the subtalar joint occurs with rarefaction of the mesenchymal cells at the forthcoming articular surfaces but does not include the entire joint equally. The cavitation of the posterior aspect of the joint proceeds more rapidly than at the anterior aspect. At the 10th week, the posterior surface of the subtalar joint is well formed. The anterior and medial articular surfaces of the subtalar joint seem more developed. At the 11th week, the cavitational process of the subtalar joint is shown to be developing differently in three regions, anterior, middle, and posterior. The articular surfaces are easily obvious at this time. At the 14th week, all the articular and capsulo-ligamentous structures of the subtalar joint and the sinus tarsi are clearly obvious. The anterior and posterior subtalar joints, well cavitated, have their proper articular capsule and a distinct sinus tarsi and tarsal canal where the extensor retinaculum, the cervical ligament and the interosseous ligament can be observed [15].
Shahabpour et al. have done a MRI study to look for variations of the subtalar and talocalcaneonavicular joints. They found that 18 (36.7%) of the subjects had 3 distinct facets on the calcaneus which in our study we found in 28.6% of cases [18].
Bunning and Barnett [1] reported that the incidence of Type 1 is significantly higher than Type 2 in both Sudanese & Indian series1. El-Eishi found Type-3 to a greater extent in Egyptians, which suggests that the facets are genetically determined as mentioned by Bunning and Barnett [2, 6]. Type-4 facet is common in Nigerians and Veddah but in a very small sample. Type-4 may, therefore perhaps be used as a ethnical characteristic [3].
In all the Indian studies done including the present one, Type-1 facets occurred in 62–67% of calcanei. In western studies also 60-70% of the calcanei showed the occurrence of Type-1 facets. In Egyptians and Spanish, Type-1 facets are found in only 50% of the calcanei, whereas, only about 30% of the European calcanei show this facet.
In Indians and most of western population percentage of Type-2 facets is just about half of the Type-1 facets. On the other hand, in Egyptians and the Spanish, the occurrence of Type-1 and 2 facets is approximately same, while in Europeans, Type-2 facets are almost twice as common as Type-1 facets. This appears to be an interesting ethnic characteristic. Many such factors as wearing of shoes, squatting habits, genetic and ethnic differences are the probable reasons for the variations in the facets on the calcanei in the western and Indian series.
The distance between anterior and middle facet is important for evan’s osteotomy. This technique is used for correction of pes plano valgus deformity and stage 2 posterior tibial tendon dysfunction, particularly when the apex of deformity is in the transverse plane. In lengthening the lateral column, talar head coverage by the navicular increases, forefoot abduction and hindfoot valgus decrease, and there is an increase in the height of the longitudinal arch. The osteotomy courses from lateral to medial in the calcaneal anterior process 1.5 cm proximal to the calcaneocuboid joint that crosses medially between the anterior and middle subtalar facets. A tricortical bone graft is used to lengthen the lateral column. So, we have divided the type 2 classifications in further subgroups to measure the distance between both of them [8].
An accessory anterolateral talar facet was found in 34% of the specimens in a pediatric osteologic group. The facet was associated with male sex, a reduced angle of Gissane, and dorsal talar beaking which we did not found in the present study [11].
Disposition of superior articular facets of the calcaneum is congenital and not a postnatal development with Type-1 more in females-sexual dimorphism [1]. Tarsal coalitions are inherited most probably as a unifactorial disorder of autosomal dominant inheritance with full penetrance [9]. They occur in association with carpal coalitions, phocomelia, hemimelia [12]. 83% are talocalcaneal leading to tarsal tunnel syndrome, osteophyte causing sensory disturbance in the region of medial plantar nerve and restriction of plantar flexion at the ankle joint [13]. Calcaneal fractures account for 33.3% of foot fractures. And it was seen that there was 100% involvement of posterior talocalcaneal facet in intra-articular calcaneal fractures [16].
In Indian populations where walking is mainly barefoot or in sandals so that the subtalar joint is more exposed to the stresses that may be produced by walking unprotected by shoes the anatomy of these articular facets is important and may also have a role in planning foot surgery [10].
References
Bunning PSC, Barnett CH (1963) Variations in the talocalcaneal articulations. J Anat 97:643
Bunning PS, Barnett CH (1965) A comparison of adult and foetal talocalcaneal articulations. J Anat 99:71–76
Bunning PSC (1964) Some observations on the West African calcaneus and the associated talocalcaneal interosseous ligamentous apparatus. Am J Phys Anthropol 22:467–472
Campos FF, Pellico LG (1989) Talar articular facets (facies articulares talares) in human calcanei. Acta Anat 134:124–127
Drayer-Verhagen F (1993) Arthritis of the subtalar joint associated with sustentaculum tali facet configuration. J Anat 183:631–634
El-Eishi H (1974) Variations in talar articular facets in Egyptian Calcanei. Acta Anat 89:134–138
Gupta SC, Gupta CD, Arora AK (1977) Pattern of talar articular facets in Indian Calcanei. J Anat 124:651–655
Hyer CF, Lee T, Block AJ, Van Court R (2002) Evaluation of the anterior and middle talocalcaneal articular facets and the evans osteotomy. J Foot Ankle Surg 41(6):389–393
Leonard MA (1974) The inheritance of tarsal coalition and its relationship to spastic flat foot. J Bone Joint Surg 56b:520–526
Madhavi C, Madhuri V, George VM, Antonisamy B (2008) South Indian calcaneal talar facet configurations and osteoarthritic changes. Clin Anat 21:581–586
Martus JE, Femino JE, Caird MS, Hughes RE, Browne RH, Farley FA (2008) Accessory anterolateral facet of the paediatric talus. An anatomic study. J Bone Joint Surg 90(11):2452–2459
Mosier KM, Asher M (1984) Tarsal coalitions and peroneal spastic flatfoot. J Bone Joint Surg 66-A(7):976–984
Olney BW, Asher MA (1987) Excision of symptomatic coalition of middle facet of the talocalcaneal joint. J Bone Joint Surg 69-A:539–544
Padmanabhan R (1986) The talar facets of the calcaneus—an anatomical note. Anat Anz 161(5):389–392
de Palma L, Santucci A, Ventura A, Marinelli M (2003) Anatomy and embryology of the talocalcaneal joint. Foot Ankle Surg 9(1):7–18
Rosenberg Zs, Feldman F, Singson RD (1987) Intra-articular calcaneal fractures: computed tomographic analysis. Skelet Radiol 16(2):105–113
Saadeh FA, Fuad AH, Mahmoud SMI, Marwan EE (2000) Patterns of talar articular facets of Egyptian calcanei. J Anat Soc India 49:6–8
Shahabpour M, Devillé A, Van Roy P, Vaes P, De Mey J, De Maeseneer M (2011) Magnetic resonance imaging of anatomical variants of the subtalar joint. Surg Radiol Anat 33(7):623–630
Uygur M, Atamaz F, Celik S, Pinar Y (2009) The types of talar articular facets and morphometric measurements of the human calcaneus bone on Turkish race. Arch Orthop Trauma Surg 129(7):909–914
Conflict of interest
We declare that we have no conflicts of interest. There is no financial help from the organizing research committee.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sharada, R., Sneha, K., Gupta, C. et al. Non-metrical study of the pattern of talar articular facets in south Indian dry calcanei. Surg Radiol Anat 34, 487–491 (2012). https://doi.org/10.1007/s00276-012-0939-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-012-0939-6