
Abstract
The anterior portion of the calcaneus is not explicitly described as a bony landmark in contemporary textbooks of human anatomy. However, it may be involved in all types of fractures of the largest tarsal bone. Both surgeons and radiologists are aware of the anterolateral extension of traumatic lesions of the calcaneus. Thus, the anterior portion of the bone should be referred to uniformly as the processus anterior calcanei.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The normal and pathological anatomy of the calcaneus is clearly demonstrated by imaging procedures. If performed skillfully and interpreted meticulously, conventional radiography provides a wealth of data for diagnosis and treatment of the various lesions of the largest tarsal bone. The degree of post-traumatic comminution and extent of articular bursting can be adequately assessed, as a rule. However, computed tomography (CT) improves the understanding of the shape and position of the components of the calcaneus, produces detailed images of the intra- and extra-articular fracture anatomy and refines classification and subclassification of the sequelae of injuries which have potential prognostic value.
The advent of CT prompted authors to pay closer attention to the anatomy of the projections of the bone. Whereas Palmer [21] and Essex-Lopresti [2] divided intra-articular fractures of the calcaneus into two distinct types (tongue type and joint depression type, respectively) without subtle description of the parts and articular facets of the bone involved, the new classification systems are explicitly related to these features. According to Sanders et al. [26, 27, 28], five major fragments—sustentacular fragment, tuberosity fragment, subtalar joint fragment, anterior process fragment, anterior subtalar joint fragment—and four joints frequently affected—posterior subtalar joint, calcaneocuboid joint, middle and anterior facets of the anterior subtalar joint—are differentiated. Obviously, the anterior portion of the calcaneus and the calcaneocuboid joint are related to each other. But whereas the calcaneocuboid surface (facies articularis cuboidea) is a common anatomical term, the anterior process of the calcaneus is not particularly designated in most contemporary textbooks of normal human anatomy.
Neither the standard English [4, 13, 37] nor the equivalent French and German reference books [11, 22] describe it as a separate morphological entity. There are few exceptions to this rule. In Quain’s Elements of Anatomy [31] the term “anterior extremity” is found. Hovelacque [7] and Testut and Latarjet [32] keep the anterior process distinct from the main mass of the bone and call it the “great apophysis” (“grande apophyse”). Similarly, Okajima [20] seems to interpret the anterior process as a projection of the calcaneus, but without giving it a particular name. Neither the Nomina Anatomica [19] nor the Terminologia Anatomica [35] specifies the anterior portion of the bone. Some direct remarks can only be found in textbooks of the nineteenth century [5, 14].
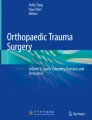
Anatomists describe three processes originating from the calcaneus [37]: the shelf-like sustentaculum tali (sustentaculum tali), the great tuberosity (tuber calcanei) and the small fibular trochlea (trochlea fibularis). The upper surface of the sustentaculum tali and the adjacent part of the body bear the anterior and middle articular surfaces for the talus. The tuberosity itself has two processes: the medial one which affords attachment to abductor hallucis and the superficial part of the retinaculum flexorum, and the lateral one which the abductor digiti minimi is attached to. Above and in front of the fibular trochlea the peroneus brevis tendon runs forwards; below and behind it the peroneus longus tendon passes downwards and forwards. Conversely, the anterior portion of the bone whose anterior surface is covered by the articular facet for the cuboid and which ligaments and muscles are attached to, is not taken as a volume element (Fig. 1).

Schematic diagram of the tarsal bones with the anterior process of the calcaneus highlighted. 1, Cuboid; 2, navicular; 3, trochlea of talus; 4, calcaneal tuberosity
The same is true for the veterinary anatomical nomenclature [8]. As comparative anatomy shows, the position of the anterior portion of the calcaneus reflects evolutionary emergence and refinement of the mammalian pattern of foot architecture [3, 12]. In living primates, except the great apes and humans, the foot is placed in a heel-elevated position when these animals move upon arboreal or terrestrial surfaces. Heel placement and bone positions are designed to increase mobility and flexibility. Orang-utans have further enhanced their ability to move by adapting their feet for suspension and thus similarly utilize foot positions where the heel does not touch the ground. Chimpanzees and gorillas represent an alternative pattern, in which the heel contacts the surface of the support at the end of the swing phase. Thus, African apes possess feet adapted for both arboreal and terrestrial terrains and also share several skeletal features with early hominids.
Embryologically, the anterior portion of the calcaneus is enchondral in origin and belongs to the central part of the bone. Ossification of the calcaneus usually originates from two independent and developmentally different centers [17]. The first one, parachondral in origin and laterally positioned, becomes visible in the fourth or fifth fetal month and resembles to the later trochlea fibularis. The second one is situated in the anterior third of the cartilaginous calcaneus in relation to the sustentaculum tali medially and to a cartilaginous prominence on its lateral circumference, respectively. It appears in the sixth or seventh fetal month. The two ossification centers usually fuse around birth. In mammals, the anterior edge of the calcaneus is elongated in the form of a more or less trigonal nose which corresponds to a notch in the talus and is named the processus coracoideus.
The anterior portion of the calcaneus takes up the anterior third of the bone and is clearly distinguished by its lower height compared with the posterior portion. In newborns and babies, it is still about half as long as the whole heel bone. The forward edges are sharply defined and serve for the attachment of the bifurcate and dorsal calcaneocuboid ligaments. The superior surface makes up the floor of the sinus tarsi. Medially, it is limited by the lateral edge of the sulcus calcanei. From a beak-like protuberance at its lateral aspect the extensores hallucis brevis and digitorum brevis arise. At the bottom surface, the tuberculum calcanei delimits the border to the central portion of the bone. The axial calcaneocuboid angle, i.e., the angle in the axial plane between the longitudinal axis of the calcaneus and a line drawn perpendicular to the calcaneocuboid joint, measures 25.3±7.3º in normal feet [24]. The most common variant of the anterior portion of the calcaneus is an accessory ossicle at its anterior facet (the so-called calcaneus secundarius) [15]. Oblique views at different angles must be made in order to separate the shadow of the anterior portion of the calcaneus from that of the front and bottom of the talus in conventional radiography (Fig. 2).

Anterior process of the calcaneus (borders marked by arrowheads) on a lateral radiograph of a talipes cavus (Friedreich’s foot)
In traumatic lesions of the calcaneus, the primary fracture line splits the posterior facet of the subtalar joint from posterolateral to anteromedial, thus dividing the bone in a roughly vertical direction, and in propagating forwards often involving the anterior portion [6, 16, 23, 25, 33]. Miric and Patterson observed extension of the fracture into the calcaneocuboid joint in 67 of 120 (58%) traumatic lesions as assessed by CT [18]. Involvement of the calcaneocuboid joint was distributed evenly among the four fracture types according to the classification of Sanders et al. The more pronounced the lateral subluxation of the posterior facet fragment or the comminution of the lateral wall of the calcaneus is, the more likely the cuboid articular facet is involved [1]. The secondary fracture line extends laterally just anterior to the posterior subtalar joint passing to the lateral wall of the calcaneus in the vicinity of the peroneal tubercle and does not reach the anterolateral extension of the bone [2].
Due to the lack of an official anatomical term, the orthopedic, surgical and radiological literature defines the anterior portion of the calcaneus differently. Johnson and Gebhardt [9] take the anterior portion as part of the body of the calcaneus and refer to it consequently as the anterior body (and its fractures). In a review on the use of axial CT in intra-articular fractures, Kerr et al. [10] call it the anterior calcaneus. To classify fracture specimens, Wülker et al. [38] divide the calcaneus into four segments, one of which is explicitly named “the anterior process”. Thus, surgeons are obviously aware of the anatomical and clinical importance of the anterior portion of the bone (Fig. 3).

Axial CT scans (slice thickness: 4 mm) of the tarsus. In the larger image, the intact anterior process of the calcaneus is depicted as sharply demarcated from the middle portion of the bone. The smaller image displays a bursting fracture of the anterior process with the calcaneocuboid articulation intact
Still more precise and consistent are the radiological comments on this region. In a review of their personal experience with CT in fractures of the calcaneus, Sbragia et al. [30] report two cases of cuboid bone impaction into “the anterior process” of the calcaneus. Wechsler et al. [34] speak about “the anterior process of the calcaneus which articulates with the cuboid and is contiguous with the posterior portion, the tuberosity”. In an accompanying schematic drawing, the abbreviation “AP” for “anterior process” is introduced without further explanation or justification. Finally, in a recent review Sanders [29] declares that the (secondary) fracture line can exit as far forward as “the anterior process” or the calcaneocuboid joint, thus creating an anterolateral fragment.
In conclusion, the anterior portion of the calcaneus is a distinct, well recognized and clinically important part of the largest tarsal bone that should be referred to uniformly as the anterior process (processus anterior) of the calcaneus in anatomical textbooks and papers. The new term accommodates the needs of both clinicians and scientists and will help the Federative Committee on Anatomical Terminology (FCAT) to make the terminology an internationally accepted living language of anatomy [36].
References
Ebraheim NA, Biyani A, Padanilam T, Christiensen G (1996) Calcaneo-cuboid joint involvement in calcaneal fractures. Foot Ankle 17:563–565
Essex-Lopresti P (1952) The mechanism, reduction technique, and results in fractures of the os calcis. Br J Surg 39:395–419
Gebo DL (1992) Plantigrady and foot adaptation in African apes: implications for hominid origins. Am J Phys Anthropol 89:29–58
Grant JCB (1956) An atlas of anatomy. Williams & Wilkins, Baltimore
Henle J (18713) Handbuch der Knochenlehre des Menschen. F Vieweg & Sohn, Braunschweig, p 295
Hodge JC (1999) Anterior process fracture or calcaneus secundarius: a case report. J Emerg Med 17:305–309
Hovelacque A (1933) Ostéologie, part 1. G. Doin & Cie, Paris, p 205
International Committee on Veterinary Anatomical Nomenclature (1973). Nomina Anatomica Veterinaria. Adolf Holzhausen Successors, Vienna, p 25
Johnson EE, Gebhardt JS (1993) Surgical management of calcaneal fractures using bilateral incisions and minimal internal fixation. Clin Orthop 290:117–124
Kerr PS, James A, Cole AS, Atkins RM (1994) The use of the axial CT scan in intra-articular fractures of the calcaneum. Injury 25:359–363
Leonhardt H, Tillmann B, Töndury G, Zilles K (1987) Rauber/Kopsch: Anatomie des Menschen. Lehrbuch und Atlas. Thieme, Stuttgart
Lewis OJ (1983) The evolutionary emergence and refinement of the mammalian pattern of foot architecture. J Anat 137:21–45
Lockhart RD, Hamilton GF, Fyfe FW (1960) Anatomy of the human body. Lippincott, Philadelphia
Luschka H von (1865) Die Anatomie der Glieder des Menschen. Verlag der H. Laupp‘schen Buchhandlung, Tübingen, p 351
Mann RW (1989) Calcaneus secundarius. Variation of a common accessory ossicle. J Am Podiatr Assoc 79:363–366
Marcinko DE, Field N (1988) Fractured anterior calcaneal process. J Foot Surg 27:43–46
Meyer DB, O‘Rahilly R (1976) The onset of ossification in the human calcaneus. Anat Embryol (Berl) 22:19–33
Miric A, Patterson M (1998) Pathoanatomy of intra-articular fractures of the calcaneus. J Bone Joint Surg Am 80:207–212
International Anatomical Nomenclature Committee (1989) Nomina Anatomica, 6th edn. Williams & Wilkins, Baltimore
Okajima K (1933) Anatomie, vol I: Einleitung, Knochen, Bänder, Muskel-, Eingeweidelehre und Lehre der inkretorischen Organe. Tohodo, Tokyo, pp 146–147
Palmer I (1948) The mechanism and treatment of fractures of the calcaneus. Open reduction with the use of cancellous grafts. J Bone Joint Surg Am 30:2–8
Poirier P, Charpy A, Nicolas A (1926) Traité d’anatomie humaine, vol I, part 2. Masson, Paris, pp 313–316
Renfrew DL, El-Khoury GY (1985) Anterior process fractures of the calcaneus. Skeletal Radiol 14:121–125
Richardson ML, Van Vu M, Vincent LM, Sangeorzan BJ, Benirschke SK (1992) CT measurement of the calcaneal varus angle in the normal and fractured hindfoot. J Comput Assist Tomogr 16:261–264
Roesen HM, Kanat IO (1993) Anterior process fractures of the calcaneus. J Foot Ankle Surg 32:424–429
Sanders R, Hansen ST Jr, McReynolds IS (1991) Trauma to the calcaneus and its tendon. In: Jahss MD (ed) Disorders of the foot and ankle: medical and surgical treatment, 2nd edn, vol 3. WB Saunders, Philadelphia, pp 2326–2354
Sanders R (1992) Intra-articular fractures of the calcaneus: present state of the art. J Orthop Trauma 6:252–265
Sanders R, Fortin P, DiPasquale T, Walling A (1993) Operative treatment in 120 displaced intraarticular calcaneal fractures. Results using a prognostic computed tomographic scan classification. Clin Orthop 290:87–95
Sanders R (2000) Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 82:225–250
Sbragia P, Zanfranceschi G, Niccolai F, Piperno G (1991) Le fratture del calcagno: aspetti TC. Radiol Med (Torino) 82:265–269
Sharpey W, Thomson A, Schäfer EA (1876) Quain’s elements of anatomy, vol I. Longman, Green & Co, London, p 114
Testut L, Latarjet A (19489) Traité d’anatomie humaine, vol 1: Ostéologie arthrologie myologie. G Doin & Cie, Paris, p 429
Thorén O (1964) Os calcis fractures. Acta Orthop Scand Suppl 70:1-116
Wechsler RJ, Schweitzer ME, Karasick D, Deely DM, Morrison W (1998) Helical CT of calcaneal fractures: technique and imaging features. Skeletal Radiol 27:1-6
Whitmore I (1998) Terminologia Anatomica—International Anatomical Terminology. Federative Committee on Anatomical Terminology (FCAT). Thieme, Stuttgart
Whitmore I (1999) Terminologia anatomica: new terminology for the new anatomist. Anat Rec 257:50–53
Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, Ferguson MWJ (1995) Gray‘s anatomy. The anatomical basis of medicine and surgery, 38th edn. Churchill Livingstone, New York
Wülker N, Zwipp H, Tscherne H (1991) Experimentelle Untersuchung zur Klassifikation von intraartikulären Fersenbeinfrakturen. Unfallchirurgie 94:198–203
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Golder, W.A. Anterior process of the calcaneus: a clinical-radiological contribution to anatomical vocabulary. Surg Radiol Anat 26, 163–166 (2004). https://doi.org/10.1007/s00276-003-0220-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-003-0220-0