
Abstract
The scaphoid cortical ring sign (CRS) has been identified as a radiological indicator of ligamentous injury of the wrist. It has been associated with some pathokinematic states. There exists a range of wrist positions where the CRS may be normally present. The purpose of this study was to define the range of motion when the CRS can normally be observed on a standard posteroanterior radiograph and, in turn, to define the range where the CRS is not expected to be present. One hundred and nine posteroanterior radiographs of normal wrists were evaluated for the presence, partial presence and absence of the scaphoid CRS. The results were correlated with the radio-metacarpal (RM) angle in neutral palmar-dorsiflexion of the wrist. The range of wrist deviation for the wrists studied was −10.0° (radial deviation) to 23.0° (ulnar deviation). We defined the normal (and abnormal) range as being two standard deviations from the mean. The CRS was present in 25% of the radiographs evaluated. Moreover, the CRS was found to be present at 2.7° (±7.7°) of radial deviation with a calculated range of -18.1° to 12.7°. The CRS was absent at 12.4° (±11.7°) of ulnar deviation. It is concluded that the CRS observed at values less than 13° of ulnar deviation may or may not be abnormal. If the CRS is observed at a RM angle of 13° of ulnar deviation or greater, it should be considered pathological. The CRS, however, should be used in conjunction with other clinical findings of carpal instability.
Résumé
Le signe de l'anneau cortical du scaphoïde (SACS) est classiquement considéré comme un indicateur radiographique de lésion ligamentaire du poignet, qui peut s'observer dans plusieurs situations pathologiques. A l'inverse, il peut aussi être rencontré sur un poignet normal, en fonction de la position de celui-ci. Le but de cette étude était de définir les positions du poignet pour lesquelles ce signe peut être normalement observé, et à l'inverse non observé, sur une radiographie en incidence postéro-antérieure. Sur 109 clichés standard de poignets normaux, la présence, la présence partielle ou l'absence de ce signe a été déterminée. Ces résultats ont ensuite été confrontés au degré d'inclinaison radio-ulnaire, mesurée par l'angle radio-métacarpien, le poignet étant en flexion (dorso-palmaire) neutre. Les limites des valeurs normales ont été définies par un écart de deux déviations standard par rapport à la moyenne. Le SACS a été retrouvé dans 25% des cas. Il était observé lorsqu'il existait une inclinaison radiale moyenne de 2,7°±7,7° (valeurs extrêmes: 18,1°–12,7°). Il était absent en cas d'inclinaison ulnaire moyenne de 12,4° (±11,7°). Le signe de l'anneau cortical du scaphoïde observé pour une inclinaison ulnaire inférieure à 13° n'a pas de signification pathologique formelle. En revanche, pour une inclinaison ulnaire de 13° ou plus, il doit être considéré comme anormal. Ce signe doit toujours être interprété en tenant compte des signes cliniques d'instabilité du carpe.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The cortical ring sign (CRS) is an "end-on" view of the proximal and distal poles of the scaphoid [1, 5]. The CRS was at one time described as pathognomonic for "rotational dislocation" of the scaphoid [5] and is still considered an essential radiographic feature of rotary subluxation of the scaphoid [8]. The CRS is normally present when the wrist is in radial deviation [1, 8]. However, Cautilli and Wehbe [3] reviewed 100 normal wrist radiographs in neutral deviation and did not find the CRS present [3]. The CRS, however, was not correlated with the degree of radial-ulnar deviation of the wrist [3]. Since the CRS can be associated with carpal instability and can also be seen in normal wrists, radiographs without wrist pathology were collected, to determine the frequency of the CRS. The radiographs studied displayed a range of angles of wrist deviation. This information was used to determine the range where a CRS can occur in the normal wrist, where a partial CRS can be noted and where a CRS should not be observed. With this information, clinicians can determine when the presence of the CRS is supportive for carpal instability.
Materials and methods
One hundred and nine high-quality posteroanterior (PA) wrist and forearm radiographs of patients without wrist pathology were collected on 78 subjects. The radiographs were performed for screening purposes for unrelated complaints such as carpal tunnel syndrome, trigger finger, fifth metacarpal and phalangeal fractures. Fractures of the distal radius and the first through fourth metacarpals were excluded. The ages of the subjects ranged from 15 to 77 years with a mean age of 43 years. Sixty-two radiographs were of the right wrist and 47 were of the left. Forty-three of the subjects were male, 35 were female. The hand-wrist-distal forearm radiographs were performed in the posteroanterior plane. The wrist was maintained in neutral flexion with the hand resting on the cassette, the elbow was flexed to 90° and the arm was adducted (neutral abduction). Presence of the CRS was defined as a completely enclosed circle (ring) (Fig. 1A). Partial presence entailed any portion of the ring (Fig. 1B) and absence was reserved for radiographs with no portion of the CRS (Fig. 1C). Measurements of the radio-metacarpal angle (RM) were made using the longitudinal axis of the third metacarpal and the longitudinal axis of the radius in the PA plane (Fig. 2). All three authors performed the radiological measurements. Wrists with radial deviation were recorded as negative angles and those with ulnar deviation as positive angles. Furthermore, the presence, partial presence or absence of the CRS was determined for each of the radiographs studied. The mean angle and range of wrist deviation were determined for the presence, partial presence, and absence of the CRS.

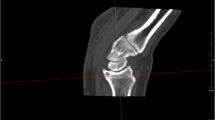
View of normal wrist radiograph with an absent cortical ring sign. B View of a normal wrist with a partial cortical ring sign. C View of a normal wrist with a typical cortical ring sign

Measurement of the radio-metacarpal angle (RM), which represents wrist deviation
Results
Twenty-seven (25%) of the 109 radiographs demonstrated a CRS. The wrist deviation for the study group ranged from −23° (radial deviation) to 40° (ulnar deviation). The RM angle was used to measure the wrist deviation. The CRS was found to be present at 2.7° (±7.7°) of radial deviation with an actual range of −23° to 10°. A partial sign was noted at 5.7° (±9.8°) of ulnar deviation with an actual range of −12° to 25°. However, the CRS was absent at 12.4° (±11.7°) of ulnar deviation with an actual range of −5° to 43°.
Using two standard deviations as the limits of normal, the calculated expected range for the CRS is 18.1° of radial deviation to 12.7° of ulnar deviation. In essence, using this information, the CRS should not be present at 13.0° or greater of ulnar deviation (Figs. 3, 4). A partial sign can be expected at 13.9° of radial deviation to 25.3° of ulnar deviation. Lastly, absence of the CRS can be expected from 16.7° of radial deviation to 35.8° of ulnar deviation. The data clearly demonstrate overlap of each finding. The results are summarized in Table 1 and Fig. 5.

Distribution of the cortical ring sign by percentage at varying degrees of wrist deviation

Number of radiographs (subjects) evaluated and their corresponding wrist position

Absolute wrist deviation range for presence, partial presence and absence of the cortical ring sign
Discussion
Ligamentous and bony injuries to the wrist can be devastating to the function of the hand. These injuries are typically caused by a fall on an outstretched hand with the wrist in an ulnarly deviated and hyperextended position [8]. The intrinsic ligaments of the scapholunate joint are typically damaged [8]. The result of this damage is termed scapholunate dissociation, which is essentially an uncoupling of the scaphoid from the lunate [8]. This uncoupling results in rotary subluxation of the scaphoid, where the proximal pole of the scaphoid subluxes over the dorsal lip of the distal radius causing pain and clicking with radial deviation [4, 8]. If scapholunate dissociation is not treated, the pathokinematic motion leads to degenerative arthritis of the radioscaphoid and scaphocapitate joints, and migration of the capitate proximally between the lunate and scaphoid. This post-traumatic process is termed scapholunate advanced collapse or SLAC wrist. The CRS may be present in advanced stages of the SLAC wrist. The associated palmar flexion of the scaphoid causes a reciprocal extension of the lunate and a dorsal intercalated segmental instability (DISI) collapse pattern of the wrist [4, 8].
Radiographic findings are helpful but often are normal for rupture of the scapholunate interosseous ligament (SLIL) in the early stages. Thompson et al. and Linscheid et al. separately described radiographic features of rotary subluxation of the scaphoid. These are decreased height of the scaphoid on the anteroposterior radiograph, increased space between the scaphoid and lunate, increased horizontal positioning of the scaphoid's long axis on a lateral view, and a ring apparent over the distal scaphoid pole or a "cortical ring sign" [6, 7]. Some have stated that this ring sign is pathognomonic of scapholunate dissociation [3, 5]. Studies of the normal kinematics of the scaphoid, however, show that with flexion or radial deviation of the wrist the scaphoid also volar flexes as it would in scapholunate dissociation [10]. This scaphoid flexion in turn can also cause the appearance of a CRS on a normal radiograph [10].
Because the CRS is considered a radiological indicator of carpal instability and can also be present in normal wrist radiographs, it is essential to determine the parameters within which the CRS can be observed. Our study demonstrates that the CRS is found relatively frequently in the normal wrist. It is therefore imperative that the clinician be cognizant of the positions where the CRS is normally observed and when it is associated with pathokinematic motion of the wrist.
Conclusion
The CRS should be considered pathological if it is found at 13° of ulnar deviation or greater. If the CRS is observed at values less than 13° of ulnar deviation, it may be normal or abnormal. However, the CRS should be used in conjunction with other clinical and radiological findings to diagnose carpal instability.
References
Belsole RJ (1986 ) Radiography of the wrist. Clin Orthop 202: 50–56
Bond JR, Berquist TH (1991) Radiologic evaluation of hand and wrist motion. Hand Clin 7: 113–123
Cautilli GP, Wehbe MA (1991) Scapho-lunate distance and cortical ring sign. J Hand Surg [Am] 16: 501–503
Cope J (1984) Rotary subluxation of the scaphoid. Clin Radiol 35: 495–501
Crittenden JJ, Jones DM, Santarelli AG (1970) Bilateral rotational dislocation of the carpal navicular. Radiology 94: 629–630
Linscheid RL, Dobyns JH, Beabout JW, Bryan RS (1972) Traumatic instability of the wrist. J Bone Joint Surg Am 54: 1612–1632
Loewen JL, Pirela-Cruz MA, Lucas GL(1998) Kinematics of the capitolunate joint in the sagittal plane: a new method based on reference points and triangulation. J Hand Surg [Br] 23: 410–412
Nathan R, Blatt G (2000) Rotary subluxation of the scaphoid—revisited. Hand Clin 16: 417–431
Oberlin C, Daunois O, Oberlin F (1990) L'arthrose scapho-trapézo-trapézoïdienne. Son retentissement sur le carpe. Ann Chir Main 9: 163–167
Thompson CT, Campbell RD, Arnold WD (1964) Primary and secondary dislocation of the scaphoid bone. J Bone Joint Surg Br 46: 73–82
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Material
Rights and permissions
About this article
Cite this article
Pirela-Cruz, M.A., Hilton, M.E. & Faillace, J. Frequency and characteristics of the scaphoid cortical ring sign. Surg Radiol Anat 25, 451–454 (2003). https://doi.org/10.1007/s00276-003-0165-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-003-0165-3