
Abstract
Pedicle screw fixation of the spine has become one of the most stable and versatile methods of spine fixation, and knowledge of pedicle morphology is crucial for the safe application of these systems. We undertook this study because only a few reports have investigated Eastern populations. Lumbar pedicle anatomy, i.e., pedicle width (PW) and pedicle height (PH), transverse and sagittal pedicle angles (TPA, SPA), and pedicle length (PL), were assessed in the following two groups: (1) computed tomography scans of 29 normal adults, and (2) 16 dried lumbar spines obtained from the Anatomy Department. Interpedicular distance was different in each group. PW ranged from 4 mm to 14 mm. In both groups, the narrowest PH was 8.2 mm, the widest 19.7 mm. TPA ranged from 6o to 19o and increased from L1 to L5. In the sagittal plane, the pedicles angled caudally at L5. PL was longest at L1 and shortest at L5. In conclusion, pedicle dimensions and angles may show individual and structural differences. Our data were not significantly different from previous reported data. A detailed knowledge of these relationships is important for any surgery involving screw purchase via a pedicle, to prevent screw cutout and failure of fixation or neurological injury. Selection of the proper diameter of screw is an important issue for safe placement. Knowledge of the pedicle axis length is essential in choosing screw lengths but should always be checked intraoperatively with fluoroscopic control during screw insertion.
Résumé
L'implantation de vis pédiculaires vertébrales est devenue une des méthodes de fixation de la colonne vertébrale les plus stables et polyvalentes. La connaissance de la morphologie pédiculaire est fondamentale pour une utilisation de ces implants en toute sécurité. Les populations orientales ont été peu étudiées, c'est pourquoi nous avons réalisé ce travail. L'anatomie du pédicule vertébral, c'est-à-dire la largeur pédiculaire (lP) et la hauteur pédiculaire (HP), l'inclinaison pédiculaire dans les plans transversal et sagittal (APT, APS), et la longueur pédiculaire (lP), a été évaluée dans les deux groupes suivants : (1) 29 examens tomodensitométriques d'adultes normaux et (2) 16 colonnes lombaires sèches appartenant à la collection du département d'anatomie. La distance interpédiculaire (DIP) était différente dans chaque groupe. La lP variait de 4 mm à 14 mm. Dans les deux groupes, la HP la plus étroite était de 8,2 mm, la plus large de 19,7 mm. L'APT variait de 6° à 19° et augmentait de L1 à L5. Dans le plan sagittal, les pédicules étaient inclinés caudalement au niveau de L5. Les LP étaient les plus élevées au niveau de L1 et les plus basses au niveau de L5. En conclusion, les dimensions et les inclinaisons pédiculaires avaient tendance à montrer des différences individuelles et structurales. Nos données ne sont pas significativement différentes des données rapportées par d'autres auteurs. Une connaissance détaillée de ces rapports est importante pour toute chirurgie proposant de choisir une vis par rapport à un pédicule, ceci dans le but de prévenir un trajet de vis extra-osseux et une défaillance de la fixation ou une lésion neurologique. La sélection du diamètre approprié de la vis est un point important pour un placement en toute sécurité. La connaissance de la longueur de l'axe pédiculaire est essentielle dans le choix des longueurs de vis, mais doit toujours être vérifié durant l'opération avec un contrôle radioscopique pendant l'insertion de la vis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Posterior stabilization of the injured lumbar spine resulting from trauma or neoplasm is an important component in surgical management [26]. Pedicle screw fixation has become a popular method of spinal internal fixation [14]. Gaines [7], Steinman et al. [23] and Whitecloud et al. [25] reported that King described the first spinal arthrodesis performed using pedicles screws in 1944. Since then many authors have refined the technique of pedicle screw placement. Knowledge of the pedicles is necessary for the safe application of these systems. This has been the impetus for several studies of lumbar pedicle anatomy. Some researchers have used computed tomography (CT) data to assess pedicle anatomy [2, 13, 14, 19, 22, 24, 27]. Others have directly assessed lumbar pedicle anatomy using calipers and goniometers or specially designed devices [2, 4, 8, 9, 14, 16, 20, 21]. Although knowledge of pedicle morphology has been obtained as a result of these researches, the complications of the method of pedicle screw fixation have not yet been solved [7, 12]. Most of the reported data have been obtained from investigations in Western countries [2, 8, 9, 14, 20], and other populations have rarely been investigated [8, 9]. This study aimed to determine indices of lumbar pedicle anatomy of the Eastern Anatolian population, and to compare these data with the results of all previously reported researches.
Materials and methods
Lumbar pedicle anatomy was measured in two groups of specimens. In the first group lumbar pedicle measurements were taken in 29 subjects without spinal disorder (14 women, 15 men; age range 18–39 years; mean age 35 years). In the second group pedicle measurements were obtained from 16 dried human spinal columns stored in the Department of Anatomy. The measurements were taken with a caliper (± 0.1 mm) and goniometer (± 0.1°) in the second group and by CT in the first group. A radiologist (A.L.) performed the measurements of lumbar pedicle anatomy in the first group. In the second group, the senior author assessed all specimens.
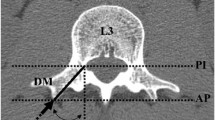
The interpedicular distance (IPD) was measured at the midshaft of the pedicle. We chose the narrowest dimensions of pedicles in both the transverse and the sagittal planes as the pedicle width (PW, mediolateral outer cortical of the pedicle) and the pedicle height (PH, craniocaudal outer cortical diameter of the pedicle), respectively. The transverse pedicle angle (TPA) was obtained by measuring the angle between a Steinmann pin (a line in CT) placed through the center of the pedicle and a line parallel to the vertebral midline in the transverse plane. The sagittal pedicle angle (SPA) was measured between the Steinmann pin (a line in CT) and the posterior vertebral body border in the sagittal plane. The length of the pedicle was measured from posterior cortex to the midpoint of the anterior vertebral cortex at each spinal level (PAL) (Figs. 1, 2).

Description of vertebral measurements taken from the superior-inferior aspect. Interpedicular distance was measured at the midshaft of the pedicle (IPD). Pedicle width was the narrowest dimension of the pedicle in the transverse plane (PW). Length of the pedicle was measured from the posterior cortex to the mid-point of the anterior vertebral cortex (PAL). Transverse pedicle angles (TPA) were obtained by measuring the angle between the PAL and the vertebral midline in the transverse plane

Description of vertebral measurements taken from the lateral aspect. Pedicle height was measured as the narrowest dimension of the pedicle in the sagittal plane (PH). Sagittal pedicle angles (SPA) were obtained by measuring the angle between the PAL and the posterior vertebral body border (pvbb) in the sagittal plane
The pedicle measurements obtained from this study were compared with those previously reported. All data were analyzed using a frequent and paired sample test by SPSS software.
Results
Interpedicular distance
The widest IPD measured at the midline of each pedicle was different in the two groups. But in each group the IPD was the narrowest at the L1 vertebra and widest at the L5 vertebra (p<0.001). The statistical relation was significant between first and second groups at L1 (p<0.05). The relation of the findings at L5 was similar to that at L1. It was very significant between the two groups (p<0.001). These findings are shown in Table 1.
Pedicle widths
In our study, the pedicle width (PW) ranged from 4 to 14 mm. PWs increased from rostral to caudal. PWs obtained in the first group were wider than those in the second group. In both groups, a very significant relation was found between the data on L1 and L5. These differences between groups reached statistical significance at L1 (p<0.001), L3 (p<0.001) and L5 (p<0.05) (Table 2).
Pedicle heights
Among the data on two groups, the lowest value of pedicle height (PH) was 8.2 mm and the highest value, 19.7 mm. PHs decreased from L1 to L5 in both groups. In addition, the statistical relation between vertebral levels was significant except for L1 and L2 in the first group (p<0.05); it was not significant except from L1 to L4 and from L1 to L5 in the second group (p<0.05, p<0.001, respectively). According to data on L1, L3 and L5, there were very significant differences between the first and second groups (p<0.001) (Table 3).
Transverse pedicle angles
Although the TPAs in both groups ranged from 6° to 19°, the values in the first group were larger than those in the second group (p<0.001). TPAs increased from L1 to L5. The difference between L1 and L5 was significant in the second group (p<0.05) and very significant in the first group (p<0.001). These statistically significant differences varied between 6° and 19° (Table 4).
Sagittal pedicle angles
The sagittal pedicle angles (SPAs) measured in our study are depicted in Table 5. The widest SPAs were observed in the first group, while the narrowest SPAs were measured in the second group. SPAs showed a 1–5° difference from L1 to L5; this was statistically significant (p<0.05). But even the differences at vertebral levels in the first group were not significant.
Pedicle axis lengths
The pedicle axis length (PL) was longest at L1 and shortest at L5. There was a significant difference between the measurements at L1 and L5 in the first group (p<0.05). However, the differences among levels were not significant in the second group (Table 6).
Discussion
Posterior stabilization of lumbar spine injury resulting from trauma or neoplasm is an important component in surgical management [3, 4, 5, 6, 11, 17, 23, 26, 28]. In many cases, spinal instrumentation reduces fracture-dislocation and helps to maintain stability of the spine, thereby facilitating neurological recovery by improving vertebral alignment. Late neurological sequelae and disabling mechanical pain related to post-traumatic kyphosis may also be prevented [26]. In recent years, internal fixation of the spine using pedicle screws and rods has been a widely used treatment method. Therefore, knowledge of the morphology of the pedicles is necessary for the safe and appropriate application of these systems [2, 7, 12, 14, 18].
Various researchers have studied pedicle anatomy. The results of some previous studies are listed and compared with those of the present study in Table 7. Krag et al. [10] used CT data to assess pedicle anatomy of the low thoracic and lumbar vertebrae. Panjabi et al. [16] and Semaan et al. [21] used specially designed morphometers to measure the pedicle dimensions of vertebrae. McCormack et al. [14] measured only the pedicles of thoracic vertebrae using calipers and a goniometer. Berry et al. [2], Hou et al. [8] and Scoles et al. [20] reported the results of measurements obtained from only selected thoracic and lumbar vertebrae. Zindrick et al. [27] reported the average and range of anterior vertebral cortex dimensions obtained from all thoracic and lumbar vertebrae in addition to measurements of previously reported studies. Then, two studies using similar measurements were carried out in far Eastern populations [8, 9].
In the present study, the same measurements were taken only in lumbar vertebrae. However, we examined the pedicle anatomy of lumbar vertebrae by cadaveric and CT data, and investigated the correlations between the data. We obtained all the measurements in young or middle-aged subjects because we aimed to exclude spinal degenerative disorders and to take consistent measurements.
The dimensions of the vertebral canal gradually increased from rostral to caudal. In our study, IPD was wider in dried vertebrae than on CT. The IPD measurements in our study are in agreement with those reported by Berry et al. [2] and Scoles et al. [20]. Some authors regard the IPD as the transverse diameter of the vertebral foramen [2, 14, 20], but Chaynes et al. [4] think that it is not applicable to the relationship between the two pedicles of a vertebra.
Selection of a suitable diameter of transpedicular screw is an important issue for safe surgical placement [10, 28]. It has been emphasized that the insertion of a badly fitting screw with anatomical constraints may result in failure of fixation or fracture of the pedicle [4, 9, 10, 28].
Pedicle dimensions in this study were consistent with those of previous studies in the literature [2, 7, 8, 9, 18, 20, 27, 28]. The narrowest dimension of the ovoid-shaped pedicle is in the transverse plane [15]. The average width in this plane was reported to range from 18 mm in the L5 vertebra to 7 mm in the L1 vertebra. PWs in L1 and L5 were found to be 7.0 mm and 10.9 mm, respectively, by Berry et al. [2], 7.0 mm and 12.9 mm by Hou et al. [8], 6.8 mm and 18.4 mm by Kim et al. [9], 10.3 mm and 21.6 mm by Robertson and Stewart [18], 7.4 mm and 9.9 mm by Scoles et al. [20] and 8.7 mm and 18.0 mm by Zindrick et al. [27]. We determined the average PWs to range from 4 mm to 14 mm in all our specimens. The dimension of PW increased caudally. PWs obtained from CT examinations were slightly wider than those on dried vertebrae. This may be due to mistakes in calculating the magnification during CT examinations. However, it is of interest that PW values reported from two studies using the same methods appeared to be very different in closely similar populations [8, 9].
PHs were wider than PWs and decreased from rostral to caudal in this study. The narrowest PH was 8.2 mm, and the widest 19.7 mm among all our specimens. We observed the PHs in our cadaveric vertebrae were smaller compared with the PHs noted by Berry et al. [2], Hou et al. [8] and Zindrick et al. [27]. In comparison with the studies of Hou et al. and Zindrick et al., a difference was seen between values of PWs and PHs. PWs and PHs determined by Hou et al. [8] were significantly smaller than those reported by Zindrick et al. [27]. PHs of dried vertebrae measured in our study were smaller than those reported by Hou et al. [8].
PL is longest at the L1 vertebra and shortest at the L5 vertebra in our study. In view of the measurement methods, our data are similar to the values of PL reported by Hou et al. [8], Scoles et al. [20] and Zindrick et al. [27]. The pedicle axis assessed by Hou et al. [8] was closer to the midline than that reported by Zindrick et al. [27]. In our data, the pedicle was shorter and wider than that in previously reported studies. There were significant differences between L1 and L5 from CT findings, while no differences were found in the values of PL obtained from cadaveric vertebrae. Our PL values were longer than the measurements noted by Hou et al. [8] and Scoles et al. [20], and not different from those reported by Zindrick et al. [27]. It is interesting that the longest PL value is reported in the Chinese population. In contrast to our data, the values of PL noted by Scoles et al. [20] increased from rostral to caudal. The findings reported by Scoles et al. [20] do not agree with the PL values determined by Hou et al. [8] and Zindrick et al. [27].
Proper angular placement of a pedicle screw in the sagittal and transverse planes is an additional issue and various screw orientations have been proposed to avoid neurological complications [4]. Although TPAs ranged from 6° to 19° as calculated from CT findings and cadaveric vertebrae, TPAs calculated from CT findings were wider than TPAs measured in dried vertebrae. We observed that TPAs increased from L1 to L5. These differences were significant, and had a range of 9–10°. This range was approximately 24° in the study by Berry et al. [2], 20° in that by Zindrick et al. [27] and 12° in measurements reported by Scoles et al. [20]. The pedicle angles are medial to midline in the transverse plane. TPAs were widest at the lower lumbar vertebrae; they narrowed rostrally, and approximated to neutral at L1.
SPAs were smaller in our cadaveric vertebrae compared with the SPAs measured on CT scans. SPAs showed differences that ranged between 1° and 5° from L1 to L5 in dried vertebrae. But these differences were not observed in findings obtained from CT scans. SPAs similar to TPAs increased from cephalad to caudal [2, 20, 27]. However, the angular relationships between the pedicle and vertebral body are highly variable and largely unpredictable [20].
The observations presented here have defined many of the anatomical parameters that should be taken into consideration for spinal instrumentation. The IPD dictates that the length of the transverse fixator system will range from 22 mm to 32 mm depending on the spinal level. Also, the diameter of screw should be compatible with the pedicular width. Using a mean diameter of 5–7 mm can be successful in instrumentation of the lumbar spine. Knowledge of the pedicle axis length (distance from anterior vertebral cortex) is important to avoid perforations of the anterior vertebral cortex and probable injury of neural structures during screw insertion in internal fixation with transpedicular screws. In addition, it is recommended that the depth of screw insertion into the vertebral body should be near but not penetrate the anterior vertebral cortex, to prevent or minimize instrument failure. Therefore, preoperative radiological assessment helps the determination of pedicle screws, in the way that intraoperatively using fluoroscopy may guide insertion of the screws. According to the findings of previously reported studies and our study, the length of pedicle screws is limited to 45 mm at the lumbar vertebrae. The pedicular angles play an important role in the overall stability of the fixation.
Conclusion
Pedicle dimensions and angles vary from region to region in spine. Although some differences were seen between different levels of the lumbar spine, these differences were not important. When carrying out pedicle screw fixation a surgeon should be aware of the pedicle dimensions and relations for the prevention of fixation failure and screw breakage, avoiding injuries to the neural structures. Calculation of PL is essential for screw selection. However, screw insertion is always checked intraoperatively by fluoroscopy or an image intensifier.
References
Aebi M, Etter C, Kehl T, Thalgott J (1988) The internal skeletal fixation system: a new treatment of thoracolumbar fractures and other spinal disorders. Clin Orthop 227: 30–43
Berry JL, Moran JM, Berg WS, Steffee AD (1987) A morphometric study of human lumbar and selected thoracic vertebrae. Spine 12: 362–367
Blumenthal S, Gill K (1993) Complications of the Wiltse pedicle screw fixation system. Spine 18: 1867–1871
Chaynes P, Sol J-C, Vaysse P, Becue J, Lagarrigue J (2001) Vertebral pedicle anatomy in relation to pedicle screw fixation. Surg Radiol Anat 23: 85–90
Ciappetta P, Delfini R, Costanzo G (1996) Posterolateral decompression and stabilization of thoracolumbar injuries using Diapason instrumentation. Acta Neurochir (Wien) 138: 314–321
Denis F (1983) The three-column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 8: 817–831
Gaines RW Jr (2000) The use of pedicle-screw internal fixation for the operative treatment of spinal disorders. J Bone Joint Surg Am 82: 1458–1476
Hou S, Hu R, Shi Y (1993) Pedicle morphology of the lower thoracic and lumbar spine in a Chinese population. Spine 18: 1850–1855
Kim NH, Lee HM, Chunk IH, Kim HJ, Kim SJ (1994) Morphometric study of the pedicles of thoracic and lumbar vertebrae in Koreans. Spine 19: 1390–1394
Krag MH, Beynon BD, Pope MH, Frymoyer JW, Haugh LD, Weaver DL (1986) An internal fixator for posterior application to short segments of the thoracic, lumbar or lumbosacral spine: design and testing. Clin Orthop 203: 75–98
Lee TC (1996) Transpedicular reduction and stabilization for postlaminectomy lumbar instability. Acta Neurochir (Wien) 138: 139–145
Loenstein JE, Denis F, Perra JH, Pinto MR, Smith MD, Winter RB (1999) Complications associated with pedicle screws. J Bone Joint Surg Am 81: 1519–1528
Luque ER (1986) Interpeduncular segmental fixation. Clin Orthop 203: 54–57
McCormack BM, Benzel EC, Adams MS, Baldwin NG, Rupp FW, Maher DJ (1995) Anatomy of the thoracic pedicle. Neurosurgery 37: 303–308
Nagel DA, Edwards WT, Schneider E (1991) Biomechanics of spinal fixation and fusion. Spine 16 (Suppl): S151–S154
Panjabi MM, Goel V, Oxland T, Takata K, Duranceau J, Krag M, Price M (1992) Human lumbar vertebrae. Quantitative three-dimensional anatomy. Spine 17: 299–306
Pihlajamäki H, Böstman O, Ruuskanen M, Myllynen P, Kinnunen J, Karaharju E (1996) Posterolateral lumbosacral fusion with transpedicular fixation. Acta Orthop Scand 67: 63–68
Robertson PA, Stewart NR (2000) The radiologic anatomy of the lumbar and lumbosacral pedicles. Spine 25: 709–715
Roy-Camille R, Saillant G, Mazel C (1986) Internal fixation of the lumbar spine with pedicle screw plating. Clin Orthop 203: 7-17
Scoles PV, Linton AE, Latimer B, Levy ME, Digiovanni BF (1988) Vertebral body and posterior element morphology: the normal spine in middle life. Spine 13: 1082–1086
Semaan I, Skalli W, Veron S, Templier A, Lassau J-P, Lavaste F (2001) Anatomie quantitative tridimensionnelle du rachis lombaire. Rev Chir Orthop 87: 340–353
Steffee AD, Biscup RS, Sitkowski DJ (1986) Segmental spine plates with pedicle screw fixation. A new internal fixation device for disorders of the lumbar and thoracolumbar spine. Clin Orthop 203: 45–53
Steinmann JC, Herkowitz HN, El-Kommos H, Wesolowski DP (1993) Spinal pedicle fixation. Confirmation of an image-based technique for screw placement. Spine 18: 1856–1861
Ullrich CG, Binet EF, Sanecki MG, Kieffer SA (1980) Quantitative assessment of the lumbar spinal canal by computed tomography. Radiology 134: 137–143
Whitecloud TS III, Butler JC, Cohen JL, Candelora PD (1989) Complications with the variable spinal plating system. Spine 14: 472–476
Yoganandan N, Larson SJ, Pintar F, Maiman DJ, Reinartz J, Sances A (1990) Biomechanics of lumbar pedicle screw/plate fixation in trauma. Neurosurgery 27: 873–881
Zindrick MR, Wiltse LL, Doornik A, Widell EH, Knight GW, Patwardan AG, Thomas JC, Rothman SL, Fields BT (1987) Analysis of the morphometric characteristics of the thoracic and lumbar pedicles. Spine 12: 160–166
Zindrick MR, Wiltse LL, Widell EH, Thomas JC, Holland WR, Field BT, Spencer CW (1986) A biomechanical study of intrapedicular screw fixation in the lumbosacral spine. Clin Orthop 203: 99–112
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kadioglu, H.H., Takci, E., Levent, A. et al. Measurements of the lumbar pedicles in the Eastern Anatolian population. Surg Radiol Anat 25, 120–126 (2003). https://doi.org/10.1007/s00276-003-0109-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-003-0109-y