
Abstract
A study was made of 100 homogeneous CT scans of the petrous part of the temporal bone to determine whether or not the arcuate eminence (AE) is a good landmark for the superior semicircular canal (SSCC) in the suprapetrous approach to the internal acoustic meatus which is used in the extirpation of acoustic neuromas. Direct measurements were made on consecutive coronal sections, 1 mm thick. The AE was absent from the petrous surface in 15% of cases. It corresponded to the relief of the SSCC in 37% of cases; laterally, however, it was separated from the petrous cortex by bone whose thickness varied from 0.5 to 5 mm. Finally, in 48% of cases, the AE was not a good landmark for the canal although nonetheless it participated in the development of this bulge in 46% of cases, always lying towards the medial border of the pneumatized eminence. In addition, study of the coronal sections with MRI allowed us to confirm that the AE does not routinely correspond to the imprint of a temporal sulcus. The AE, whose presence on the petrous surface is due to the combined effects of the SSCC, the air cells of the petrous part of the temporal bone and the temporal sulci, is only a good guide to the SSCC in 37% of cases and should not be considered as a reliable surgical landmark.
Résumé
Pour déterminer si l'eminentia arcuata constitue ou non un bon repère du canal semi-circulaire antérieur (CSCA) dans la voie d'abord sus-pétreuse du méat acoustique interne, mise à profit lors de l'exérèse chirurgicale d'un neurinome du VIII, l'étude a été menée à partir d'une série homogène de 100 scanners du rocher. Les mesures ont été réalisées directement, au double décimètre, sur des coupes coronales, jointives, d'un millimètre d'épaisseur. L'eminentia arcuata était absente de la surface pétreuse dans 15% des cas. Elle correspondait au relief du CSCA dans 37% des cas, ce dernier étant alors séparé de la corticale pétreuse par une épaisseur d'os variant de 0,5 à 5 mm. Enfin dans 48% des cas, l'eminentia arcuata n'était pas un bon repère du canal, lequel participait néanmoins à la genèse de cette saillie dans 46% des cas, toujours situé sous le versant médial de l'éminence pneumatisée. En outre, l'analyse de coupes coronales en IRM nous a permis d'affirmer que l'eminentia arcuata ne correspond pas systématiquement à l'empreinte d'un sillon temporal. L'eminentia arcuata, dont la présence à la surface pétreuse tient aux rôles combinés du CSCA, des cellules aérifères du rocher et des sillons temporaux, n'est un bon repère du CSCA que dans 37% des cas, ce qui ne peut autoriser à la considérer comme un repère chirurgical fiable.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The arcuate eminence (AE) is the classical landmark of the internal acoustic meatus in the suprapetrous surgical approach. Paturet [8] described it as a smooth rounded bulge with its long axis obliquely forwards and inwards, lying very close to the superior border of the petrous part of the temporal bone at the junction between the lateral third and medial two thirds. Considered as the relief of the superior semicircular canal (SSCC), it does not always seem to correspond to it. The aims of this radioanatomical study were to understand, through CT scanning and MRI, the structure of the AE, to define its relationships with the structures of the inner ear which are at risk through surgical approaches and to study its reliability as a surgical landmark.
Materials and methods
Computed tomographic study
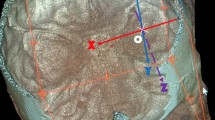
A homogeneous series of 100 computed tomographic (CT) scans of the petrous part of the temporal bone carried out between January and December 1998 in the radiology department of the Hôtel-Dieu of Nantes was studied (Fig. 1). The images were stored in the departmental archive and were of patients who presented with otological pathology without any pathological changes in the petrous structures. Twenty cases were bilateral and allowed a study of symmetry. All sections were carried out with a Philips Tomoscan AVE1 CT scanner. They were consecutive 1 mm thick sections carried out in the 350–450 HU zone and a scale of ±2000. Three-dimensional reconstruction was not used as it was not part of the routine clinical assessment and the aim of this study was to give the surgeon the data which would be available in daily practice.

Distribution of the subjects for both age and gender
The scale of the scans allowed direct measurement of the millimetric dimensions on the films. The measurements were carried out on coronal sections passing through both the SSCC and the AE, when it was found. Only these sections were retained since they made up the surgical landmarks par excellence for the suprapetrous approach. The following were calculated:
- (1):
-
To study the relationship between the SSCC and the AE: Measurements of the distance (in millimeters) separating the SSCC from the AE on the most cranial section of the petrous part of the temporal bone, the distance (in millimeters) separating the SSCC from the AE on the most caudal section and the distance (in millimeters) separating the summit of the SSCC from the AE. Whenever possible, the location of the canal within the AE was defined.
- (2):
-
To study the structure of the AE: Measurement of the height of the AE, measurement of the thickness of the bone covering the roof of the SSCC and an assessment of the pneumatization of the AE.
MRI study
T2-weighted coronal sections passing through the petrous part of the temporal bone and the temporal lobe were used. This approach allowed analysis of the relationships between the AE and the telencephalic structures. It was easy to see the gyri and sulci. The AE corresponded to the highest point of the petrous part of the temporal bone. Its relationships with the sulci were noted. Five cases were studied. The variability of the results meant that a larger study was not necessary.
Results
The results are summarized in Fig. 2.

Correspondence between the arcuate eminence (AE) and the superior semicircular canal (SSCC) (100 scans). White, AE absent; grey, AE corresponds to the SSCC; black, AE does not correspond to the SSCC
CT study
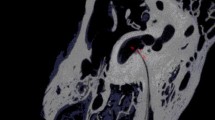
In 15 cases out of 100, it was not possible to identify the AE. In 14 cases, the superior endocranial surface of the petrous part of the temporal bone was not marked by any relief (Fig. 3). In one case, a regular layer of pneumatized bone overlay the canal, leveling the petrous surface (Fig. 4). In one case, the endocranial surface had several reliefs which meant it could not be determined which truly corresponded to the AE (Fig. 5).

Coronal sections of the petrous part of the right temporal bone. Note the absence of the arcuate eminence. 1, Superior semicircular canal; 2, horizontal semicircular canal; 3, vestibule; 4, internal acoustic meatus; 5, air cells; 6, mastoid process

Coronal sections of the petrous part of the right temporal bone. Note the absence of the arcuate eminence. 1, Superior semicircular canal; 2, horizontal semicircular canal; 3, vestibule; 4, internal acoustic meatus; 5, air cells

Coronal section of the petrous part of the right temporal bone. Multiple reliefs of the petrous surface. 1, Superior semicircular canal; 2, horizontal semicircular canal; 3, vestibule; 4, internal acoustic meatus; 5, air cells
In 37 cases out of 100, there was an exact correspondence between the SSCC and AE whatever the level of the section. It seemed of value to distinguish here two categories:
- (1):
-
In 23 cases, the AE was "non-pneumatized", i.e., clearly delineated and bulging, it corresponded exactly and uniquely to the SSCC. Its height varied between 2 and 6 mm. The canal was, therefore, separated from the dura mater lining the middle cranial fossa by a fine layer of compact bone no thicker than 2 mm (Fig. 6).
Fig. 6. 
Coronal section of the petrous part of the right temporal bone. Perfect correspondence between the arcuate eminence and the superior semicircular canal. 1, Superior semicircular canal; 2, horizontal semicircular canal; 3, vestibule; 4, internal acoustic meatus; 5, air cells; 6, arcuate eminence
- (2):
-
In 14 cases, the AE was "pneumatized", i.e., made up of air cells. The canal, although exactly underneath the AE, could not explain the relief on its own. The thickness of bone covering the canal could thus attain 5 mm and the height of the AE varied between 1.5 and 6 mm (Fig. 7).
Fig. 7. 
Coronal section of the petrous part of the right temporal bone. Pneumatized arcuate eminence above the superior semicircular canal. 1, Superior semicircular canal; 2, horizontal semicircular canal; 3, vestibule; 4, internal acoustic meatus; 5, air cells; 6, arcuate eminence


In 48 cases out of 100, the AE did not correspond to the relief of the SSCC., There were, however, some variations:
- (1):
-
In two cases, the AE was at a distance from the SSCC. It was made up of pneumatized bone, slightly prominent (its height varying from 2 to 6 mm). It lay more laterally than the canal. The latter, whose summit was situated more than 5 mm medially with respect to the AE, could not explain this relief. In these two cases, a fine bony layer 1 mm thick separated the canal from the middle cranial fossa (Fig. 8).
Fig. 8. 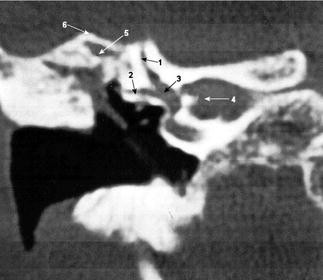
Coronal section of the petrous part of the right temporal bone. Arcuate eminence without any relationship to the superior semicircular canal. 1, Superior semicircular canal; 2, horizontal semicircular canal; 3, vestibule; 4, internal acoustic meatus; 5, air cells; 6, arcuate eminence
- (2):
-
In 46 cases, the SSCC was in a very variable position within the AE, which sometimes a simple small bony crest could also extend over the petrous surface without clear margins as follows:

- (1):
-
In 18 cases, the SSCC only partially corresponded to the summit of the AE, sometimes on the sections passing through the summit of the canal and sometimes on the more cranial sections. In fact, as the two structures do not have the same access, the canal could not suffice to explain the AE. It always consisted of a "semipneumatized" AE whose height varied between 1 and 6 mm.
- (2):
-
In 28 cases, the canal never corresponded to the summit of the AE whatever the level of the sections. The AE, whose height varied from 1 to 7 mm, was "semipneumatized", which was perfectly shown on CT section 7. The AE was made up both of compact bone in its medial part (site of the canal) and air cells in its lateral part. In these 28 cases, the summit of the canal was always sited towards the medial border of the AE (Fig. 9).
Fig. 9. 
Coronal section of the petrous part of the right temporal bone. Arcuate eminence with no relationship with the superior semicircular canal but a morphogenetic role determining the air cells. 1, Superior semicircular canal; 2, horizontal semicircular canal; 3, vestibule; 4, internal acoustic meatus; 5, air cells; 6, arcuate eminence

Study of 20 bilateral cases showed almost constant disparities between the right and left sides, confirming the extreme variability of this structure.
MRI study
The immediately disparate character of our data led us to limit the number of cases studied to five. In only two cases did the AE correspond perfectly to the third temporal sulcus and might, therefore, have been created by it. The SSCC was thus constantly found on the medial border of the AE (Fig. 10). In one case, the AE was absent and the SSCC was found under the third temporal sulcus. In one case, the AE lay under the second temporal sulcus with the SSCC opposite the third temporal sulcus. Finally, in another case the AE lay opposite the gyrus without any relationship either with the third temporal sulcus or with the SSCC (Fig. 11).

Coronal MRI section of the petrous part of the right temporal bone. Arcuate eminence under the third temporal sulcus and superior semicircular canal lying medially. 1, superior semicircular canal; 2, horizontal semicircular canal; 3, internal acoustic meatus; 4, vestibule; 5, third temporal sulcus; 6, arcuate eminence

Coronal MRI section of the petrous part of the right temporal bone. Arcuate eminence related to the third temporal gyrus and superior semicircular canal lying medially. 1, superior semicircular canal; 2, horizontal semicircular canal; 3, internal acoustic meatus; 4, vestibule; 5, third temporal sulcus; 6, arcuate eminence; 7, third temporal gyrus; 8, third temporal sulcus
Discussion
Classical teaching suggests that the AE corresponds to the relief of the SSCC [9]. However, Bellocq [1], in his study of the adult human temporal bone, stated that the SSCC was more medial than the AE, which it did not detail. He placed the canal at the inferior third of the antero-medial side of the AE. Charachon and Accoyer [2], studying the landmarks for the internal acoustic meatus during the suprapetrous surgical approach, added that the canal was not fixed with respect to the AE, was more anterior and medial than the latter, did not always correspond to the position indicated by Bellocq and could be sited at the summit or on the anterior side of the AE.
Girard [3] thought that the AE was only an elevation of the petrous cortex by the subjacent air cells and thus had no direct relationship with the SSCC.
Finally, Paturet [8] and Hovelacque [6] considered this bulge as the equivalent of the numerous eminences found on the base of the skull corresponding to the sulci and fissures of the brain. The AE should correspond to the posterior part of the sulcus separating the third and forth temporal gyri. Guerrier and Guerrier [4] confirmed this hypothesis, emphasizing that the AE is not a prominence related to the SSCC but more associated with a cerebral sulcus. More recently Tsunoda et al. [12] reinforced this hypothesis on 28 petrous parts of temporal bones, noting the absence of the AE in two cases and the existence of several eminences in a third of cases. Still more recently [13], on 46 bones studied, he found the AE in 80% of cases and stressed that it did not correspond with the SSCC, emphasizing the participation of the temporo-occipital sulci in its formation but in an inconstant fashion.
Three hypotheses can be proposed: the AE corresponds to (1) the SSCC, (2) the subjacent air cells or (3) the third temporal sulcus. Our study showed that these three hypotheses can be sustained and are variably associated, which excludes any single theory of the origin of the AE. It needs to be emphasized above all that the AE is an inconstant relief which is not generally accepted. It is indeed absent from the petrous surface in 15% of cases. This result is verified by Kartush et al.'s study [7] of 60 petrous parts of temporal bones.
Finally, the AE only corresponds explicitly to the relief of the SSCC in 23% of cases, confirming Rouvière and Delmas' hypothesis [9]. It is thus the slightly pneumatized petrous parts of temporal bones in which the only relief determining the AE is the bulge of the canal under the petrous cortex. On the heavily pneumatized petrous parts of temporal bones on the other hand, the air cells emanating from the mastoid process accumulate under the petrous cortex [3]:
-
They may lie exactly over the canal, explaining why it is sometimes necessary to ream several millimeters of pneumatized bone before discovering the canal.
-
They may accumulate laterally against the canal, explaining those eminences which appear "mixed" on CT scanning and are made up of compact bone medially and pneumatized bone laterally. It is to be noted that the pneumatization of the eminence always comes from its lateral side. This supports the idea of Bellocq [1] and Charachon and Accoyer [2] that the canal can be found at the summit of the AE or on its medial side but never on its lateral side.
-
They may be irregularly spread over the petrous surface, explaining why the eminence can be very difficult to discern on some petrous parts of the temporal bone or even completely absent.
There remains the MRI study of the last hypothesis, according to which, the AE is fashioned by the temporal cortex [6, 8, 12, 13]. Perfect correspondence with the temporal cortex, particularly at the third sulcus, was found in only two cases out of five.
The AE seems to escape all attempts to systematize it. Of very variable shape, this elevation of petrous cortex may represent the SSCC, a temporal sulcus, air cells or all three. The air cells, coming from the mastoid and varying in number, accumulate on the reliefs of the labyrinth facing the ring of the SSCC which they push medially and thus model the petrous surface under the pressure from the temporal lobe. It is, therefore, important to alert surgeons to these anatomical facts since surgical articles mention the AE as the first landmark to the internal acoustic meatus via the suprapetrous approach with the aim of preserving hearing, without taking account of the variations which we have just emphasized [10] or even mentioning them [5, 11].
Conclusion
The AE is absent from the petrous surface in 15% of cases and only seems to be a good landmark for the SSCC in 37% of cases, which certainly does not allow it to be considered as a reliable surgical landmark in the suprapetrous approach to the internal acoustic meatus. It should be added that the canal is thus found more or less deeply situated under the eminence and it is sometimes necessary to abrade up to 5 mm of bone before discovering its loop.
However, in other cases (48%) we noted that the canal was roughly situated under the medial side of the eminence. The tends to support current surgical techniques which consist of abrading with precautions and under continuous irrigation the medial side of the AE as far as the "blue line" of the SSCC. This technique, however, remains dangerous since the eminence presents a very variable appearance between different bones and a landmark is sometimes difficult to see. Preoperative CT with coronal sections is essential. There is unquestionably a model indication for neuronavigation-assisted surgery preceded by radiological three-dimensional reconstruction, but that does not allow one to forget the numerous anatomical variations which we would wish to emphasize.
Overall, given the pneumatization of the petrous part of the temporal bone—sometimes by the SSCC, sometimes by the air cells or temporal sulci—the AE is a poor landmark for the surgeon.
References
Bellocq P (1924) L'os temporal chez l'homme adulte. Strasbourg-Médical, Strasbourg
Charachon R, Accoyer B (1976) Notes techniques sur le repérage du conduit auditif interne. Acta Oto-Rhino-Laryngol Belg 30: 76–83
Girard L (1938) Atlas d'anatomie et de médecine opératoire du labyrinthe osseux. Maloine, Paris
Guerrier Y, Guerrier B (1976) Anatomie topographique et chirurgicale du rocher. Acta Oto-Rhino-Laryngol Belg 30: 22–50
Holsinger FC, Cocker NJ, Jenkins HA (2000) Hearing preservation in conservation surgery for vestibular schwannoma. Am J Otol 21: 695–700
Hovelacque A (1934) Ostéologie II, Crâne-Face. Douin, Paris, pp 65–74
Kartush JM, Kemink JL, Graham MD (1985) The arcuate eminence topographic orientation in middle cranial fossa surgery. Ann Otol Rhinol Laryngol 94: 25–28
Paturet G (1951) Traité d'anatomie humaine. Masson, Paris, p 130
Rouvière H, Delmas A (1984) Anatomie humaine, 12th edn, vol 1. Masson, Paris, p 56
Slattery WH, Brackmann DE, Hitselberger W (1997) Middle fossa approach for hearing preservation with acoustic neuromas. Am J Otol 18: 596–601
Staecker H, Nadol JB, Ojeman R, Ronner S, McKenna MJ (2000) Hearing preservation in acoustic neuroma surgery: middle fossa versus retrosigmoid approach. Am J Otol 21: 399–404
Tsanuda A, Kimura Y, Sumi T, Komatsuzaki A, Sato T (2000) The arcuate eminence is not a protrusion of the superior semi-circular canal but a trace of sulcus on the temporal lobe. J Laryngol Otol 114: 339–344
Tsanuda A (2001) Arcuate eminence in Caucasian populations. J Laryngol Otol 115: 9-13
Tsanuda A, Komatsuzaki A, Kobayashi M, Suzuki Y (2001) Three-dimensional image for the middle fossa approach and its anatomical considerations. Laryngoscope 111: 1048–1052
Acknowledgements
We thank S. Lagier and Y. Blin for technical collaboration.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Faure, A., Masse, H., Gayet-Delacroix, M. et al. What is the arcuate eminence?. Surg Radiol Anat 25, 99–104 (2003). https://doi.org/10.1007/s00276-003-0102-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-003-0102-5