
Abstract
Purpose
The purpose of this study is to accentuate the efficacy of direct stenting (stent placement without predilatation of the lesion) in patients with acute lower limb arterial ischemia (ALLI).
Materials and Methods
Between January 2010 and September 2015, 16 patients (11 men and 5 women) underwent direct stenting of acute arterial occlusions. All patients had contraindication for surgical revascularization or catheter-directed thrombolysis. According to SVS/ISCVS Classification, six patients had IIa and ten patients IIb ALLI. The occlusions were located in CIA, EIA, SFA, or popliteal artery. Mean follow-up time with clinical examination and color Duplex ultrasonography was 37.6 months (range 1–72). We analyzed the technical and clinical outcomes of the procedures, as well the complications and patency rates.
Results
Technical success was achieved in all patients (16/16) and there was significant clinical improvement in 15 patients. There was neither distal embolization nor procedure-related complications. During the 6 years of follow-up, four patients died due to non-procedure-related causes and there were two minor and one major amputations. The primary patency rates and the amputation-free survival rates were 93.7 and 87% at 1 year, 75.2 and 71.2% at 3 years, and 75.2 and 62.3%, respectively, at 6 years.
Conclusions
Direct stenting may be a valuable alternative procedure for acute arterial occlusions in selected cases with high technical success and significant clinical improvement.
Level of Evidence
Level 4, Case Series.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acute lower limb ischemia (ALLI) represents a quickly developing or sudden decrease in limb perfusion, resulting in a potential threat to the viability of the extremity [1]. The hypoperfusion also impairs cardiopulmonary and renal function due to systemic acid–base and electrolyte abnormalities [2]. Causes of ALLI include acute thrombosis of a limb artery or bypass graft, embolism from the heart, dissection, and trauma [3]. A limb-threatening ischemic event is characterized acute if the duration of symptoms is less than 14 days, subacute between 15 days and 3 months, and chronic after 3 months [4]. Α patient with ALLI often presents with the “5 P’s” of paresthesia, pain, pallor, pulselessness, and paralysis, and the incidence is about 1.5 cases per 10,000 persons per year [5]. Patients with ALLI have poor short-term outcomes, with a risk of amputation between 10 and 30% and a mortality rate of approximately 15–20% in the first year, mainly in the peri-operative period [1, 6].
The management includes either surgical procedures [7–10] or percutaneous endovascular procedures such us catheter-directed thrombolysis, manual aspiration thrombectomy, and mechanical thrombectomy [4, 11–14]. Surgical revascularization is the classic treatment and includes procedures such us embolectomy with a Fogarty catheter, bypass grafting, and endarterectomy [3]. Despite there is no significant difference in limb salvage rate or mortality between surgical procedures and catheter-directed thrombolysis [8], surgical procedures are associated with higher incidence of infections, rethrombosis, or fasciotomy [10]. Surgical procedures and administration of anesthesia are associated with a complex stress response. The American Society of Anesthesiologists (ASA) grading system offers a simple description of the physical state of a patient and is a component of the overall procedural risk [15]. Despite improvements in pre- and peri-operative management, arterial thromboembolectomy is characterized by high morbidity and mortality in elderly patients with an ASA score ≥ III [16]. On the other hand, catheter-directed thrombolysis may be effective for treating acute limb ischemia caused by thrombotic or embolic occlusions but it is associated with substantial risk of major hemorrhage and stroke [9, 17, 18]. There are also absolute or relative contraindications for catheter-directed thrombolysis such us ongoing bleeding, intracranial hemorrhage, compartment syndrome, recent eye surgery, and recent gastrointestinal bleeding. Moreover it cannot be used in patients with severe limb ischemia that require immediate recanalization due to the longer procedural time [14]. Percutaneous aspiration thrombectomy and percutaneous mechanical thrombectomy are efficient methods for transluminal removal of thrombus but they are associated with high risk for distal embolization (up to 28%), and they also require larger sheaths, which can lead to puncture-site complications (hematoma, dissection) [12].
Reperfusion injury is a common complication after revascularization which can lead to rapid development of compartment syndrome. In this case, surgical fasciotomy is necessary to prevent irreversible neurologic and muscular damage [3]. ALLI despite recent advancements in treatment strategies continues to confer significant risks for patients’ limb and life, and since currently available surgical or endovascular strategies are not without adverse events and contraindications, there is an obvious necessity for new techniques to be developed.
In this study, we present long-term results in patients with acute arterial occlusions who were treated with direct stenting (stent placement without predilatation of the lesion).
Materials and Methods
Study Design and Patient Selection
This is an observational, retrospective, single-center study aiming to examine efficacy of direct stenting to treat patients presenting with ALLI. Approval was obtained from our institutional review board to conduct this retrospective study. According to local treatment protocols and in accordance to international guidelines, patients presenting with SVS/ISCVS III ALLI (irreversible ischemia) were subjected to primary amputation. Those with SVS/ISCVS I, IIa, and IIb (viable, marginally, and immediately threatened limbs, respectively) were initially subjected to computed tomography (CT) imaging, and the subsequent management was determined on a consensus between vascular surgeons and interventional radiologists. 24-hour availability of the interventional radiology unit allowed for the alternative of the endovascular treatment to be available even for patients with immediately threatened limbs. Patients were allocated to treatment with direct stenting technique according to the following selection criteria:
-
1.
Compromised patients with ASA score class III or IV who are not ideal candidates for surgery
-
2.
Native artery occlusion (ALLI due to graft thrombosis excluded)
-
3.
Contraindication for administration of thrombolytic agents
-
4.
At least one tibial vessel runoff in the CTA
Patient Data: Clinical Information (Table 1)
From January 2010 to September 2015, 120 patients were diagnosed with ALLI at our institution. Among those, 16 patients (11 men and 5 women), aged between 52 and 93 years (median age 72.5 years), underwent direct stenting of acute arterial occlusions. In all patients, the duration of symptoms was less than 2 weeks with a mean duration of 2 days. Categorized in SVS/ISCVS Classification of ALLI, six patients were allocated to class IIa with minimal sensory deficit but no motor deficit and ten patients were allocated to class IIb with sensory deficit and mild to moderate motor deficit. Arterial doppler signal at the level of the malleolus was not detected in the affected limbs of all patients. The affected limbs could be salvageable if immediate revascularization took place.
The main risk factors were hypertension (n = 10), hyperlipidemia (n = 8), diabetes mellitus (n = 9), atrial fibrillation (n = 4), smoking (n = 6), previous acute myocardial infarction or ischemic stroke (n = 4), and previous endovascular or surgical procedure (n = 5).
All patients underwent lower extremity CT angiography (CTA) which revealed occlusions in CIA (n = 5), EIA (n = 7), SFA (n = 6), or POPA (n = 4) taking into consideration that some patients had more than one occlusion. In 12 patients, the cause of ALLI was assumed acute in situ thrombosis in a pre-existing atherosclerotic occlusion while in four patients embolism from the heart. The patients were considered as high risk for surgery due to multiple comorbidities so they were transferred to the interventional radiology suite for endovascular recanalization. Catheter-directed thrombolysis was not considered as a treatment option either because it was contraindicated (history of previous intracranial hemorrhage, recent eye surgery, recent intracranial trauma, diabetic hemorrhagic retinopathy, recent gastrointestinal bleeding) or the severity of limb ischemic symptoms was such that prompted immediate revascularization. Availability of percutaneous mechanical thrombectomy catheters is intermittent in our institute, and there was lack of these devices during treatment of the patients included in our study.
Procedural Details
Percutaneous common femoral arterial access was performed under real time U/S guidance. Depending on ipsilateral antegrade or contralateral retrograde approach, 5–6F vascular sheaths of variable lengths were inserted with their tip close to the occluded segment.
Our typical treatment strategy is to initially attempt crossing the occluded segment intraluminally using a 0.035 in. straight or curved hydrophilic guide wire (Terumo, Japan) supported by a standard 5F straight or curved catheter. In all patients, the occlusions were easily traversed intraluminally with straight type hydrophilic guide wires, a sign strongly predicting the presence of soft thrombus. Subsequently, self-expanding nitinol stents (Complete, Medtronic), (Luminexx, Bard), (Maris, Medtronic), (Sinus-SuperFlex, OptiMed), (Zeus SX, Rontis Medical) (Protege Everflex, Covidien) were deployed across the lesions. The selection of the self-expanding nitinol stent was based on the availability of the desired stent (diameter and length) in our department at that time. Deployment of a single long stent was preferred over implantation of multiple overlapping stents. Routinely, self-expanding nitinol stents should be 1–2 mm greater than the artery diameter. In our cases, the stent diameter was selected to be similar to the vessel diameter as it was measured before and after the occluded segment to prevent clot prolapse. As far as the stent length, it was about 20 mm longer than the lesion (10 mm proximal and 10 mm distal to the occlusion) to avoid thrombus relocation through both stent ends. Post-dilatation was performed only if there was more than 30% residual stenosis using slightly undersized angioplasty balloons at low pressures to avoid laceration and dislodgement of thrombus which could cause distal embolization. Apart from that the thermal memory of self-expanding nitinol stents would allow them to expand at the beneficial size.
The patients received a bolus of 5000 IU of heparin intra-arterially during the procedure. After the endovascular procedure, anticoagulant and antiplatelet therapy was important not only to obtain patency but to prevent recurrence. Patients with emboli of cardiac origin were placed on long-term anticoagulation with warfarin (INR: 2–3). Patients with non-embolic local arterial thrombosis received dual antiplatelet therapy including clopidogrel (75 mg once daily) and aspirin (100 mg once daily) for 1 month and then aspirin (100 mg once daily) indefinitely.
Endpoints
Primary endpoints of the analysis were efficacy measures of 30-day and long-term survival as well as 30-day and long-term limb salvage rate. Secondary outcomes that were assessed included procedural details like technical success, contrast administration, as well as safety measures like complication rate and distal embolization during the procedure. Reperfusion injury and need for fasciotomy were recorded. Patients were followed up with clinical examination at 1, 3, 6, and 12 months and color Doppler ultrasound combined with clinical examination on an annual basis. Patency and reintervention rates were also calculated.
Statistical Analysis
Statistical analysis was performed with GraphPad Prism 5.0 (GraphPad Software, Inc., San Diego, CA). Amputation-free survival and overall survival were evaluated using Kaplan–Meier statistics. Amputation-free survival is a composite metric which incorporates the hard endpoints of mortality and major amputation. Toe and distal foot amputations were considered minor amputations.
Results
Procedural Details: Outcome Measures (Table 2)
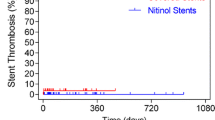
Recanalization was technically successful in all patients. There were no significant residual stenoses in the stented segments and there was neither distal embolization nor acute in-stent thrombosis, as it confirmed with the final angiography (Figs. 1, 2). There were no complications related to femoral arterial catheterizations such as hematomas, pseudoaneurysms, or arteriovenous fistulas. In 15 of 16 patients, there was a significant clinical improvement with immediate relief of symptoms. After the procedure, 14/16 patients restored palpable pedal pulses, while median post-procedural ABI was 0.8 (range 0.2–1.1). During the first week after the procedure, there was one case of in-stent thrombosis followed by above-knee amputation. The patients were followed up with clinical examination and color Duplex ultrasonography for a mean duration period of 37.6 months (SD 24.9 months, range 1–72). During follow-up, four patients died due to non-procedure-related causes (colon cancer, breast cancer, myocardial infarction, ischemic stroke) and there were two minor (toe) amputations and one major (above-knee) amputation. The amputations took place during the first year after the procedure. The 1-, 3- and 6-year survival rates, estimated by Kaplan–Meier analysis, were 93.3% [95% confidence interval (CI) 61.2–99%], 77.8% (95% CI 45.5–92.3%), and 69.1% (95% CI 36.7–87.3%), respectively, and the 1-, 3- and 6-year Amputation-free survival rates were 87% (95% CI 57.3–96.6%), 71.2% (95% CI 39.8–88.2%), and 62.3% (95% CI 31–82.6%), respectively (Fig. 3). The primary patency rate (defined as exempt from in-stent-restenosis greater than 50%) was 93.7% (95% CI 63.2–99.1%) at 1 year, 85.9% (95% CI 54–96.3%) at 2 years, and 75.2% (95% CI 39.4–91.6%) at 3 to 6 years (Fig. 4). No reperfusion injury was observed in this series and fasciotomy was not necessary in any of the patients treated.

A 80-year-old patient with atrial fibrillation. A DSA showed total occlusion of left CIA and left EIA. B Through percutaneous crossover approach from the right common femoral artery, the acute occlusion was traversed with a hydrophilic guide wire. Note the left CIA filling defect in the proximal end of the occlusion (arrow), typical for acute thrombus. C A self-expanding 7 × 200 mm nitinol stent was deployed across the lesion and D flow restoration was immediately achieved without distal embolization or other complications. E, F 4 years later the patient was asymptomatic. On color Duplex follow-up, the stented segment and distal runoff arteries remained patent with no significant restenosis

A 91-year-old patient with right acute lower limb ischemia. A DSA showed a thrombotic occlusion of the right popliteal artery with a small intraluminal filling defect in the distal end of the occlusion (arrow) consistent with the presence of fresh thrombus. B The occlusion was intraluminally traversed with a hydrophilic guide wire. C Following the implantation of a 6 × 60 mm self-expanding nitinol stent, DSA demonstrated significant flow restoration. D Conclusion DSA showed no evidence of distal embolization in the distal runoff arteries

The survival curves (±95% confidence interval) were calculated by Kaplan–Meier method. The x-axis shows months of follow-up, the y-axis shows proportion of patients remaining alive (A) or alive without major amputation (B). The number of patients at risk is indicated for each time point during follow-up

Kaplan–Meier curve of primary patency (±95% confidence interval) after stent placement. The number of patients at risk for each follow-up period is also indicated
Discussion
Acute limb ischemia is a sudden decrease in limb perfusion that threatens the viability of the extremity and requires immediate revascularization.
Stenting has been used successfully in acute myocardial infarction after failed thrombolysis [19] or after unsuccessful emergency angioplasty [20] but is also an effective primary revascularization strategy with many advantages compared with PTCA [21]. Primary intracranial stenting is also a safe and feasible approach for patients with acute ischemic stroke [22, 23]. Moreover, primary or direct stenting is an acceptable revascularization treatment for peripheral artery disease [1]. It is effective both for iliac artery occlusive disease [24] and femoropopliteal disease [25]. Direct stenting is not considered as a standard treatment option for ALLI due to a risk of distal embolization, which worsens the ischemia. So far there are only a few reports of patients with ALLI treated with stenting. Yilmaz et al. treated six patients with embolic occlusions in the common or external iliac arteries with primary stenting without complications [26]. Berczi et al. reported seven patients with acute thrombotic occlusions in the iliac arteries, who underwent stent implantation with no significant embolic complications [27]. Raja et al. reviewed 4 patients with acute thrombotic or embolic occlusions in iliac or femoropopliteal arteries who were treated with stenting [28]. Finally Kim et al. treated fifteen patients with ALLI with stent implantation with significant technical and clinical success [29].
Our study includes the largest number of patients with ALLI, treated with primary or direct stenting (n = 16) and the longest follow-up (mean duration of about 3 years), which confirms a sustainable clinical improvement and low risk for amputation. In our study, we applied direct stenting as a primary endovascular treatment due to unavailability of percutaneous mechanical thrombectomy catheters at the time of cases presentation, while catheter-directed thrombolysis was either contraindicated or was considered too time consuming for immediate limb revascularization. Our findings indicate that direct stenting is an attractive therapeutic alternative for the management of patients with ALLI whenever feasible. The 100% technical success rate recorded in our study cohort compares favorably with the results of other reports employing the traditional and widely accepted techniques of catheter-directed thrombolysis and percutaneous mechanical thrombectomy. Furthermore, we neither encountered puncture-site complications nor distal embolization which confirms the safety of this technique in patients with ALLI. From our clinical experience, immediate recanalization of acute arterial occlusions with direct stenting did not induce compartment syndrome or systemic inflammatory response triggered by reperfusion injury in any patients at least to an extent that needed any further concomitant treatment. We used only self-expanding nitinol stents to avoid laceration and dislodgement of thrombus and reduce the traumatic injury of the vessel. Drug-eluting stents (DES) improve patency rates and reduce the risk of reintervention compared with PTA or bare-metal stents (BMS) in atherosclerotic disease of femoral, popliteal [30], and infrapopliteal arteries [31]. However, there are no reported cases of the use of DES in ALLI. Stents in the femoropopliteal system and especially if the lesions expanded in the inguinal ligament or knee joint have historically been associated with increased rate of stent fracture and restenosis. Modern self-expanding nitinol stents with their resistance to external deformation and their thermal memory properties are sometimes indicated for placement in areas of flexion (close to the inguinal ligament, in the adductor canal and at the knee joint) [32]. Multiple studies have reported the use of flexible self-expanding nitinol stents in the popliteal artery and lesions which were extended into the below-knee segment with good patency rates [33]. In our study, we avoided stent placement when the lesion crossing joints and there was only one patient (Fig. 2) who underwent direct stenting of popliteal artery occlusion crossing the knee joint. This patient was 90-year-old, presenting multiple comorbidities and was partially immobilized for 2 years. Therefore, he was a poor surgical candidate presenting also contraindication for catheter-directed thrombolysis. In this instance, direct stenting seemed an appealing therapeutic option even if the stent would be crossing the knee joint. Despite the fact that the lesions observed in this series were relatively long, technical success was achieved in all patients. Other authors who performed direct stenting for ALLI encountered similar long arterial occlusions (up to 150 mm) [26–29]. All stents deployed in the studied patients were commercially available self-expanding nitinol ones with different strut configuration and it would be interesting to analyze in larger cohort studies the potential influence of strut design to overall nitinol stent performance in the ALLI setting.
In conclusion, direct stenting appears to be a safe, effective, and durable treatment for patients with ALLI who require immediate recanalization and they have contraindications for catheter-directed thrombolysis or surgical revascularization.
References
Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33(Suppl 1):S1–75. doi:10.1016/j.ejvs.2006.09.024.
Kasirajan K, Ouriel K. Current options in the diagnosis and management of acute limb ischemia. Prog Cardiovasc Nurs. 2002;17(1):26–34.
Creager MA, Kaufman JA, Conte MS. Clinical practice. Acute limb ischemia. N Engl J Med. 2012;366(23):2198–206. doi:10.1056/NEJMcp1006054.
Patel N, Sacks D, Patel RI, Moresco KP, Ouriel K, Gray R, et al. SIR reporting standards for the treatment of acute limb ischemia with use of transluminal removal of arterial thrombus. J Vasc Interven Radiol. 2003;14(9 Pt 2):S453–65.
Walker TG. Acute limb ischemia. Techniques Vasc Interven Radiol. 2009;12(2):117–29. doi:10.1053/j.tvir.2009.08.005.
Earnshaw JJ, Whitman B, Foy C. National audit of thrombolysis for acute leg ischemia (NATALI): clinical factors associated with early outcome. J Vasc Surg. 2004;39(5):1018–25. doi:10.1016/j.jvs.2004.01.019.
Yeager RA, Moneta GL, Taylor LM Jr, Hamre DW, McConnell DB, Porter JM. Surgical management of severe acute lower extremity ischemia. J Vasc Surg. 1992;15(2):385–91 discussion 92–3.
Berridge DC, Kessel DO, Robertson I. Surgery versus thrombolysis for initial management of acute limb ischaemia. Cochrane Database Syst Rev. 2013. doi:10.1002/14651858.CD002784.pub2.
Graor RA, Comerota AJ, Douville Y, Turpie AG, Froehlich J, Hosking JD, et al. Results of a prospective randomized trial evaluating surgery versus thrombolysis for ischemia of the lower extremity. The STILE trial. Ann Surg. 1994;220(3):251–66 discussion 66–8.
Taha AG, Byrne RM, Avgerinos ED, Marone LK, Makaroun MS, Chaer RA. Comparative effectiveness of endovascular versus surgical revascularization for acute lower extremity ischemia. J Vasc Surg. 2015;61(1):147–54. doi:10.1016/j.jvs.2014.06.109.
Ouriel K. Endovascular techniques in the treatment of acute limb ischemia: thrombolytic agents, trials, and percutaneous mechanical thrombectomy techniques. Semin Vasc Surg. 2003;16(4):270–9.
Morgan R, Belli AM. Percutaneous thrombectomy: a review. Eur Radiol. 2002;12(1):205–17. doi:10.1007/s003300101014.
Kashyap VS, Gilani R, Bena JF, Bannazadeh M, Sarac TP. Endovascular therapy for acute limb ischemia. J Vasc Surg. 2011;53(2):340–6. doi:10.1016/j.jvs.2010.08.064.
Karnabatidis D, Spiliopoulos S, Tsetis D, Siablis D. Quality improvement guidelines for percutaneous catheter-directed intra-arterial thrombolysis and mechanical thrombectomy for acute lower-limb ischemia. Cardiovasc Interven Radiol. 2011;34(6):1123–36. doi:10.1007/s00270-011-0258-z.
Zambouri A. Preoperative evaluation and preparation for anesthesia and surgery. Hippokratia. 2007;11(1):13–21.
Morris-Stiff G, D’Souza J, Raman S, Paulvannan S, Lewis MH. Update experience of surgery for acute limb ischaemia in a district general hospital—are we getting any better? Ann R Coll Surg Engl. 2009;91(8):637–40. doi:10.1308/003588409X12486167521271.
Ouriel K, Shortell CK, DeWeese JA, Green RM, Francis CW, Azodo MV, et al. A comparison of thrombolytic therapy with operative revascularization in the initial treatment of acute peripheral arterial ischemia. J Vasc Surg. 1994;19(6):1021–30.
van den Berg JC. Thrombolysis for acute arterial occlusion. J Vasc Surg. 2010;52(2):512–5. doi:10.1016/j.jvs.2010.01.080.
La Vecchia L, Favero L, Martini M, Vincenzi P, Rubboli A, Ottani F, et al. Systematic coronary stenting after failed thrombolysis in high-risk patients with acute myocardial infarction: procedural results and long-term follow-up. Coron Artery Dis. 2003;14(5):395–400. doi:10.1097/01.mca.0000085136.16622.33.
Steffenino G, Dellavalle A, Ribichini F, Uslenghi E. Coronary stenting after unsuccessful emergency angioplasty in acute myocardial infarction: results in a series of consecutive patients. Am Heart J. 1996;132(6):1115–8.
Mehta RH, Bates ER. Coronary stent implantation in acute myocardial infarction. Am Heart J. 1999;137(4 Pt 1):603–11.
Velat GJ, Hoh BL, Levy EI, Mocco J. Primary intracranial stenting in acute ischemic stroke. Curr Cardiol Rep. 2010;12(1):14–9. doi:10.1007/s11886-009-0069-x.
Samaniego EA, Dabus G, Linfante I. Stenting in the treatment of acute ischemic stroke: literature review. Front Neurol. 2011;2:76. doi:10.3389/fneur.2011.00076.
Tsetis D, Uberoi R. Quality improvement guidelines for endovascular treatment of iliac artery occlusive disease. Cardiovasc Intervent Radiol. 2008;31(2):238–45. doi:10.1007/s00270-007-9095-5.
Mewissen MW. Primary nitinol stenting for femoropopliteal disease. J Endovasc Ther. 2009;16(2 Suppl):63–81. doi:10.1583/08-2658.1.
Yilmaz S, Sindel T, Luleci E. Primary stenting of embolic occlusions in iliac arteries. J Endovasc Ther. 2003;10(3):629–35. doi:10.1583/1545-1550(2003)010<0629:PSOEOI>2.0.CO;2.
Berczi V, Thomas SM, Turner DR, Bottomley JR, Cleveland TJ, Gaines PA. Stent implantation for acute iliac artery occlusions: initial experience. J Vasc Interven Radiol. 2006;17(4):645–9. doi:10.1097/01.RVI.0000203918.91835.73.
Raja J, Munneke G, Morgan R, Belli AM. Stenting in acute lower limb arterial occlusions. Cardiovasc Interven Radiol. 2008;31(2):S41–4. doi:10.1007/s00270-007-9052-3.
Kim C, Jeon W, Shin T, Choi D, Kim J, Lee C, et al. Stent-assisted recanalisation of acute occlusive arteries in patients with acute limb ischaemia. Eur J Vasc Endovasc Surg. 2010;39(1):89–96. doi:10.1016/j.ejvs.2009.09.023.
Dake MD, Ansel GM, Jaff MR, Ohki T, Saxon RR, Smouse HB, et al. Durable clinical effectiveness with paclitaxel-eluting stents in the femoropopliteal artery: 5-year results of the zilver ptx randomized trial. Circulation. 2016;133(15):1472–83. doi:10.1161/CIRCULATIONAHA.115.016900 discussion 83.
Fusaro M, Cassese S, Ndrepepa G, Tepe G, King L, Ott I, et al. Drug-eluting stents for revascularization of infrapopliteal arteries: updated meta-analysis of randomized trials. JACC Cardiovasc Interven. 2013;6(12):1284–93. doi:10.1016/j.jcin.2013.08.007.
Katsanos K, Tepe G, Tsetis D, Fanelli F. Standards of practice for superficial femoral and popliteal artery angioplasty and stenting. Cardiovasc Interven Radiol. 2014;37(3):592–603. doi:10.1007/s00270-014-0876-3.
Bishu K, Armstrong EJ. Supera self-expanding stents for endovascular treatment of femoropopliteal disease: a review of the clinical evidence. Vasc Health Risk Manag. 2015;11:387–95. doi:10.2147/VHRM.S70229.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflicts of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Galanakis, N., Kontopodis, N., Peteinarakis, I. et al. Direct Stenting in Patients with Acute Lower Limb Arterial Occlusions: Immediate and Long-Term Results. Cardiovasc Intervent Radiol 40, 192–201 (2017). https://doi.org/10.1007/s00270-016-1500-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-016-1500-5