
Abstract
Adventitial cystic disease (ACD) of the popliteal artery is an uncommon vascular condition of unknown etiology. In the present case report, we describe a case of bilateral ACD of the popliteal artery in a 58-year-old male. To the best of our knowledge, this is the first case of bilateral ACD of the popliteal artery reported in the literature.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Adventitial cystic disease (ACD) of the popliteal artery is an uncommon vascular condition of unknown etiology. ACD is more frequent in young and middle-age males and it can cause progressive claudication due to compression of the arterial lumen by a mucin-containing cyst localized in the adventitial layer of the artery. In the present case report, we describe a case of bilateral ACD of the popliteal artery in a 58-year-old male on whom ultrasound (US), angiography, computed tomography (CT), and magnetic resonance imaging (MRI) were performed. To the best of our knowledge, this is the first case of bilateral ACD of the popliteal artery reported in the literature.
Case Report
A 58-year-old man presented with a 6-month history of progressive severe claudication. The patient had a positive history of cigarette smoking for the past 8 years and a negative history of hypertension or hyperlipidemia. Physical exam demonstrated no neurological abnormalities or skin ulcers; the femoral pulses were normal; there were absent popliteal pulses and diminished dorsalis pedis and posterior tibial pulses bilaterally. The ankle-brachial indexes (ABIs) were 0.58 and 0.57 at the right and left sides, respectively.
An extrainstitutional initial US examination suggested the diagnosis of bilateral popliteal aneurysms. Selective arteriography was performed, which showed mild diffuse atherosclerotic changes throughout both superficial femoral arteries, with a short segment of occlusion on the distal third of the left superficial femoral artery (SFA) with immediate distal reconstitution. There were bilateral popliteal artery occlusions with distal reconstitution via collaterals (Fig. 1). Although the angiographic findings suggested atherosclerotic disease, a computed tomography angiography (CTA) was performed to rule out thrombosed popliteal aneurysms, as suggested by the previous US.

A Arteriography with digital substraction of the right lower extremity. Anterior–posterior projection. Abrupt occlusion at the junction of the proximal and mid portion of the popliteal artery (arrows) is seen with distal reconstitution via collaterals. B Arteriography with digital substraction of the left lower extremity. Anterior–posterior projection. Observe tappering of the vascular lumen (arrowheads) and occlusion at the mid popliteal artery (arrows) with distal reconstitution via collaterals.
Computed tomography angiography showed multiple hypodense cysticlike masses with thin enhancing rims and nonenhancing centers in both popliteal fossae, with occlusion of both popliteal arteries (Fig. 2). The diagnosis of bilateral ACD of the popliteal arteries was made. A second US examination with a Doppler mode was performed showing hypoechoic cystic lesions with well-defined margins and posterior acoustic enhancement. Some of the cysts had multiple septated hypoechoic spaces with thin walls (Fig. 3). There was absence of flow on both popliteal arteries, with monophasic continuous waves in the dorsalis pedis and posterior tibial arteries bilaterally.

Axial computed tomography with intravenous contrast medium at the level of the femoral condyles. A Right popliteal fossa. Note multiple hypodense cysticlike masses with a thin enhancing rim and nonenhancing center (arrowheads). There is occlusion of the popliteal artery (curve arrow). Note patent popliteal vein (straight arrow). B Left popliteal fossa. Observe multiple hypodense cysticlike masses (arrowheads), with a thin enhancing rim and nonenhancing center. Occlusion of the popliteal artery (curve arrow) and patent popliteal vein (straight arrow).

Gray-scale sonogram of both popliteal fossae. Sagittal (A) and transverse (B) planes of the right popliteal fossa. Note a hypoechoic cystic lesion with well-defined margins and posterior acoustic enhancement (arrowheads). Sagittal (C) and transverse (D) planes of the left popliteal fossa showing multiple septated hypoechoic spaces with thin walls (arrowheads). Note that the extension of the lesion is larger on the right side.
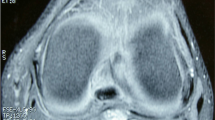
Magnetic resonance imaging and magnetic resonance arteriography (MRA) examinations were performed for educational purposes. Using fast spin-echo images with fat saturation, the MRI showed multiple lobulated cystic lesions adjacent to the wall of the popliteal arteries with homogeneous signal intensity. Homogeneous low T1- and high T2-weighted spin-echo signal intensities were observed on images with fat saturation (Fig. 4). Hypointense multilobulated cystic masses with enhancing septa and thin walls, without inner enhancement, were observed on postcontrast T1-weighted spin-echo images with fat saturation (Fig. 5). There were also severe bilateral tricompartmental degenerative changes in both knees. Incidental finding of a Baker’s cyst was noted in the left knee with no apparent communication with the adventitial cysts. MRA showed bilateral popliteal occlusion and also the short-segment occlusion of the distal left femoral superficial artery. Multiple collateral vessels around the left SFA occlusion and irregularity of the superficial femoral arteries bilaterally probably secondary to concomitant atherosclerotic disease were also noted (Fig. 6).

Axial (A) and sagittal (B) T2-weighted fast spin-echo images with fat saturation of the right knee. Note the multiple lobulated cystic lesions adjacent to the wall of the popliteal artery with homogeneous high signal intensity (arrowheads). The lesions are seen surrounding the popliteal artery and producing extrinsic compression of its lumen (curved arrow). Observe in the sagittal image the longitudinal extension of the lesion (arrowheads). Popliteal vein (straight arrow).

Postcontrast axial T1-weighted spin-echo image with fat saturation of the right knee. Hypointense multilobulated cystic mass with rim enhancing (arrowheads); there is no enhancement in the center of the lesions. There is no enhancing of the popliteal artery due to the occlusion (curve arrow). Note the normal enhancing of the popliteal vein (straight arrow).

Magnetic resonance arteriography; Coronal maximum intensity projection. Note the long segment occlusion of the right popliteal artery (arrowheads) with collaterals. On the left, observe the short segment occlusion of the distal left SFA (straight arrows) and of the left popliteal artery (arrowheads).
The patient underwent surgery on the right side initially and on the left leg 6 months later. Chronic thrombosis of the mid popliteal arteries was observed with multiloculated cysts and extensive inflammatory adhesions bilaterally. Excision of the multiple cysts was performed and a nonreversed saphenous vein bypass was interposed in both lower extremities. Palpable popliteal, dorsalis pedis, and posterior tibial pulses with normal sensation and motion were observed after the surgery. The patient presented with recurrent symptoms in the right leg 4 months after the initial surgery due to intimal hyperplasia of the distal bypass anastomosis that was successfully treated with balloon angioplasty. Th patient is currently asymptomatic in the last follow-up.
Discussion
Cases of ACD have been reported involving the external iliac, popliteal, femoral, radial, and ulnar arteries [1–6] and the external iliac, femoral and superficial veins [1, 7]. The incidence of ACD is 1 in 1000 femoral angiograms and 1 in 1200 cases of claudication [7, 8]. The ratio of males to females is 15:1 [7, 9]. The presenting age varies between the fifth (men) and sixth (women) decades of the life [7], although cases have been reported in other ages [8, 10].
The etiology of ACD is currently unclear. Four theories have been proposed: repetitive local trauma, abnormalities of the embryological development, ACD as part of a systemic disease, and the synovial hypothesis [4, 9, 11–14]. The synovial (or ganglion) and the abnormal embryological development are the most currently accepted theories [13]. The first one refers to the herniation of capsular synovial structures from the adjacent joint, along vascular branches, to form a ganglion or synovial cyst into the adventitial of the artery [13, 14]. This theory is based on the similar findings of ganglia and rich hyaluronic acid content of the adventitial cysts [14]. Leu et al. [1] believe that ACD is caused by a ganglion or bursalike ectopic tissue originating from scleroblastoma. Scleroblastoma is responsible for the formation of joint capsules and bursae. Both ganglia and Baker’s cysts might communicate with joints or with tendon sheaths. Cases of ACD with communication of the cyst with the adjacent knee joint and a Baker’s cyst have been described [14–16].
The embryological theory postulated like an unifying hypothesis explains the ACD as an error of development caused by incorporation of mesenchymal cells, destined to form joint tissue, into the developing nonaxial vessels. These less differentiated joint-related mesenchymal cells slowly produce mucoid material, which explains the later life symptomology [14].
The traumatic theory is unlikely because ACD can occur in children and is not frequent in athletes; also a past history of repetitive trauma is uncommon [1, 14]. ACD has not showed any consistent association with a systemic disease [14].
Histopathologically, ACD is a cystic collection filled with a gelatinous material that is crystal clear to yellowish in color depending of the degree of hemorrhage. The material is rich in mucoproteins and mucopolysaccharides. The cysts are located with tension between the adventitial and medial layers of the vessel wall [4, 7, 12, 13, 17]. These cysts can eventually compress the vascular lumen of the artery causing stenosis or occlusion. The compromise of the vascular lumen explains the clinical symptomology.
Adventitial cystic disease of the popliteal artery should be clinically suspected in an adult male patient, between the fourth and fifth decades of life, who presents with sudden onset of claudication in the lower extremities without significant evidence of atherosclerotic disease [4, 9, 11–13]. The symptoms typically worsen with flexion of the knee [12, 13]. If a direct communication of the adventitial cyst with the joint space or a Baker’s cyst exists, exercise or repetitive trauma can cause rapid growth of the cyst with accelerated progression of symptoms [1, 11, 16]. Spontaneous rupture of the cyst is a rare event and might result in relief of symptoms by decompression of the cyst [12, 17]. The recurrence after spontaneous rupture might depend on the extension of the perforation in the wall of the cyst [17]. ACD is classically a unilateral process. Bilateral popliteal involvement has not been reported previously [18].
When ACD involves the popliteal artery, stenosis is more common than occlusion. Arterial occlusion has been observed in 30% of patients [19]. A classical clinical finding is the Ischikawa sign; the popliteal and pedal pulses are normal in a neutral position but diminish or disappear during flexion of the knee [11, 13, 20]. Generally, it is not possible to feel the cyst on physical exam, but sometimes ACD can present as soft-tissue-like masses involving the extremities and causing confusion with a slowly growing soft tissue tumor [14, 21].
The differential diagnoses of popliteal artery disease in a young to middle-aged patient with progressive and intermittent claudication, with nonatherosclerotic disease include the following: popliteal artery entrapment syndrome, ACD, popliteal aneurysm (trombosed or not), thromboangiitis obliterans (Buerger’s disease), secondary embolism, hematoma, or Baker cyst producing entrapment [4, 11, 12, 22].
Clinical history with physical exam plus an US examination is usually enough to establish a diagnosis of ACD. US is readily available and inexpensive. A gray-scale sonogram demonstrates hypoechoic cystic lesions with or without multiple septated hypoechoic spaces. Doppler US clearly shows the stenosis with turbulent flow or arterial occlusion with absent color flow. An intra-arterial sonogram shows a large cystic mass arising from adventitia of the vessel [18, 21].
Arteriography has been regarded as the gold standard, but it is diagnostic only when the study shows characteristics findings such as the scimitar or the hourglass signs produced by the eccentric or concentric compression [4, 11, 12]. However, in many cases when the angiographic findings are not typical or there is popliteal artery occlusion, arteriography is not conclusive and other imaging studies are required [4]. Other disadvantages of the arteriography include the high cost, invasiveness, and radiation exposure.
Computed tomography and MRI are excellent diagnostic tools that can accurately depict the anatomy of the popliteal fossae, showing the cystic lesions and their relationships to the vessels [7, 9, 11, 12, 22–24]. Additionally, MRA and CTA can noninvasively demonstrate the arterial stenosis or occlusion and also determine the inflow and the distal runoff of the arterial segments [9, 12, 25].
In this case report, our patient presented with both atherosclerotic disease and bilateral ACD. The imaging findings demonstrated multiple bilateral popliteal cysts with occlusion of both popliteal arteries; there was extensive involvement with multiple cysts. During surgery, extensive inflammatory reaction and extrinsic compression over the popliteal arteries was demonstrated.
The classical therapy of ACD has been surgery [24]. The two surgical options are the evacuation with excision of the wall cysts and bypass grafting [11–13, 18, 26]. If the cyst has communication with the joint space, surgical treatment is indicated [11]. Complete evacuation with excision of the wall cyst and conservation of the medial and intimal layers is the preferred surgical technique [13, 24], but this has a relapse rate of about 10% [18, 27]. Bypass grafting is indicated in cases of complete arterial occlusion if the arterial wall is weakened or if secondary intimal ulceration has occurred [9, 11, 12, 24]. The prognosis is good after bypass grafting [4, 7, 9, 12–14, 25, 26].
Several reports on US- and CT-guided percutaneous cyst aspiration for the treatment of ACD have shown encouraging initial results [11–13, 23, 24]. The clinical success with percutaneous aspiration depends on the quality of the cysts content. Highly mucinous and gelatinous content will be difficult to aspirate. Percutaneous aspiration is an alternative for patients who do not have thrombotic occlusion; unfortunately, the recurrence after aspiration is common [7, 9, 14, 17]. Percutaneous transluminal angioplasty (PTA) is not indicated because the stenosis is caused by an extrinsic compression and the intima of the vessel in ACD is normal and, therefore, compliant [7]. Furthermore, cyst contents are not compressible and cyst rupture might result in an untoward result.
References
Leu HJ, Largiader J, Odermatt B (1984) Pathogenesis of the so-called cystic adventitial degeneration of peripheral blood vessels. Virchows Arch 404:289–300
Atkins H, Key J (1947) A case of myxomatous tumor arising in the adventitia of the left external iliac artery. Br J Surg 34:426–427
Ejrup B, Hiertonn T (1954) Intermittent claudication: three cases treated by free vein graft. Acta Chir Scand 108:217–230
Velasquez G, Zollikofer C, Nath H, et al. (1980) Cystic arterial adventitial degeneration. Radiology 134:19–21
Bäckström CG, Linell F, Ostberg G (1965) Cystic, myxomatous adventitial degeneration of the radial artery with development of ganglion in the connective tissue. Report of two cases. Acta Chir Scand 129:447–451
Flanigan D, Burnham S, Goodreau J, (1979) Summary of cases of adventitial cystic disease of the popliteal artery. Ann Surg 189:165–175
Bergan J (1995) Adventitial cystic disease of the popliteal artery. In: Rutherford RB (ed) Vascular Surgery, 4th ed. WB Saunders. Philadelphia, pp 883–887
Lewis GJT, Douglas DM, Reid W, et al. (1967) Cystic adventitial disease of the popliteal artery. Br Med J 3:411–415
Miller A, Salenius JP, Sacks BA, et al. (1997) Noninvasive vascular imaging in the diagnosis and treatment of adventitial cystic disease of the popliteal artery. J Vasc Surg 26:715–720
DeLaurentis DA, Wolferth CC Jr, Wolf FM, et al. (1973) Mucinous adventitial cysts of the popliteal artery in an 11-year-old girl. Surgery 74:456–459
Sys J, Michielsen J, Bleyn J, (1997) Adventitial cystic disease of the popliteal artery in a triathlete. a case report. Am J Sports Med 25(6):854–857
Ricci P, Panzetti C, Mastantuono M, et al. (1999) Cross-sectional imaging in a case of adventitial cystic disease of the popliteal artery. Cardiovasc Intervent Radiol 22(1):71–74
Papavassiliou VG, Nasim A, Awad EM, (2002) Adventitial cystic disease of the popliteal artery: diagnosis and treatment. A case report. J Cardiovasc Surg 43:399–401
Levien LJ, Benn CA (1998) Adventitial cystic disease: a unifying hypothesis. J Vasc Surg 28:193–205
Unno N, Kaneko H, Uchiyama T, et al. (2000) Cystic adventitial disease of the popliteal artery: elongation into the media of the popliteal artery and communication with the knee joint capsule: report of a case. Surg Today 30(11):1026–1029
Schroё H, Van Opstal C, De leersnijder J, et al. (1988) Baker’s cyst connected to popliteal artery cyst. Ann Vasc Surg 2(4):385–389
Lossef SV, Rajan S, Calcagno D, et al. (1992) Spontaneous rupture of an adventitial cyst of the popliteal artery: confirmation with MR imaging. J Vasc Intervent Radiol 3:95–97
Landry G, Abou-Zamzam A, Edwards J, et al. (2002) Nonatherosclerotic vascular disease. In: Moore WS (ed) Vascular Surgery. A Comprehensive Review, 6th ed. WB Saunders. Philadelphia, pp 143–144
Bunker SR, Lauten GJ, Hutton JE (1981) Cystic adventitial disease of the popliteal artery. Am J Roentgenol 136:1209–1212
Ikeda M, Fujimori Y, Tankawa H, (1984) Compression syndrome of the popliteal vein and artery caused by popliteal cyst. Angiology 35(4):245–251
Peterson JJ, Kransdorf MJ, Bancroft LW, et al. (2003) Imaging characteristics of cystic adventitial disease of the peripheral arteries: presentation as soft-tissue masses. Am J Roentgenol 180:621–625
Elias DA, White LM, Rubenstein JD, et al. (2003) Clinical evaluation and MR imaging features of popliteal artery entrapment and cystic adventitial disease. Am J Roentgenol 180:627–632
Comerota AJ (1995) Vascular imaging techniques. In: Rutherford RB (ed) Vascular Surgery, 4th ed. WB Saunders. Philadelphia, p 137
Do DD, Braunschweig M, Baumgartner I, et al. (1997) Adventitial cystic disease of the popliteal artery: percutaneous US-guided aspiration. Radiology 203:743–746
Rückert RI, Taupitz M (2000) Cystic adventitial disease of the popliteal artery. Am J Surg 180(1):53
Fox CJ, Rasmussen TE, O’Donnell SD (2004) Cystic adventitial disease of the popliteal artery. J Vasc Surg 39:1351
Lazic V, Stierli P (1994) Adventitia resection in cystic degeneration of the popliteal artery. Helv Chir Acta 60(6):883–886
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ortiz M., W.R., Lopera, J.E., Giménez, C.R. et al. Bilateral Adventitial Cystic Disease of the Popliteal Artery: A Case Report. Cardiovasc Intervent Radiol 29, 306–310 (2006). https://doi.org/10.1007/s00270-004-0300-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-004-0300-5