
Abstract
Introduction
Different outcomes in breast cancer have been reported for low and high socio-economic groups. We present data quantifying disparities between South African public and private patients.
Methods
Records of 240 consecutive patients treated in 2008 in a public versus 97 patients in a private health facility were reviewed for demographic and oncologic data.
Results
The average of patients was 56.2 versus 51.9 years (p = 0.032). Stage at presentation was 0 in 0.83 versus 25.8%, I in 4.5 versus 15.5%, II in 41.3 versus 37.1%, III in 37.1 versus 18.6% and IV in 16.3 versus 3.1% public versus private patients. Seventy-three percent of patients were symptomatic versus 57.7%. Of patients with stage 0–III disease, 17.9 versus 20% had simple tumour excision and 7.5 versus 14%, oncoplastic tumour excision. The mastectomy rate was similar (52 vs. 60%), but immediate reconstruction was performed in 10 versus 63%. Public patients were less likely to have radiotherapy. The pathology was similar, 27.2 versus 20, 54 versus 52, 87 versus 61% of patients with stage I, II and III disease, respectively, had chemotherapy. Hormonal therapy for premenopausal patients in private was a LHRH agonist in 9.3%, ovarian ablation/BSO in 11.7% of public patients; biologicals were given in 7.2 versus 0% of patients. Overall survival for public versus private was 66 versus 80% (p < 0.001) months. Better per stage survival of private patients 100 versus 100, 72.7 versus 93.3, 84.8 versus 88.9, 57.3 versus 77.8 and 33 versus 33% for stages 0, I, II, III and IV, did not reach statistical significance.
Conclusion
The greatest impact on outcome was stage at presentation, but more aggressive therapy for each stage resulted in a trend to better outcome for private patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the most common cause of cancer death in females globally [1]. This also is true for South Africa [2]. The outcome of breast cancer has been documented to differ between socio-economic groups in the developed world [2, 3]. This disparity has been attributed only in part to later stage at diagnosis in poorer socio-economic groups [4] and also holds true for other types of cancer with a relative risk of death 1.3–1.5 in deprived groups [5, 6]. There is a paucity of similar data for developing countries [3]. South Africa has a Gini coefficient much higher than most of the countries where data linking cancer outcomes in relation to socio-economic factors have been reported [7]. In such an extremely unequal society, factors reflecting socio-economic deprivation other than stage at diagnosis may be amplified. We here compare the outcome of breast cancer between a resource rich and resource poor environment in an African setting.
Methods
An analysis was performed of prospectively collected records of consecutive patients treated for breast cancer at a private and public hospital in the Western Cape Province of South Africa, during the period January 2008–December 2008. Data were compiled in a Microsoft Access database (Microsoft Corporation, Redmond, WA, USA) and included demographical, clinical and histopathological data; treatments administered, compliance and oncologic outcomes as reflected in Table 1. No data regarding the ethnicity of patients were gathered, as many of our patients are of “mixed-race” origin and the collection of data concerning ethnicity in a South African context has been questioned [8]. Staging was performed according to the AJCC/TNM staging manual [9]. Patients for whom clinical and pathological staging were unknown were excluded from analysis. No males were included in this study. Surgical treatment was performed according to the NCCN guidelines [10] and clinical staging. Adjuvant therapy was provided according to the “St Gallen” guidelines of 2007 [11], and neoadjuvant therapy according to the NSABP protocols B-18 and B-27 [12]. Survival and relapse rates were calculated according to the method described by Kaplan and Meier [13]. IBM SPSS version 23 (International Business Machines Corporation, Armonk, New York, USA) was used to analyse the data. A p value <0.05 was considered as statistically significant. Pearson’s chi-square tests [8] were used to compare categorical variables between groups. Kaplan–Meier time to event analysis was used to describe and compare survival between groups using a log-rank test.
The protocol was approved by the Ethics Committee of the University of Stellenbosch (HREC S15/10/240).
Results
Demographics
In 2008, 250 new patients were seen at the public and 106 patients at the private institution with newly diagnosed breast cancer. Of these, ten patients and nine patients, respectively, had no staging data and were excluded from analysis.
The average age was 56.2 years for public patients and 51.9 years for private patients (p = 0.032).
Presentation
Fifty-eight out of the 240 (25.6%) public patients presented for or after screening, whereas 41 out of 97 (42.3%) patients in the private sector presented for screening, or were screened elsewhere prior to presentation (Tables 2, 3).
There was a significant difference in the percentage of patients who presented for screening, and at what stage they were diagnosed in the public and private health sector groups (p < 0.01).
Treatments
Surgical treatment
Of the nine patients with stage II disease who did not have surgery, two were not offered surgical intervention due to severe systemic comorbidities, three were lost to follow-up, two died of other causes prior to surgery, one patient with c-erb B2-positive disease refused surgery and survived for 36 months on tamoxifen alone, and one patient was diagnosed by screening, refused any treatment and did not undergo any hormonal testing, and was last known to be alive with disease after 84 months with no therapy (Table 4).
Of the five patients with stage III disease who did not have any surgery, two patients refused surgical intervention, one patient died of unrelated causes whilst undergoing neoadjuvant chemotherapy, and two died of breast cancer within two months of diagnosis (Table 5).
The three of the four patients who are not known to have had surgery were lost to follow-up prior to commencement of therapy. One patient with stage III disease died before surgery could be undertaken. Patients from the private sector group were more likely to have breast reconstruction surgery than patients in the private sector (p value <0.001), whereas patients in the public sector were more likely to undergo mastectomy alone. Similar rates of tumour excision and oncoplastic surgery were seen in both groups.
Radiotherapy provided
In the public group classified as “other”, one patient each with stage I and stage II disease had ovarian radiation only, and another seven patients had palliative radiotherapy to symptomatic metastases in bone (Table 6).
In private, seven patients were lost to follow-up and are not known to have received radiotherapy (Table 7).
Chemotherapy provided
Six patients diagnosed with breast cancer in private were lost to follow-up prior to commencement of chemotherapy (Tables 8, 9).
No patients in the public sector had access to taxane-containing chemotherapy regimens. Totally, 19 patients in the private sector group received chemotherapy containing taxanes.
One patient in the public, and two patients in private, presented with stage 0 breast cancer and were found to be triple negative cancers (ER- , PR- and c-erb2 negative), and as such underwent systemic chemotherapy.
Of 13 patients with stage 0 or I disease in the public sector, four patients had chemotherapy because of nodal involvement in three and FISH-positive cancer in one case. Of 40 private patients with stage 0 and I disease, six received adjuvant chemotherapy; of these, three had triple negative cancers 1 cm or larger, one a high-risk tumour at molecular genetic profiling and one for high-grade tumours larger than 1-cm diameter that were endocrine only partially dependent.
Hormonal status and therapy
A total of 20 patients did not have hormonal receptor tests. Of these, nine had stage II, three stage III, five stage IV and three unknown staging that were initially treated and underwent surgery elsewhere. Of these patients, five are known to be alive with no evidence of disease (Table 10).
Out of the 40 premenopausal patients that had hormone receptor-positive disease, eight had bilateral salpingo-oophorectomies, 20 had ovarian ablation radiotherapy, three died of disease prior to starting therapy, one died of other causes, one is lost to follow-up, and six were peri-menopausal and had tamoxifen only (Table 11).
About 76.7% of patients in the public hospital group tested positive for either oestrogen or progesterone receptors, whereas 85.5% of patients in private sector were hormone receptor positive.
In the public sector, fifty-six (23.3%) patients tested positive for HER2 receptors (2+ or 3+), 149 (62.1%) tested negative (− or 1+) and 35 (15.6%) were untested. None of the patients in the public sector were treated with HER2 agents.
In the private sector, 11 patients with infiltrating carcinomas had HER2 2+ or 3+ immunohistochemistry. Of these, one patient’s FISH test was negative for HER2 amplification, two patients’ medical funders did not approve Herceptin and one was lost to follow-up. Seven patients received Herceptin.
Within each stage, there was no statistically significant association between public or private and outcome. The difference approached significance in patients with stage 0/I disease (p = 0.099) where a higher proportion of patients with no evidence of disease was found in private sector (Table 12).
Survival
Mean overall survival for patients in the public sector and private sectors was 66 months (CI 95% 61.7–71.3) and 79.8 months (CI 95% 76–83.6; p < 0.001), respectively.
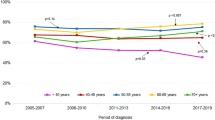
There was a trend to better survival for private patients if grouped by stage for stages I–IV, but it did not reach statistical significance (Figs. 1, 2; Table 13).

Kaplan–Meier overall survival analysis for public and private sector patients

Kaplan–Meier analysis for disease free survival in public and private sector patients
Disease-free survival for all public patients were 63.5 months (CI 95% 59.3–67.7) versus 78.8 months in private (CI 95% 75.0–82.7; p < 0.001).
Average follow-up for patients in the public and private sectors was 48 and 55 months respectively (Table 14).
Discussion
Breast cancer is the most common cancer in women worldwide [14]. Access to health care differs between high and low socio-economic groups in South Africa. According to the WHO, privately insured patients, which constitute only 16% of the population, utilise about $1500 annually per person, whereas the not insured 84% of the population, which is catered for in public institutions, utilise $120 annually [15].
In common with reported figures from Brazil, a country much like South Africa in terms of Gini coefficient [7], patients utilising health care in public hospitals presented with more advanced disease than those accessing private health care, and therefore had a poorer outcome [3, 16]. In our series, if a similar proportion of patients in the public sector presented with early disease, one would have expected to have seen 86 more patients with either stage 0 or I breast cancer in public. As 90% of patients with such early disease are known to be alive with no evidence of disease, an additional 77 patients in the public sector would have been saved from death due to breast cancer.
Annual mammographic screening for women aged 40 and more is recommended by the Cancer Association of South Africa (CANSA), but is currently not part of the Western Cape Health policy [2]. In an earlier study at Tygerberg Hospital, it was found that in the period from 2003 to 2012, 24% of mammograms were performed for “screening” purposes. In this group, cancer was diagnosed in 11.4 out of every 1000 examinations (1.14%) [17]. A similar detection rate was recorded in a Malaysian screening series, indicating that breast cancer incidence rates for urbanised populations in middle-income developing countries with a predominant non-white population may be similar to those in developed countries [17]. Consequently, the WHO recommends for middle-income countries the establishment of mammographic population screening programs [18].
In our current analysis, 10% of patients were screened for disease in the public sector, whereas 26% of patients in the private sector presented for screening purposes. Some authors contend that screening in the USA has not decreased risk of death from breast cancer, even though it was noted that as a result of screening programmes, patients were more likely to present with earlier stage disease [19]. It is likely that in a resource-constrained environment, where later stage at presentation is the main determinant of poorer outcomes, the beneficial effects of screening programmes would be amplified, leading to better outcomes. Others from developing countries have followed a similar approach to us in opportunistic screening and have argued that such efforts may be effective in reducing the stage at presentation [16].
In addition, perhaps the more important point in the differences in rates of screening in the public and private groups in our study reflects not only the access to screening, but rather the attitude of asymptomatic patients towards their health, with far more people in the private sector presenting for purely screening purposes. Other researchers have documented a linear relationship between the human development index (HDI) and stage presentation, where a high HDI was associated with a higher rate of stage I disease, and a lower HDI associated with a lower rate [16].
As such, increased screening alone does not account for the vast differences seen in patients with breast cancer in the public and private health sectors. In a rural community in South Africa, poor knowledge and understanding of cancer combined with absence of health-seeking behaviour prevented the early detection of disease [20] and should be targeted for educational interventions.
Taxanes and biological agents such as Herceptin provide improved outcomes in the treatment of breast cancer [21, 22]. Patients in the public sector had no access to these agents. Although a trend towards better outcomes were observed in the private sector in the same stages of breast cancer, it did not reach statistical significance. With a larger private sector sample, such a difference will likely be demonstrable. As some of these agents’ use is still limited by cost, it may not be feasible for resource-constrained countries to invest vast amounts of money on such expensive medication for everyone. For the individual at risk however, access to newer pharmacological agents would make a tremendous difference and should therefore be motivated for. A cost-effectiveness analysis in Canada for example, has shown that the cost of taxane-containing chemotherapy, compared favourably with the improvement in quality-adjusted life years (QALY’s), in patients with breast cancer, and can be regarded as an acceptable standard chemotherapy regimen [23].
With the exception of reconstruction post mastectomy, surgical treatments were similar between public and private patients, and in keeping with internationally accepted standards of care, indicating less of a gap than in the provision of medical oncological treatments, where the greater availability of advanced treatment options may explain the trend towards better survival in private patients [21, 22]. This presents an area for improvement of resource allocation, notably as outcomes have been shown to be different between African–American and white American women [24]; black women in southern Africa have a higher likelihood of more aggressive breast cancers [25] and would thus benefit from access to more effective systemic treatments.
The increased mortality of public patients in our series due to unrelated causes indicates poorer health in general. In a similar study comparing patients in the same geographical area in South-East Asia (from Malaysia, like South Africa an upper-middle-income country and Singapore, a high-income country), patients treated in Malaysia had a 67% higher risk of mortality than patients diagnosed in Singapore [26]. Like us, the authors found late stage at diagnosis but also poorer general health a reason for the poorer overall survival in the Malaysian patients.
Others have documented the influence of the quality of health systems on outcome of cancer patients on a global level [27]. We therefore postulate that unless health systems in general are improved, much of the effort spent in improving cancer care will be lost due to poor survival from unrelated causes in poor patients.
Further study is needed to quantify the differences observed in similarly treated patients with equal clinical staging from different socio-economic groups in our country, to evaluate specific issues that may need to be addressed in future. In this series, the main determinant of poorer outcomes observed in the public sector was the later stage at presentation. Even though there is a strong tendency towards better outcomes within stage analysis in the private sector, the area where most resources need to be allocated is a public health issue, where access to health care, attitudes towards breast health, appropriate and timeous referral, patient and health care provider education, and shorter clinic waiting times are all issues that can be addressed to make a difference in patients with breast cancer.
Conclusion
Treatment of breast cancer differs between the public and private health care sectors in South Africa. Although there is a strong tendency towards better outcomes in stage-matched comparison, the factor that had the greatest effect on outcome was the later stage at presentation in public. These points to potential targets for improvement in the public sector, such as better access to health care, health education of communities and the importance of regular, organised public screening programmes.
References
Jemal A, Bray F, Ferlay J (2011) Global cancer statistics. CA Cancer J Clin 61:69–90
Herbst MC (2015) Cancer Association of South Africa (CANSA) fact sheet on the top ten cancers per population group top ten most common cancers of women top ten most common cancers of Asian men. Cansa 2015:1–6
Liedke PER et al (2014) Outcomes of breast cancer in Brazil related to health care coverage: a retrospective cohort study. Cancer Epidemiol Biomark Prev 23:126–133
Kaffashian F et al (2003) Socioeconomic effects on breast cancer survival: proportion attributable to stage and morphology. Br J Cancer 89:1693–1696
Woods LM, Rachet B, Coleman MP (2006) Origins of socio-economic inequalities in cancer survival: a review. Ann Oncol 17:5–19
Niu X, Roche LM, Pawlish KS, Henry KA (2013) Cancer survival disparities by health insurance status. Cancer Med 2:403–411
The World Factbook—Central Intelligence Agency (2017) https://www.cia.gov/library/publications/the-world-factbook/fields/2172.html. Accessed on 2nd April 2017
Ncayiyana D (2007) Racial profiling in medical research: what are we measuring? S Afr Med J 97(12):1225–1226
Greene FL, AJCC, ACS (2002) AJCC cancer staging manual, 6th edn, pp 255–281. https://cancerstaging.org/references-tools/deskreferences/Documents/AJCC6thEdCancerStagingManualPart1.pdf
Carlson RW et al (2009) Breast cancer. Clinical practice guidelines in oncology. J Natl Compr Cancer Netw 7:122–192
Glick JH et al (2005) Meeting highlights: international expert consensus on the primary therapy of early breast cancer 2005. Ann Oncol 16:1569–1583
Mamounas EP (2003) NSABP breast cancer clinical trials: recent results and future directions. Clin Med Res 1:309–326
Kaplan EL, Meier P (1958) Nonparametric estimation from incomplete observations. J Am Stat Assoc 53:457–481
Parkin DM, Bray F, Ferlay J, Jemal A (2014) Cancer in Africa 2012. Cancer Epidemiol Biomark Prev 23:953–966
Benatar SR (2013) The challenges of health disparities in South Africa. S Afr Med J 103:154–155
Teh YC et al (2015) Opportunistic mammography screening provides effective detection rates in a limited resource healthcare system. BMC Cancer 15:405
Apffelstaedt JP, Dalmayer L, Baatjes K (2014) Mammographic screening for breast cancer in a resource-restricted environment. S Afr Med J. 104:294
Cancer Screening Guidelines|Detecting Cancer Early. https://www.cancer.org/healthy/find-cancer-early/cancer-screening-guidelines/american-cancer-society-guidelines-for-the-early-detection-of-cancer.html
Bleyer A, Welch HG (2012) Effect of three decades of screening mammography on breast-cancer incidence. N Engl J Med 367(21):1998–2005
Maree JE, Wrights S (2010) How would early detection be possible? An enquiry into cancer related knowledge, understanding and health seeking behaviour in urban black women in Tshwane, South Africa. Eur J Oncol Nurs 14(3):190–196
Ghersi D, Wilcken N, Simes J, Donoghue E (2003) Taxane containing regimens for metastatic breast cancer. Cochrane Database Syst Rev (2):CD003366. doi:10.1002/14651858.CD003366.pub2
Balduzzi S et al (2014) Trastuzumab-containing regimens for metastatic breast cancer. Cochrane Database Syst Rev (6):CD006242. doi:10.1002/14651858.CD006242.pub2
Younis T, Rayson D, Skedgel C (2011) The cost-utility of adjuvant chemotherapy using docetaxel and cyclophosphamide compared with doxorubicin and cyclophosphamide in breast cancer. Curr Oncol 18(6):e288–e296
Newman LA et al (2006) Meta-analysis of survival in African American and white American patients with breast cancer: ethnicity compared with socioeconomic status. J Clin Oncol 24(9):1342–1349
Dickens C, Duarte R, Zietsman A, Cubasch H, Kellett P (2014) Racial Comparison of receptor-defined breast cancer in Southern African women: subtype prevalence and age-incidence analysis of nationwide cancer registry data. Cancer Epidemiol Prev Biomark. doi:10.1158/1055-9965.EPI-14-0603
Saxena N et al (2012) Breast cancer in South East Asia: comparison of presentation and outcome between a middle income and a high income country. World J Surg 36:2838–2846. doi:10.1007/s00268-012-1746-2
Sankaranarayanan R et al (2010) Cancer survival in Africa, Asia, and Central America: a population-based study. Lancet Oncol 11:165–173
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Coetzee, W.C., Apffelstaedt, J.P., Zeeman, T. et al. Disparities in Breast Cancer: Private Patients Have Better Outcomes Than Public Patients. World J Surg 42, 727–735 (2018). https://doi.org/10.1007/s00268-017-4187-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-017-4187-0