
Abstract
Background
Systemic inflammation as evidenced by the Glasgow prognostic score (GPS) predicts cancer-specific survival in various types of cancer. The aim of this study was to evaluate the significance of GPS in therapeutic outcome after surgical resection of gallbladder cancer.
Methods
The subjects were 51 patients who underwent surgical resection for gallbladder cancer. For the assessment of systemic inflammatory response using the GPS, patients were classified into three groups: patients with normal albumin (≥3.5 g/dl) and normal C-reactive protein (CRP) (≤1.0 mg/dl) as GPS 0 (n = 38), those with low albumin (<3.5 g/dl) or elevated CRP (>1.0 mg/dl) as GPS 1 (n = 8), and those with low albumin (<3.5 g/dl) and elevated CRP (>1.0 mg/dl) as GPS 2 (n = 5). We retrospectively investigated the relation between patient characteristics including GPS, and disease-free as well as overall survival.
Results
In disease-free survival, advanced tumor stage based on pathology (p = 0.006), positive lymph node metastasis (p = 0.001), and GPS 1 or 2 (p = 0.006) were independent predictors of cancer recurrence in multivariate analysis. In overall survival, positive lymph node metastasis (p = 0.002) and GPS 1 or 2 (p = 0.032) were independent predictors of poor patient outcome in multivariate analyses.
Conclusion
The GPS in patients with gallbladder cancer is an independent prognostic predictor after surgical resection.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Gallbladder cancer is a relatively rare neoplasm [1], and often diagnosed at advanced stages [2, 3]. The therapeutic outcome was favorable for pT1 cancer with the 5-year survival rate of 85.9 %, whereas quite poor for pT3 and pT4 cancer with the 5-year survival rate of 19.2–14.1 % in Japan [4]. In addition, optimal extent of liver resection including extended lobectomy, resection of segment 4b and segment 5, and liver bed resection is still controversial [5]. Although pre-operative prognostic indicators of gallbladder cancer are limited, elucidation of such parameters is important for the post-operative management after surgical resection.
The presence of systemic inflammatory response, as evidenced by an elevated C-reactive protein (CRP) concentration, may be associated with poor therapeutic outcome for malignant tumors. Several recent investigators reported that the systemic inflammatory response by the combination of serum CRP and albumin concentrations, i.e., Glasgow prognostic score (GPS) predicts cancer-specific survival, including colorectal [6], gastro-esophageal [7], urinary bladder [8], pancreatic [9], renal [10], and non-small-cell lung cancers [11]. In this study, we retrospectively investigated the relation between GPS and disease-free as well as overall survival after surgical resection of gallbladder cancer.
Patients and methods
Between January 2004 and December 2011, 57 patients with gallbladder cancer underwent surgical resection at the Department of Surgery, Jikei University Hospital, Tokyo, Japan. Of these, 6 patients were excluded, 3 patient for insufficient data, 2 patients for palliative resection, and 1 patient who were lost to follow up, leaving the remaining 51 patients for the study. Basically, patients with incidental diagnosis of gallbladder cancer after noncurative cholecystectomy underwent additional hepatic resection with or without bile duct and lymph node resection.
For the assessment of systemic inflammatory response using the GPS, the patients were classified into three groups: patients with normal albumin (≥3.5 g/dl) and normal CRP (≤1.0 mg/dl) as GPS 0 (n = 38), those with low albumin (<3.5 g/dl) or elevated CRP (>1.0 mg/dl) as GPS 1 (n = 8), and both low albumin (<3.5 g/dl) and elevated CRP (>1.0 mg/dl) as GPS 2 (n = 5).
We investigated the relation between clinicopathologic variables and disease-free as well as overall survival after surgical resection by univariate and multivariate analyses. The factors consisted of the following 8 factors: age, gender, pre-operative hemoglobin, post-operative complications, tumor stage based on tumor pathology (T stage), status of lymph node metastasis on pathology, the presence or absence of gallstones, and status of GPS.
Next, we investigated the relation between clinicopathologic variables and GPS by univariate and multivariate analyses. The factors consisted of the following 11 variables: age, gender, pre-operative hemoglobin, surgical procedure, additional radical resection after cholecystectomy, duration of operation, intra-operative blood loss, post-operative complications, T stage based on tumor pathology, status of lymph node metastasis on pathology, and the presence or absence of gallstones.
Clinicopathologic continuous variables were classified into two groups for the Log-rank test and the Cox proportional hazard regression model as follows: age <70 or ≥70 years, and pre-operative hemoglobin <12 or ≥12.
Recurrence of gallbladder cancer was defined as newly detected local, or distant metastatic tumors by ultrasonogaphy, computed tomography or magnetic resonance image with or without increase in serum carcinoembryonic antigen or carbohydrate antigen 19-9.
This retrospective study was approved by the Ethics Committee of Jikei University School of Medicine (#21-121).
Statistical analysis
Data are expressed as a mean ± standard deviation (SD). Univariate analysis was performed using the non-paired Student’s t and χ2 tests. Analysis of disease-free and overall survival was performed using the Log-rank test for univariate analysis, and the Cox proportional regression model and the logistic regression model with backward elimination stepwise approach for multivariate analysis. All p values were considered statistically significant when the associated probability was less than 0.05.
Results
Patient characteristics
Patient characteristics are outlined in Table 1. Among the study population, the mean age was 67.8 years with a range from 38 to 88 years, and 27 of them were male. Operative procedures consisted of cholecystectomy in 19, liver bed resection with in 22, hepatic resection of segment 4b and segment 5 in 8, and extended right lobectomy in 2 patients, respectively. GPS consisted of GPS 0 in 38, GPS 1 in 8, and GPS 2 in 5 patients, respectively. In GPS 1, 3 patients were classified due to low albumin, and 5 patients were classified due to elevated CRP. Post-operative complications developed in 12 of 51 patients (23.5 %), consisting of SSI in 6 (11.8 %), pulmonary complications in 7 (13.7 %), and bile leakage in 2 patients (3.9 %), respectively. In this study, the five-year disease-free and overall survival rates after surgical resection for gallbladder cancer were 49.7 and 67.9 %, respectively.
Univariate and multivariate analyses of clinicopathologic variables in relation to disease-free and overall survival after surgical resection of gallbladder cancer
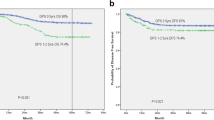
Table 2 lists the relationship between the clinicopathologic variables and disease-free and overall survival after surgical resection of gallbladder cancer. In univariate analysis of disease-free survival, pre-operative hemoglobin less than 12 g/dl (p = 0.021), the presence of post-operative complications (p = 0.008), advanced T stage (p < 0.001), positive lymph node metastasis (p < 0.001), and GPS 1 or 2 (Fig. 1a; p = 0.031) were significantly associated with cancer recurrence. In multivariate analysis, advanced T stage (p = 0.006), positive lymph node metastasis (p = 0.001), and GPS 1 or 2 (p = 0.006) were independent risk factors associated with poor disease-free survival.

In statistical analysis, GPS 1 or 2 was an independent risk factor of poor disease-free survival (a), and overall survival (b)
In univariate analysis of overall survival, the presence of post-operative complications (p = 0.006), advanced T stage (p < 0.001), and positive lymph node metastasis (p < 0.001) were significantly associated with poor overall survival. GPS 1 or 2 tended to be associated with poor overall survival, but not significantly (Fig. 1b; p = 0.078). In multivariate analysis, positive lymph node metastasis (p = 0.002) and GPS 1 or 2 (p = 0.032) were independent risk factors associated with poor overall survival. Advanced T stage tend to be associated with poor overall survival, which however was not significant (p = 0.072).
Association between clinicopathologic variables and Glasgow prognostic score
Table 3 lists the relationship between patient characteristics and GPS. Duration of operation in patients with GPS 1 or 2 was longer than those in GPS 0 patients (p = 0.001) on univariate analysis. Patients with GPS 1 or 2 tended to have advanced T stage (p = 0.274), needed more invasive procedures, such as hepatic resection of segment 4b and segment 5 or extended right lobectomy (p = 0.105) and had greater intra-operative blood loss (p = 0.053) as compared to those with GPS 0, which however was not significant. In multivariate analysis, duration of operation (p = 0.049) and intra-operative blood loss (p = 0.012) were independent factors associated with GPS.
Discussion
In patients with gallbladder cancer, the resection rate and the curative resection rate were 69.8 and 37.7 %, respectively in Japan [4]. The depth of tumor invasion through the gallbladder wall and status of lymph node metastasis were strongly associated with therapeutic outcome after resection [4, 12]. In this study, advanced T stage, positive lymph node metastasis, and GPS 1 or 2 were independent risk factors of cancer recurrence in multivariate analysis. Positive lymph node metastasis and GPS 1 or 2 were also independent risk factors of poor overall survival, and advanced T stage tended to be associated with poor overall survival, but not independently by multivariate analysis. To the best of our knowledge, this is the first report of correlating therapeutic outcome after surgical resection of gallbladder cancer with GPS.
GPS had been reported as a predictor of prognosis in patients with various unresectable cancers of the lung [13, 14], breast [15], esophageal or gastric [16], pancreatic [17], renal [18], and colorectal cancer [19]. For primary resectable cancer patients, GPS is associated with therapeutic outcome in colorectal [6], gastro-esophageal [7], urinary bladder [8], pancreatic [9], renal [10], and non-small-cell lung cancers [11]. We previously reported GPS as a predictor of therapeutic outcome in patients with carcinoma of the ampulla of Vater after pancreaticoduodenectomy [20], unresectable colorectal cancer liver metastasis [21], and of post-operative complication in patients with hepatocellular carcinoma after hepatic resection [22]. However, the reasons for the association between GPS, pre-treatment elevated serum CRP or low serum albumin concentrations, and therapeutic outcome in patients with various malignancies remain unclear [23]. In this study, pre-operative patients status including age, primary resection or additional radical resection after noncurative cholecystectomy, positive or negative lymph node metastasis, and presence or absence of gallstone were comparable in patients with GPS 0, and in those with GPS 1 or 2. On the other hand, patients with GPS 1 or 2 tended to have advanced T stage, and needed more invasive procedure, such as hepatic resection of segment 4b and segment 5 or extended right lobectomy as compared to those with GPS 0, but not significantly. These results suggest that GPS may reflect malignant potential of primary tumor rather than lymph node or distant organ metastasis.
Because survival benefit of adjuvant chemotherapy has not been established on gallbladder cancer after surgery [24], further assessments of mechanism(s) between pre-operative systemic inflammatory response and poor outcome may improve therapeutic outcome of gallbladder cancer after curative resection. Patients’ risk stratification using GPS is easy and less invasive, because GPS is composed only of pre-operative serum CRP and albumin concentration, which are routine examinations for peri-operative patients management. GPS therefore is useful for identification of patients at risk of cancer recurrence and poor prognosis after resection for gallbladder cancer.
Conclusion
In conclusion, the GPS upon diagnosis in patients with gallbladder cancer was an independent predictor in disease-free and overall survival after surgical resection. Measurement of the GPS may help decision making in the post-operative management of patients with gallbladder cancer.
References
Fong Y, Wagman L, Gonen M, Crawford J, Reed W, Swanson R, Pan C, Ritchey J, Stewart A, Choti M (2006) Evidence-based gallbladder cancer staging: changing cancer staging by analysis of data from the National Cancer Database. Ann Surg 243:767–771 discussion 771–774
Hawkins WG, DeMatteo RP, Jarnagin WR, Ben-Porat L, Blumgart LH, Fong Y (2004) Jaundice predicts advanced disease and early mortality in patients with gallbladder cancer. Ann Surg Oncol 11:310–315
Ito H, Matros E, Brooks DC, Osteen RT, Zinner MJ, Swanson RS, Ashley SW, Whang EE (2004) Treatment outcomes associated with surgery for gallbladder cancer: a 20-year experience. J Gastrointest Surg 8:183–190
Miyakawa S, Ishihara S, Horiguchi A, Takada T, Miyazaki M, Nagakawa T (2009) Biliary tract cancer treatment: 5,584 results from the Biliary Tract Cancer Statistics Registry from 1998 to 2004 in Japan. J Hepatobiliary Pancreat Surg 16:1–7
D’Angelica M, Dalal KM, DeMatteo RP, Fong Y, Blumgart LH, Jarnagin WR (2009) Analysis of the extent of resection for adenocarcinoma of the gallbladder. Ann Surg Oncol 16:806–816
McMillian DC, Crozier JE, Canna K, Angerson WJ, McArdle CS (2007) Evaluation of an inflammation-based prognostic score (GPS) in patients undergoing resection for colon and rectal cancer. Int J Colorectal Dis 22:881–886
Crumley AB, McMillan DC, McKernan M, Going JJ, Shearer CJ, Stuart RC (2006) An elevated C-reactive protein concentration, prior to surgery, predicts poor cancer-specific survival in patients undergoing resection for gastro-oesophageal cancer. Br J Cancer 94:1568–1571
Hilmy M, Bartlett JM, Underwood MA, MaMillan DC (2005) The relationship between the systemic inflammatory response and survival in patients with transitional cell carcinoma of the urinary bladder. Br J Cancer 92:625–627
Jamieson NB, Glen P, McMillan DC, McKay CJ, Foulis AK, Carter R, Imrie CW (2005) Systemic inflammatory response predicts outcome in patients undergoing resection for ductal adenocarcinoma head of pancreas. Br J Cancer 92:781–784
Lamb GW, McMillan DC, Ramsey S, Aitchison M (2006) The relationship between the preoperative systemic inflammatory response and cancer specific survival in patients undergoing potentially curative resection for renal clear cell cancer. Br J Cancer 94:781–784
Hara M, Matsuzaki Y, Shimizu T, Tomita M, Ayabe T, Enomoto Y, Onitsuka T (2007) Preoperative serum C-reactive protein level in non-small cell lung cancer. Anticancer Res 27:3001–3004
Ito H, Ito K, D’Angelica M, Gonen M, Klimstra D, Allen P, DeMatteo RP, Fong Y, Blumgart LH, Jarnagin WR (2011) Accurate staging for gallbladder cancer: implications for surgical therapy and pathological assessment. Ann Surg 254:320–325
Forrest LM, McMillan DC, McArdle CS, Angerson WJ, Dunlop DJ (2003) Evaluation of cumulative prognostic scores based on the systemic inflammatory response in patients with inoperable non-small-cell lung cancer. Br J Cancer 89:1028–1030
Forrest LM, McMillan DC, McArdle CS, Angerson WJ, Dunlop DJ (2004) Comparison of an inflammation-based prognostic score (GPS) with performance status (ECOG) in patients receiving platinum-based chemotherapy for inoperable non-small-cell lung cancer. Br J Cancer 90:1704–1706
Al Murri AM, Bartlett JM, Canney PA, Doughty JC, Wilson C, McMillan DC (2006) Evaluation of an inflammation-based prognostic score (GPS) in patients with metastatic breast cancer. Br J Cancer 94:227–230
Crumley AB, McMillan DC, McKernan M, McDonald AC, Stuart RC (2006) Evaluation of an inflammation-based prognostic score in patients with inoperable gastroesophageal cancer. Br J Cancer 94:637–641
Glen P, Jamieson NB, McMillan DC, Carter R, Imrie CW, McKay CJ (2006) Evaluation of an inflammation-based prognostic score in patients with inoperable pancreatic cancer. Pancreatology 6:450–453
Ramsey S, Lamb GW, Aitchison M, Graham J, McMillan DC (2007) Evaluation of an inflammation-based prognostic score in patients with inoperable renal cancer. Cancer 109:205–212
Leitch EF, Chakrabarti M, Crozier JE, McKee RF, Anderson JH, Horgan PG, McMillan DC (2007) Comparison of the prognostic value of selected markers of the systemic inflammatory response in patients with colorectal cancer. Br J Cancer 97:1266–1270
Shiba H, Misawa T, Fujiwara Y, Futagawa Y, Furukawa K, Haruki K, Iwase R, Wakiyama S, Ishida Y, Yanaga K (2013) Glasgow prognostic score predicts therapeutic outcome after pancreaticoduodenectomy for carcinoma of the ampulla of vater. Anticancer Res 33:2715–2721
Furukawa K, Shiba H, Haruki K, Fujiwara Y, Iida T, Mitsuyama Y, Ogawa M, Ishida Y, Misawa T, Yanaga K (2012) The Glasgow prognostic score is valuable for colorectal cancer with both synchronous and metachronous unresectable liver metastases. Oncol Lett 4:324–328
Fujiwara Y, Shiba H, Furukawa K, Iida T, Haruki K, Sakamoto T, Gocho T, Wakiyama S, Hirohara S, Ishida Y, Misawa T, Ohashi T, Yanaga K (2010) Glasgow prognostic score is related to blood transfusion requirements and post-operative complications in hepatic resection for hepatocellular carcinoma. Anticancer Res 30:5129–5136
Moyes LH, Leitch EF, McKee RF, Anderson JH, Horgan PG, McMillan DC (2009) Preoperative systemic inflammation predicts postoperative infectious complications in patients undergoing curative resection for colorectal cancer. Br J Cancer 100:1236–1239
Horgan AM, Amir E, Walter T, Knox JJ (2012) Adjuvant therapy in the treatment of biliary tract cancer: a systematic review and meta-analysis. J Clin Oncol 30:1934–1940
Acknowledgments
We thank Dr. Matsushima (Division of Clinical Epidemiology, Jikei University School of Medicine) for his contributions in statistical analyses.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Shiba, H., Misawa, T., Fujiwara, Y. et al. Glasgow Prognostic Score Predicts Outcome After Surgical Resection of Gallbladder Cancer. World J Surg 39, 753–758 (2015). https://doi.org/10.1007/s00268-014-2844-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-014-2844-0