
Abstract
Background
The present study was designed to investigate the prognostic factors of stage IIA (pT3N0M0) colon cancer.
Methods
We retrospectively reviewed consecutive patients with stage IIA colon cancer treated with curative surgery alone from January 2004 to June 2008 in Peking University Cancer Hospital. Patient demographics, and clinical, histopathologic, and laboratory data were analyzed. Univariate and multivariate analyses were carried out to identify prognostic factors associated with 3-year disease-free survival (DFS).
Results
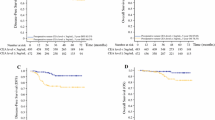
For the 84 valid cases reviewed in this study, the 3-year DFS was 88.1 %. That for a group with elevated CEA was 77.1 % and for a group with a normal CEA level, it was 95.9 %, with statistical difference (p = 0.007). Multivariate analysis demonstrated that CEA level (p = 0.012, OR = 8.013, 1.573–40.817), expression of Ki67 (p = 0.099, OR = 3.298, 0.799–3.610), male gender (p = 0.024, OR = 7.212, 1.293–40.237), and anemia (p = 0.011, OR = 6.461, 1.537–27.151) were the independent prognostic factors for 3-year DFS. Stratified analysis revealed that an elevated CEA level combined with high expression of Ki67 was associated with poorer prognosis (3-year DFS 70 %).
Conclusions
An elevated preoperative serum level of CEA and high expression of Ki67 in tumor tissue were predictors of poor prognosis for patients with stage IIA colon cancer. These patients should therefore be considered candidates for receiving intensive surveillance. Future clinical trials using multicenter patient cohorts should be prospectively performed to evaluate whether these high-risk patients could benefit from adjuvant chemotherapy to improve prognosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colon cancer is one of the most common malignant tumors of the gastrointestinal tract. The American Joint Cancer Commission/tumor-node-metastasis (AJCC TNM) staging system [1] is an internationally recognized system for staging of colon cancer. Some 30 % to 40 % of colon cancers are diagnosed as TNM stage II disease following radical resection [2, 3]. According to the recommendations from current guidelines, the indications for adjuvant treatment for stage II colon cancer remain controversial [4–7], particularly in view of the consensus that TNM stage III colon cancer should routinely receive adjuvant chemotherapy. Adjuvant chemotherapy is only considered for patients with stage II colon cancer characterized by poor prognostic features, including obstruction, perforation, emergent admission, T4 stage, resection of fewer than 12 lymph nodes, and poor histology [8, 9].
Stage IIA colon cancer has a relatively good prognosis after surgery alone, with 5-year survival rates of approximately 80 % [1]; however, eventually 20 % to 25 % of patients will die of recurrence or distant metastasis [10]. Thus, the current consensus supports the use of adjuvant chemotherapy for those stage II patients with adverse characteristics but leaves an open question about the optimal management of those patients with the risk factors that can further stratify stage IIA (T3N0M0) tumors and predict the outcome without adverse characteristics [11] .
In the present study we performed a retrospective analysis of demographics, clinical, histopathologic, and laboratory data of stage IIA colon cancer patients to identify the prognostic factors associated with disease-free survival (DFS). The results of these analyses are reported herein.
Patients and methods
Patients
From January 2004 to June 2008 a total of 161 patients who were diagnosed with colon cancer and underwent radical colectomy were pathologically confirmed as having stage II colon cancer at Peking University Cancer Hospital. The clinical, pathological, and immunohistochemical data of these patients were collected and analyzed in this retrospective study.
Surgery
All operations were open surgeries performed by two senior colorectal surgeons. Radical colectomy was defined as colectomy with high ligation of the central vessels following the principle of complete mesocolic excision (CME) [12]. Tumor-specific excision included a more than 15 cm proximal/distal margin in right/transverse/left colon cancer and a 5–10 cm proximal/distal margin in sigmoid cancer. Mesocolic excision (or ileum mesentery for cecum cancer) was also performed. All stapling anastomoses were constructed by the end-to-side method with hand-sewn enhancement. Drainage without vacuum was placed in all cases.
Exclusion criteria included previous malignant disease history, hereditary colon cancer, synchronous distant metastasis, and inflammatory bowel disease (IBD).
Immunohistochemical assay of P53 and Ki67
Paraffin-embedded blocks of resected specimens were cut into 5 μm sections. P53 and Ki67 expression were analyzed using a standard avidin–biotin technique. Sections of the tissue blocks were de-paraffinized with xylene and then rehydrated in a graded ethanol series. Tissue sections were washed three times in 0.05 mol/L phosphate-buffered saline (PBS), and were later incubated in endogenous peroxidase blocking solution (3 %) for 8 min. Nonspecific antibody binding was blocked by pretreatment with phosphate-buffered saline containing 5 g/L bovine serum albumin for 10 min.
Sections were then rinsed in PBS and incubated at 4 °C overnight with primary MIB1monoclonal antibody (DAKO, USA) at a 1:60 dilution and the primary p53 D07 monoclonal antibody (Vector Laboratories, Burlingame, CA) at a 1:50 dilution, respectively. As a negative control, the primary antibody was discarded and replaced with PBS. The sections were washed with PBS, covered with a 1:100 dilution of streptavidin–biotin-peroxidase complex at room temperature for 20 min. Color development was achieved by applying a 3-3′-diaminobenzine-tetrahydrochloride (DAB) reagent (Sigma, Oakville, Ontario) for 5 min. Tissues were counterstained with hematoxylin (Sigma), dehydrated in a graded ethanol series, and mounted with coverslips. All the above procedures were performed according to the manufacturer’s instructions.
Evaluation of immunohistochemical staining
Quantification was carried out by two trained pathologists who were blinded with respect to the patients’ identity and had no previous knowledge of any of the cases. Slides were examined under a light microscope and scored independently. For the tissue evaluation of Ki67, each slide was scored based on the percentage of positively stained malignant nuclei. The following ranges were used: 0–20 %, >20–40 %, >40–60 %, >60–80 %, and >80–100 %. Samples with Ki67 nuclear staining equal to or above 40 % were considered to have a high proliferative index, whereas nuclear positivity below 40 % was considered a low proliferative index (Fig. 1).

Positive staining of Ki67 by immunohistochemistry in paraffin-fixed tissue of colon cancer. Magnification ×100
The p53 antigen was considered overexpressed when ≥10 % of the malignant nuclei were positive. If fewer than 10 % of the nuclei were stained, the slide was scored as having normal p53 expression [13].
Follow-up
Patients were followed at three-month intervals for the first two years and then at six-month intervals for the next three years. Evaluations consisted of physical examination, serum carcinoembryonic antigen (CEA), a complete blood count, and blood chemical analysis. Proctoscopy, abdominal ultrasonography, CT of the abdomen and pelvis, and chest radiography were also routinely performed every 6–12 months.
Variables and statistical analysis
Nine variables were recorded and analyzed statistically. Preoperative variables included age, gender, and preoperative hemoglobin level (Hgb). Tumor-related variables recorded included TNM staging by the seventh AJCC cancer staging system, lymph node number, and lymph vessel invasion. Immunohistochemical variables included expression of the Ki67 and p53 antigens in paraffin-fixed tumor specimens. The categorical variables were analyzed with the Pearson Chi-square or Fisher’s exact test, when appropriate. The logistic regression model (Backward, LR) was used in multivariate analysis, variables would retain in the regression equation when p value< 0.1, the risk ratio was also calculated (odds ratio; OR). Disease-free survival (DFS) curves were compared among groups using the log-rank test for time-to-event parameters. The Kaplan–Meier survival curve was used to estimate the proportion of patients surviving or remaining disease-free at each time interval. Multivariate Cox proportional hazards regression was used to analyze the major factors affecting DFS, with the level of significance set at 0.1. The software SPSS version 13.0 for Windows (SPSS Inc., Chicago, IL) was used for the analysis.
Results
Patient demographics
The records of 161 patients were reviewed. The disease of 84 of those patients who were eligible for analysis was pathologically staged as IIA. The median follow-up period was 45 months (2–77 months). The follow-up rate was 88.1 %, with 10 patients lost. The median patient age was 67 years (range: 34–89 years), with 59.5 % (50/84) male patients. Thirty-two patients had preoperative anemia (Hgb <110 g/L). There were 43 right colon cancers and 41 left colon cancers (including sigmoid cancer) according to tumor site. Some 70.2 % of patients had more than 12 retrieved lymph nodes (LN), and the median number of LN number was 14.5 (range: 4–48). Poor tumor differentiation (G3–4) was identified in 21.4 % (18/84) of all cases. Lymphovascular invasion was rarely represented in this group (2.4 %; 2/84) and was not considered a variable in the statistical analysis. A preoperative elevated serum CEA level was observed in 41.7 % of patients (35/84).
Survival
The 3-year DFS was 88.1 % in all cases. Eight patients had liver metastases, and two patients had lung metastases. No local recurrences were recorded.
Univariate survival analysis
By univariate analysis, possible factors associated with disease-free survival were tested (log-rank test). Patients with an elevated CEA level had poorer DFS than those with a normal CEA level, and the difference was statistically significant (95.9 % versus 77.1 %; p = 0.007). Age ≥65 (p = 0.054), preoperative anemia (p = 0.108), and high expression of Ki67 (p = 0.104) showed a tendency to decrease 3-year DFS; however, the difference was not statistically significant on univariate analysis. Expression of p53 and the other factors had no significance in survival analysis (Table 1).
Multivariate survival analysis
All variables in the univariate analysis were entered into the Cox regression. Four of those variables were identified as independent risk factors for 3-year DFS: male gender (p = 0.024, OR = 7.212, 1.293–40.237), CEA level (p = 0.012, OR = 8.013, 1.573–40.817), anemia (p = 0.011, OR = 6.461, 1.537–27.151), and expression of Ki67 (p = 0.099, OR = 3.298, 0.799 –13.610). Further subgroup analysis revealed that patients with an elevated CEA level and high expression of Ki67 had poorer DFS when compared with those who had a normal CEA level (p = 0.002).
Discussion
About 40 % of patients with colon cancer were classified as pathological stage II. Although the prognosis of patients with stage II colon cancer after radical resection is quite good, stage IIA (T3N0M0) and IIB (T4N0M0) patients with 5-year survival rates were 88 % and 75 %. The available randomized controlled trials (RCT), reviews, pooled analyses, and meta-analyses have demonstrated that adjuvant chemotherapy can bring about a 2 % to 4 % increase in absolute survival, a statistically nonsignificant improvement for the entire patient group [8, 14, 15]. Therefore, a number of studies and meta-analyses were designed to find some useful factors to stratify stage II colon cancer patients into subgroups with poor prognosis and good prognosis. Among the clinical and histopathologic factors for poor prognostic features were (1) elevated preoperative CEA (>5 ng/mL), (2) diagnosis in the setting of bowel obstruction or perforation, (3) need for emergent operation, (4) T4 stage (extension to adjacent organs), (5) inadequate nodal resection (<12 nodes), or (6) peritumoral lymphatic/venous invasion [8, 16–18]. Molecular and biological factors for poor prognostic features include (1) tumor budding, (2) abnormal expression of vascular endothelial growth factor (VEGF) and integrin, (3) microRNA expression profiles, and (4) loss of Bcl-2 expression [19–23].
Because the prognosis of stage IIB & IIC (T4a/b N0M0) disease approaches that of stage III [8, 24], most of the studies recommend adjuvant chemotherapy for these patients [8]. However, there were no reliable prognostic factors for stage IIA (T3N0M0) colon cancer that might help to identify patients at high risk of recurrence who might benefit from adjuvant chemotherapy. The present study therefore focused exclusively on patients classified as stage IIA to identify patients at high risk of tumor relapse by analyzing the actual prognostic impact of a wide spectrum of pathologic parameters.
Carcinoembryonic antigen defines a class of complex glycoproteins among approximately 20 related molecules in the immunoglobulin gene superfamily [25]. Serum CEA is the most widely accepted tumor marker for colorectal cancer. Its measurement is standardized, quantitative, and readily available in clinical practice. In the College of American Pathologists Consensus Statement, preoperative CEA elevation is classified into category I according to its strength and reliability from published evidence in the literature [18, 26]. The American Society of Clinical Oncology Tumor Marker Expert Panel has recommended preoperative and postoperative measurement of CEA levels for at least 3 years [27].
However, there were still controversies surrounding the indication for adopting adjuvant chemotherapy in stage II colon cancer when the patient has an elevated preoperative serum CEA level. In large-scale clinical trials that focused on adjuvant chemotherapy in the treatment of colon cancer, preoperative serum CEA level was not recorded in the analysis [14, 15, 28–30]. In the MOSAIC trail, postoperative serum CEA level was identified as a risk factor associated with the effect of adjuvant chemotherapy [29]. In contrast, the American Society of Clinical Oncology (ASCO) suggested there were insufficient data to support the use of preoperative CEA levels to determine whether colon cancer patients were candidates for adjuvant therapy, especially in stage II [8].
Actually, elevated serum CEA level has been associated with poorer survival rates and a higher incidence of systemic recurrence in colorectal cancer, and has definitely proved to be of prognostic value in various published studies and is generally used in preoperative patient evaluations [31–38], particularly in patients classified as having early stage (stage I and II) disease [33, 35]. However, although 90 % of colorectal cancers produce CEA, elevated serum levels were found in only 30 % to 40 % of patients at the time of diagnosis, because CEA enters the portal circulation and is metabolized on first pass through the liver [39]. The limited proportion of positive serum CEA tests might mitigate its weight in predicting patient outcomes.
Ki67 antigen expression is one of the most widely used markers to evaluate the proliferation of tumor cells, except during the G0 and early G1 phases of tumor growth [13]. Some investigators have demonstrated that Ki67, like p53, had significant prognostic value for colon cancer but could not be used alone to clearly discern among groups of patients with different prognosis [40, 41].
Some authors have tried to use a combined model including CEA and other pathological parameters to improve the accuracy in predicting prognosis in stage II colon cancer [42–45]. Ishida et al. reported that immunohistochemical analysis of the expression of Ki67 or CEA in metastatic lymph nodes may provide useful indicators of patient survival in Dukes’ C colorectal cancer. Maksimovic reported that patients with positive immunohistochemical CEA, PCNA, and p53 values had statistically shorter life expectancy in comparison with the patients with negative CEA, PCNA, and p53 values [45]. Graziano and Cascinu reviewed the studies that had investigated cell proliferation markers, angiogenesis markers, and biochemical markers that may play prognostic roles in Dukes’ B colorectal cancer patients, but the data did not provide sufficient evidence for the incorporation of available prognostic biomarkers into clinical practice. The limitation of these previous studies was that the CEA level was assessed through immunohistochemical but not serological methods, which could reflect secreting and proliferating functions of tumor.
In our results, multivariate analysis found that preoperative serum CEA level and expression of Ki67 in tumor tissue were independent prognostic factors for 3-year DFS. From a methodological point of view, immunohistochemical staining of Ki67 could detect the proliferative function of tumor cells in situ, whereas serological examination of CEA could directly detect the functional protein produced and secreted by tumor cells. Combining these two methods may be more useful in predicting the prognosis of stage IIA colon cancer comprehensively as compared with using the immunohistochemical method alone.
The subgroup of patients who had elevated preoperative serum CEA and high expression of Ki67 had much poorer 3-year DFS than the total group (70 % versus 88.1 %); a survival rate much lower than that reported in the published literature (87.5 %) for stage IIA (T3N0M0) colon cancer patients[1].
Other factors, such as gender or anemia, were also associated with 3-year DFS in stage IIA colon cancer. As described in the literature, male patients or patients with anemia had poorer survival in various types of neoplasms [46–49]. These findings could help resolve the complexity surrounding prognosis in stage IIA colon cancer.
Conclusions
We investigated whether an elevated preoperative serum level of CEA combined with high expression of Ki67 in tumor tissue was predictive of poor prognosis for stage IIA colon cancer patients. We could construct a simple prognostic classification that would help to identify a subgroup of patients who need more intensive surveillance. Future clinical trials using multicenter patient cohorts should be prospectively performed to evaluate whether these high-risk cases could benefit from adjuvant chemotherapy to improve prognosis.
References
Edge SB, Byrd DR (2010) AJCC cancer staging manual, 7th edn. Springer, New York 648
Jemal A, Tiwari RC, Murray T et al (2004) Cancer statistics, 2004. CA Cancer J Clin 54:8–29
Sato H, Maeda K, Koide Y (2011) Prognostic factor of stage II colon cancer. Nihon Rinsho 69(Suppl 3):189–192
Betge J, Langner C, Rehak P (2011) Adjuvant chemotherapy improves survival in patients with American Joint Committee on Cancer stage II colon cancer. Cancer 118:2184
Kopetz S, Freitas D, Calabrich AFC et al (2008) Adjuvant chemotherapy for stage II colon cancer. Oncology (Williston Park) 22:260–270 discussion 270, 273, 275
Martin RC (2006) Adjuvant treatment of stage II colon cancer: is there a true no-chemotherapy group? Ann Surg Oncol 13:766–767
Wille-Jorgensen P (2005) No clear evidence for adjuvant therapy in people with stage II colon cancer. Cancer Treat Rev 31:147–150
Benson AB 3rd, Schrag D, Somerfield MR et al (2004) American Society of Clinical Oncology recommendations on adjuvant chemotherapy for stage II colon cancer. J Clin Oncol 22:3408–3419
O’Connor ES, Greenblatt DY, LoConte NK et al (2011) Adjuvant chemotherapy for stage II colon cancer with poor prognostic features. J Clin Oncol 29:3381–3388
Ochs AM, Wong L, Kakani V et al (2004) Expression of vascular endothelial growth factor and HER2/neu in stage II colon cancer and correlation with survival. Clin Colorectal Cancer 4:262–267
Grossman SR, Lyle S, Resnick MB et al (2007) p66 Shc tumor levels show a strong prognostic correlation with disease outcome in stage IIA colon cancer. Clin Cancer Res 13:5798–5804
Hohenberger W, Weber K, Matzel K et al (2009) Standardized surgery for colonic cancer: complete mesocolic excision and central ligation—technical notes and outcome. Colorectal Dis 11:354–364 Discussion 364–365
Jakob C, Liersch T, Meyer W et al (2008) Predictive value of Ki67 and p53 in locally advanced rectal cancer: correlation with thymidylate synthase and histopathological tumor regression after neoadjuvant 5-FU-based chemoradiotherapy. World J Gastroenterol 14:1060–1066
Figueredo A, Charette ML, Maroun J et al (2004) Adjuvant therapy for stage II colon cancer: a systematic review from the Cancer Care Ontario Program in evidence-based care’s gastrointestinal cancer disease site group. J Clin Oncol 22:3395–3407
Gill S, Loprinzi CL, Sargent DJ et al (2004) Pooled analysis of fluorouracil-based adjuvant therapy for stage II and III colon cancer: who benefits and by how much? J Clin Oncol 22:1797–1806
Ogata Y, Murakami H, Sasatomi T et al (2009) Elevated preoperative serum carcinoembrionic antigen level may be an effective indicator for needing adjuvant chemotherapy after potentially curative resection of stage II colon cancer. J Surg Oncol 99:65–70
Burdy G, Panes Y, Alves A et al (2001) Identifying patients with T3–T4 node-negative colon cancer at high risk of recurrence. Dis Colon Rectum 44:1682–1688
Compton CC, Fielding LP, Burghart LJ et al (2000) Prognostic factors in colorectal cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med 124:979–994
Poincloux L, Durando X, Seitz JF et al (2009) Loss of Bcl-2 expression in colon cancer: a prognostic factor for recurrence in stage II colon cancer. Surg Oncol 18:357–365
Schetter AJ, Leung SY, Sohn JJ et al (2008) MicroRNA expression profiles associated with prognosis and therapeutic outcome in colon adenocarcinoma. JAMA 299:425–436
Bates RC, Bellovin DI, Brown C et al (2005) Transcriptional activation of integrin beta6 during the epithelial-mesenchymal transition defines a novel prognostic indicator of aggressive colon carcinoma. J Clin Invest 115:339–347
Nakamura T, Mitomi H, Kanazawa H et al (2008) Tumor budding as an index to identify high-risk patients with stage II colon cancer. Dis Colon Rectum 51:568–572
Logan-Collins JM, Lowy AM, Robinson-Smith TM et al (2008) VEGF expression predicts survival in patients with peritoneal surface metastases from mucinous adenocarcinoma of the appendix and colon. Ann Surg Oncol 15:738–744
AJCC Cancer Staging Handbook (2010), AJCC cancer staging handbook. 7th edn. New York, Springer
Burgess RE (1986) Carcinoembryonic antigen. Ann Intern Med 104:888 (letter to the editor)
Compton C, Fenoglio-Preiser CM, Pettigrew N et al (2000) American Joint Committee on Cancer Prognostic Factors Consensus Conference: Colorectal Working Group. Cancer 88:1739–1757
Locker GY, Hamilton S, Harris J et al (2006) ASCO 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer. J Clin Oncol 24:5313–5327
QUASAR Collaborative Group (2000) Comparison of flourouracil with additional levamisole, higher-dose folinic acid, or both, as adjuvant chemotherapy for colorectal cancer: a randomised trial. Lancet 355(9215):1588–1596
Andre T, Boni C, Navarro M et al (2009) Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol 27:3109–3116
Van Cutsem E, Labianca R, Bodoky G et al (2009) Randomized phase III trial comparing biweekly infusional fluorouracil/leucovorin alone or with irinotecan in the adjuvant treatment of stage III colon cancer: PETACC-3. J Clin Oncol 27:3117–3125
Park YJ, Park KJ, Park J-G et al (1999) Prognostic factors in 2230 Korean colorectal cancer patients: analysis of consecutively operated cases. World J Surg 23:721–726. doi:10.1007/PL00012376
Sener SF, Imperato JP, Chmiel J et al (1989) The use of cancer registry data to study preoperative carcinoembryonic antigen level as an indicator of survival in colorectal cancer. CA Cancer J Clin 39:50–57
Yeh CY, Hsieh PS, Chiang JM et al (2011) Preoperative carcinoembryonic antigen elevation in colorectal cancer. Hepatogastroenterology 58:1171–1176
Yang XQ, Chen C, Wang F-B et al (2011) Preoperative serum carcinoembryonic antigen, carbohydrate antigen19-9 and carbohydrate antigen 125 as prognostic factors for recurrence-free survival in colorectal cancer. Asian Pac J Cancer Prev 12:1251–1256
Huh JW, Oh BR, Kim HR et al (2010) Preoperative carcinoembryonic antigen level as an independent prognostic factor in potentially curative colon cancer. J Surg Oncol 101:396–400
Sun LC, Chu KS, Cheng SC et al (2009) Preoperative serum carcinoembryonic antigen, albumin and age are supplementary to UICC staging systems in predicting survival for colorectal cancer patients undergoing surgical treatment. BMC Cancer 9:288
Takagawa R, Fujii S, Mitsuoyshi O et al (2008) Preoperative serum carcinoembryonic antigen level as a predictive factor of recurrence after curative resection of colorectal cancer. Ann Surg Oncol 15:3433–3439
Roselli M, Guadagni F, Martini F et al (2003) Association between serum carcinoembryonic antigen and endothelial cell adhesion molecules in colorectal cancer. Oncology 65:132–138
Tabuchi Y, Deguchi H, Imanishi K et al (1987) Comparison of carcinoembryonic antigen levels between portal and peripheral blood in patients with colorectal cancer. Correlation with histopathologic variables. Cancer 59:1283–1288
Padilla D, Cubo T, Villarejo P et al (2007) Molecular profile of node-negative colorectal cancer of poor prognosis using immunohistochemical determination of p53, Ki67, VEGF, and metalloproteinase-9. Rev Esp Enferm Dig 99:424–425
Allegra CJ, Palk S, Colangelo LH et al (2003) Prognostic value of thymidylate synthase, Ki-67, and p53 in patients with Dukes’ B and C colon cancer: A National Cancer Institute-National Surgical Adjuvant Breast and Bowel Project collaborative study. J Clin Oncol 21:241–250
Ishida H, Miwa H, Tatsuta M et al (2004) Ki-67 and CEA expression as prognostic markers in Dukes’ C colorectal cancer. Cancer Lett 207:109–115
Visco V, Belleudi F, Marchese C et al (2004) Differential response to keratinocyte growth factor receptor and epidermal growth factor receptor ligands of proliferating and differentiating intestinal epithelial cells. J Cell Physiol 200:31–44
Graziano F, Cascinu S (2003) Prognostic molecular markers for planning adjuvant chemotherapy trials in Dukes’ B colorectal cancer patients: how much evidence is enough? Ann Oncol 14:1026–1038
Maksimovic S (2005) Laboratory-immunology indicators according as prognostic factors of patients with colon and rectum cancer. Med Arh 59:7–10
Sato H, Maeda K, Sugihara K et al (2011) High-risk stage II colon cancer after curative resection. J Surg Oncol 104:45–52
Prandi M, Lionetto R, Bini A et al (2002) Prognostic evaluation of stage B colon cancer patients is improved by an adequate lymphadenectomy: results of a secondary analysis of a large scale adjuvant trial. Ann Surg 235:458–463
Nanni O, Volpi A, Frassineti GL et al (2002) Role of biological markers in the clinical outcome of colon cancer. Br J Cancer 87:868–875
Caro JJ, Salas M, Ward A et al (2001) Anemia as an independent prognostic factor for survival in patients with cancer: a system[at]ic, quantitative review. Cancer 91:2214–2221
Author information
Authors and Affiliations
Corresponding author
Additional information
Y. Peng and L. Wang contributed equally in this work.
Rights and permissions
About this article
Cite this article
Peng, Y., Wang, L. & Gu, J. Elevated Preoperative Carcinoembryonic Antigen (CEA) and Ki67 Is Predictor of Decreased Survival in IIA Stage Colon Cancer. World J Surg 37, 208–213 (2013). https://doi.org/10.1007/s00268-012-1814-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-012-1814-7