
Abstract
Background
This study was designed to determine whether a preoperative fluorodeoxyglucose (FDG) positron emission tomography (PET) integrated with computed tomography (CT) (FDG-PET/CT) could be used as a guide for axillary node dissection (AND) or sentinel lymph node biopsy (SNB) in breast cancer patients.
Methods
Between February 2007 and April 2008, we performed FDG-PET/CT scans in 137 biopsy-proven breast cancer patients planning to have an SNB to select patients for either AND (PET/CT N+) or SNB (PET/CT N0). In performing SNB, we also performed additional non-SNB (ADD), which was enlarged at the lower axilla.
Results
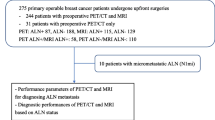
Twenty-seven patients with positive scans underwent complete AND as a primary procedure, and 110 patients with negative scans underwent SNB + ADD. There were 8 cases of false negative scans, and no case of false positive scan. The overall sensitivity, specificity, positive predictive value, and overall accuracy of FDG-PET/CT in predicting axillary metastasis were 77.1%, 100%, 100%, and 94.2%, respectively. In a subset of 110 patients with SNB + ADD, 104 patients had histologically negative SN, and 6 patients had positive SN in frozen section. Among 110 SNB + ADD cases, there were only 8 cases (7.3%) of positive axillary basins in permanent biopsy, including two cases of late positives that had micrometastases in the SN only. Through selective SNB + ADD based on an FDG-PET/CT, we have spared 27 unnecessary SNBs (true positive scans).
Conclusions
FDG-PET/CT is a specific imaging modality for predicting axillary node metastasis, and allows for a selective approach to either AND or SNB. A selective SNB + ADD based on an FDG-PET/CT reduced both unnecessary SNBs and positive axillary basins, enhancing the identification rates of SN and the accuracy of SNB.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Axillary lymph node dissection (AND) is the standard procedure for breast cancer patients with axillary node metastasis detectable through preoperative imaging or an intraoperative sentinel lymph node biopsy (SNB) [1, 2]. The relatively low sensitivity and specificity of the preoperative imaging methods makes them difficult to use as substitutes for SNB. At present, intraoperative SNB is the most accurate method for assessing axillary nodal status to determine whether or not to perform AND, and it has become the standard of care in clinically node negative early breast cancer [3, 4]. In performing an SNB, careful selection of patients is important because it is closely related to identification rates and false negative rates of SN. Sentinel nodes cannot be identified in patients with advanced disease because of either lymphatic blockage by tumor emboli or poor uptake of blue dye in SN that have been mostly replaced by tumor [5, 6]. Therefore, to enhance the identification rates of SN, clinically node-positive patients should be excluded as candidates for SNB. In patients with early breast cancer, the false negative rate of SNB is a very important problem in the current management of axilla. Among the causes of false negatives in SNB, skip metastasis (negative SN, but positive non-SN) results in regional recurrence, and late positives (showing negative results in the frozen section, but showing positive results in the permanent biopsy) necessitate delayed axillary dissection. Skip metastasis was found in 4%–10% of the patients with axillary metastases [7, 8]. Skip metastasis cannot be detected through SNB, even if performed in conjunction with serial sectioning, immunohistochemistry or reverse transcriptase polymerase chain reaction (RT-PCR) of SN. With the goal of reducing the need to perform unnecessary SNBs and the positive axillary basins that could result in either failure to identify SN or false negatives related to skip metastasis, we prospectively planned selective SNBs based on fluorodeoxyglucose (FDG) positron emission tomography (PET) integrated with computed tomography (CT) (FDG-PET/CT) scans in early breast cancer patients.
Patients and Methods
Patient population
This prospective study was approved by the review board of our institute. Written informed consent was obtained from all patients. Between February 2007 and April 2008, 137 consecutive patients with biopsy-proven early breast cancer and scheduled for SNBs took part in this study. All patients underwent a preoperative FDG-PET/CT examination, followed by definitive surgical treatment. Patients with ductal carcinoma in situ, with diabetes, who had received neoadjuvant chemotherapy, and who had undergone an excisional biopsy were excluded.
FDG-PET/CT imaging
All patients fasted for a minimum of 6 h to standardize blood glucose levels, and all of them had normal serum glucose levels (≤ 150 mg/dl). A noncontrast CT scan was performed 1 h after an intravenous injection of 7.4 MBq/kg (0.2 mCi/kg) of 18FDG in the arm contralateral to the breast cancer, for attenuation correction and for fusion with PET images using a GE Discovery LS scanner (General Electric Healthcare, ST-16, Milwaukee, WI). Imaging was acquired from the skull base to the proximal femur. Attenuation-corrected images were reconstructed in the transaxial, coronal, and sagittal planes and were interpreted by two experienced nuclear medicine physicians. Imaging results were reported as either positive or negative to describe the axillary nodal status. Images were reported to be positive if areas in the axillary basin took up more FDG than surrounding tissue through visual assessment. To allow for an objective assessment, the single-pixel maximal standardized uptake value (SUVmax) on any breast and axillary area was normalized to body weight as follows:
SUV = tissue concentration (MBq/kg) / [injected dose (MBq) / body weight (kg)]
Surgical procedures according to FDG-PET/CT imaging
The results of FDG-PET/CT scanning were used in surgical decision making with regard to management of the axilla (Fig. 1). After the induction of general anesthesia, lymphatic mapping was performed with the injection into the subareolar dermis of 5 ml 0.8% indigo carmine (Korea United Pharmaceutical, Seoul, South Korea), followed by gentle breast massage for 3 min. Five minutes after the blue dye injection, an approximately 3-cm-sized skin incision was made over the lower axilla. For the purpose of improving the accuracy of the SNB, we also performed an additional non-SNB, which was enlarged at the lower axilla at the same time as the SNB and sent for frozen section (Fig. 1). In addition to 2 mm slices of SN and non-SN from the intraoperative immediate frozen sections, the paraffin-embedded permanent sections were examined with hematoxylin-eosin (HE) staining. After completion of the SNB procedure, the primary tumor was removed. For those patients who had cancer cells in the SN or non-SN in their frozen section slides, a complete AND was performed. If no cancer cells were found in the SN and non-SN, the AND procedure was omitted.

Axillary treatment scheme according to visual assessment of fluorodeoxyglucose (FDG) positron emission tomography (PET) integrated with computed tomography (CT) (FDG-PET/CT) scan. AND, axillary node dissection; SNB, sentinel node biopsy; ADD, additional non-SNB. In the cases of positive axillary node metastasis by visual assessment of FDG-PET/CT, or positive SN or non-SN on frozen section, a complete AND was performed
Statistical analysis
The statistical parameters for FDG-PET/CT and SNB were calculated with the following formulas:
where TP = true positive, TN = true negative, FP = false positive, and FN = false negative.
Receiver operating characteristic (ROC) analysis was done to determine the optimal SUVmax threshold for surgical decision making with regard to AND or SNB.
Results
Clinicopathologic characteristics of the patients
A total of 137 newly diagnosed patients with operable breast cancers scheduled for SNBs were entered into the study. The characteristics of these patients are listed in Table 1. The mean diameter of the primary tumor in PET/CT N+ patients was 2.1 ± 0.1 (range: 0.3–4.9) cm, whereas that in PET/CT N0 patients was 1.7 ± 0.1 (range: 0.2–4.8) cm (p = 0.023, Independent-Samples t-test). A complete AND was performed in 33 patients, who had either positive scans (27 patients) or positive SN (6 patients), but AND was omitted for 104 patients with negative SN and non-SN in frozen sections (Table 2). Axillary nodal metastasis was confirmed in 35 cases through a pathology examination, and the remaining 102 patients had no axillary nodal metastasis (Table 2).
Prediction of AN status through FDG-PET/CT scans
Twenty-seven patients (19.7%) were suspected through FDG-PET/CT to harbor axillary metastases, and 110 patients (80.3%) showed negative results for axillary metastasis (Table 2). Patients with FDG-PET/CT positive node were subject to a complete AND without an SNB + ADD. There were 8 cases of false negative scans and no cases of false positive scans. Thus the positive predictive value was 100%. The mean SUVmax of the primary tumor in FDG-PET/CT N+ patients was 9.7 ± 0.9 (range: 1.9–23.7), whereas that in FDG-PET/CT N0 patients was 6.8 ± 0.5 (range: 1.5–22.7; p = 0.005, Independent-Samples t-test). An example of a positive FDG-PET/CT scan in a patient with multiple axillary node metastases is shown in Fig. 2. The overall sensitivity, specificity, and false negative rate of FDG-PET/CT in predicting axillary metastasis were 77.1% (27/35), 100% (102/102), and 22.9% (8/35), respectively (Table 3). In 129 of 137 patients (94.2%), FDG-PET/CT accurately identified positive or negative lymph node status. The eight cases of false negative FDG-PET/CT results are summarized in Table 4.

Preoperative FDG-PET and FDG-PET/CT images of a 69-year-old woman with right breast cancer suggest ipsilateral axillary lymph node metastases (solid arrow), and she also had an incidentally discovered case of gallbladder cancer (dotted arrow). A whole body FDG-PET scan (a, b) showed a focus of intense uptake in the right breast, axilla, and gallbladder. The measured SUVmax of the right breast mass was 11.5; axillary lymph nodes, 5.2; and gallbladder, 8.7. Coronal (c) and axial (d–f) slices of the FDG-PET/CT scan show a clearer anatomical relationship of axilla (d), breast (e), and fundus of gallbladder wall (f) than an FDG-PET scan
Value of selective SNB plus ADD based on FDG-PET/CT scans
Of the 137 patients examined in this study, 110 (75.2%) were classified as negative AN through the FDG-PET/CT (Table 2). SNBs were performed for all of these patients and identification rate of SN was 100%. The mean number of removed SN was 1.5 (range: 1–4). Additionally, at the lower axilla, a mean number of 2.5 (range 1–7) enlarged non-SNs were removed and sent for frozen sections, and two of 110 patients were positive for metastatic tumor cells in their frozen section slides (Table 4). The frozen sections of six out of 110 SNB +ADD patients had positive SN, and all of these patients subsequently underwent a complete AND. But out of the remaining 104 patients with negative SN results for their frozen sections, two patients were subsequently proven to have SN micrometastases on their permanent biopsy (late positive). The two patients with late positives also received adjuvant chemotherapy identical to node-positive patients, but delayed AND were omitted. The overall sensitivity, specificity, and false negative rate of SNB + ADD were 75.0% (6/8), 100% (102/102), and 25.0% (2/8), respectively (Table 3). In 108 of 110 patients (98.2%), selective SNB + ADD based on FDG-PET/CT accurately identified positive or negative lymph node status.
ROC analysis
The area under the ROC curve of axillary SUVmax was 0.882 (95% Confidence Interval [CI], 0.788–0.975; I = 0.000). With an SUVmax threshold of ≥3.85, sensitivity, specificity, and positive predictive value were 50%, 100%, and 100%, respectively. With an SUVmax threshold of less than 1.05, sensitivity, specificity, and negative predictive value were 100%, 33%, and 100%, respectively. The SUVmax cutoff point of 1.95 yielded almost equal sensitivity and specificity: 80.8% and 81.0%, respectively (Fig. 3). There were 17 patients with an SUVmax of ≥3.85 and 36 patients with an SUVmax of less than 1.05, which was almost equivalent to the surrounding normal tissue.

Ideal ranges of surgical decision making based on the receiver operating characteristic curve of axillary SUVmax. With an SUVmax cutoff value of above 3.85 (range of AND), the surgeon can proceed with AND directly. With an SUVmax cutoff value between 1.05 and 3.85 (range of SNB), SNB should be done to determine whether or not to perform AND. With an SUVmax cutoff value of less than 1.05, the surgeon can omit SNB. AUC the area under the curve
Detection of incidental tumors in other organs
Five patients underwent a combined operation for breast cancer and incidental tumors found through a preoperative FDG-PET/CT. These included 2 cases of thyroid cancer, 1 Klatskin tumor, 1 gallbladder cancer, and 1 large uterine myoma (Table 5).
Discussion
Most human cancers have demonstrated an affinity for fluorodeoxyglucose [9], and FDG-PET has been reported to have a relatively higher sensitivity and specificity than computed tomography (CT), magnetic resonance imaging (MRI), or ultrasound with regard to the axillary nodal status [10–12]. In addition, FDG-PET has the capability of detecting increased metabolic activity before any anatomic change occurs. One limitation of FDG-PET scanning has been a lack of precise anatomic information. Recently, however, FDG-PET imaging has been further refined with the development of FDG-PET/CT. The combination of FDG-PET with CT can provide detailed spatial localization of increased metabolic activity by the primary tumor and metastatic focus [13]. Ueda et al. reported the utility of 18F-FDG PET/CT for axillary staging: the diagnostic accuracy was 83% with 58% in sensitivity and 95% in specificity [14]. In the present study, the overall accuracy of FDG-PET/CT for axillary staging was 94.2% with 77.1% in sensitivity and 100% in specificity in 137 patients with early breast cancer. By performing AND as a primary procedure in the cases where there were positive FDG-PET/CT results, 27 patients were spared unnecessary SNB. In the literature, several studies of ultrasound guided fine-needle aspiration (FNA) cytology were reported for preoperative evaluation of axilla, with a sensitivity of 21%–89% and specificity of 93%–100% [15–18]. Sapino et al. [16] obtained high sensitivity (80%) and specificity (100%) because they did not exclude patients with palpable AN. In terms of accuracy, FDG-PET/CT is comparable to ultrasound guided FNA cytology for preoperative evaluation of axilla. In fat women or women with an accessory breast in the axilla, ultrasound has difficulties with transmission into fat tissue, which is not a problem in thin women. Another advantage of preoperative FDG-PET/CT is that it can be used for screening synchronous lesions in other organs at one stage, whereas ultrasound cannot. Visual assessment of FDG-PET/CT was more sensitive than quantitative analysis using SUVmax. With 100% specificity, visual assessment successfully identified 27 patients with axillary metastasis, whereas quantitative analysis identified 17 patients with axillary metastasis, who had an axillary SUVmax of ≥3.85. With 100% specificity, surgeons can proceed with AND directly without having to worry about performing an unnecessary procedure. With an increasing SUVmax threshold, specificity increased and sensitivity decreased (Fig. 3). In this situation, SNB could overcome the low sensitivity of FDG-PET/CT. Because of the limited sensitivity of FDG-PET/CT for the detection of small-sized nodal metastases, one might suggest lowering 18F-FDG uptake cutoff values to detect small metastatic AN. With an SUVmax threshold of less than 1.05, sensitivity reached 100%, which means SNB could be omitted because of complete absence of false negative (Fig. 3). There were 36 patients who had an axillary SUVmax less than 1.05, and these patients could be followed without SNBs. Actually, 8 cases of FDG-PET/CT false negatives were translated into 2 SNB late positives and 6 true positives (Table 3). The most likely explanation for the low sensitivity observed in the current study would be low tumor burden in axilla due to involvement of early stage breast cancer. Indeed, in several studies of patients with clinically node negative breast cancer, the sensitivity of FDG-PET for detection of AN metastases ranged from 25% to 50% [19–21]. Considering the 8 false negative cases of FDG-PET/CT in detecting axillary node metastasis, 5 patients had SN only micrometastases, but 3 had macrometastases (Table 4). Breast cancer with low tumor burden, such as micrometastasis or SN-only metastasis, and low FDG uptake tend to cause false negative scans. Failure to detect macrometastases may result from the low metabolic rate of tumor, which is an intrinsic tumor characteristic, such as type and grade [22–24]. Two of 3 false negatives in patients with macrometastases resulted from FDG uptake by the primary tumor, with SUVmax of 3.3 and 4.0. One of 3 patients with false negative results and with macrometastases had SN-only metastasis (Table 4). Selective SNB + ADD based on FDG-PET/CT resulted in low sensitivity (75.0%) and high false negative rates (25.0%) because of the 2 cases of late positives and small number of positive axillary basins (8 out of 110 SNB + ADD cases). These 2 cases of late positives had SN-only micrometastasis; however, delayed AND was omitted due to the following explanations. A large subset of patients with metastasis limited to the SN is unnecessarily subjected to the morbidity of AND because the incidence of non-SN involvement is low in SN that contains only micrometastatic foci [25]. Axillary recurrences and distant disease did not occur more frequently after an SNB alone in patients with negative SN or SN micrometastases, compared with breast cancer patients undergoing formal AND [26]. Furthermore, adjuvant chemotherapy or radiotherapy can effectively eradicate the micrometastatic foci. Decreased rates of positive axillary basins would have the effect of lowering the chances of false negatives related to skip metastasis in SNB. In a report by E. Barranger et al. [27], FDG-PET was found to reduce the false negative rate of SNBs through the detection of a skip metastasis that was only 3 mm in size. Although FDG-PET/CT cannot totally replace SNB, selective SNB + ADD based on FDG-PET/CT can reduce unnecessary SNBs by either performing AND as a primary procedure for patients with positive scan or omitting SNB for patients with an SUVmax of <1.05 (Fig. 3). Selective SNB + ADD based on FDG-PET/CT can reduce positive axillary basins, which have the effect of reducing false negatives related to skip metastasis. Based on our results, we do not consider that harvesting additional non-SN in the lower axilla is necessary for reducing skip metastasis.
In conclusion, FDG-PET/CT is a specific imaging modality for predicting axillary node metastasis that allows for a selective approach to either AND or SNB. Selective SNB + ADD based on FDG-PET/CT scan reduced both unnecessary SNBs and positive axillary basins, which enhanced the identification rates of SN and the accuracy of SNB. The systemic nature of FDG-PET/CT enables a one-stage evaluation of the whole body and subsequent treatment. Further endeavors to improve sensitivity and specificity will enhance the utility of FDG-PET/CT in the management of breast cancer.
References
Carmichael AR (2008) A randomized controlled clinical trial on sentinel node lymph node dissection versus axillary lymph node dissection: a matter of technique or patient selection? Ann Surg 248:895–896
Krag D, Weaver D, Ashikaga T et al (1998) The sentinel node in breast cancer: a multicenter validation study. N Engl J Med 339:941–946
Lovrics PJ, Chen V, Coates G et al (2004) A prospective evaluation of positron emission tomography scanning, sentinel lymph node biopsy, and standard axillary dissection for axillary staging in patients with early stage breast cancer. Ann Surg Oncol 11:846–853
Kumar R, Jana S, Heiba SI et al (2003) Retrospective analysis of sentinel lymph node localization in multicentric palpable and non-palpable breast cancer. J Nucl Med 44:7–10
Wong SL, Edwards MJ, Chao C et al (2002) The effect of lymphatic tumor burden on sentinel lymph node biopsy results. Breast J 8:192–198
Vargas HI, Vargas MP, Venegas R et al (2003) Lymphatic tumor burden negatively impacts the ability to detect the sentinel lymph node in breast cancer. Am Surg 69:886–890
Keskek M, Balas S, Gokoz A et al (2006) Re-evaluation of axillary skip metastases in the era of sentinel lymph node biopsy in breast cancer. Surg Today 36:1047–1052
Shivers S, Cox C, Leight G et al (2002) Final results of the department of defense multicenter breast lymphatic mapping trial. Ann Surg Oncol 9:248–255
Reske SN, Kotzerke J (2001) FDG-PET for clinical use: results of the 3rd German Interdisciplinary Consensus Conference. “Onko-PET III”, 21 July and 19 September 2000. Eur J Nucl Med 28:1707–1723
Kao CH, Hsieh JF, Tsai SC et al (2000) Comparison and discrepancy of 18F–2-deoxyglucose positron emission tomography and Tc-99 m MDP bone scan to detect bone metastasis. Anticancer Res 20:2189–2192
Kostakoglu L, Goldsmith SJ (2003) 18F-FDG PET evaluation of the response to therapy for lymphoma and for breast, lung, and colorectal carcinoma. J Nucl Med 44:224–239
Eubank WB, Mankoff DA, Vesselle HJ et al (2002) Detection of locoregional and distant recurrences in breast cancer patients by using FDG PET. Radiographics 22:5–17
Bockisch A, Brandt-Mainz K, Gorges R et al (2003) Diagnosis in medullary thyroid cancer with [18F]FDG-PET and improvement using a combined PET/CT scanner. Acta Med Austriaca 30:22–25
Ueda S, Tsuda H, Asakawa H et al (2008) Utility of 18F-fluoro-deoxyglucose emission tomography/computed tomography fusion imaging (18F-FDG PET/CT) in combination with ultrasonography for axillary staging in primary breast cancer. BMC Cancer 8:165
De Kanter AY, Van Eijck CHJ, Van Geel AN et al (1999) Multicentre study of ultrasonographically guided axillary node biopsy in patients with breast cancer. Br J Surg 86:1459–1462
Sapino A, Cassoni P, Zanon E et al (2003) Ultrasonographically guided fine-needle aspiration of axillary lymph nodes: role in breast cancer management. Br J Cancer 88:702–706
Motomura K, Inaji H, Komoike Y et al (2001) Gamma probe and ultrasonographically-guided fine-needle aspiration biopsy of sentinel lymph nodes in breast cancer patients. Eur J Surg Oncol 27:141–145
Kuenen-Boumeester V, Menke-Pluymers M, De Kanter AY et al (2003) Ultrasound-guided fine needle aspiration cytology of axillary lymph nodes in breast cancer patients. A preoperative staging procedure. Eur J Cancer 39:170–174
Guller U, Nitzsche EU, Schipr U et al (2002) Selective axillary surgery in breast cancer patients based on positron emission tomography with 18F-fluoro-2-deoxy-D-glucose: not yet! Breast Cancer Res Treat 71:171–173
Yang JH, Nam SJ, Lee TS et al (2001) Comparison of intraoperative frozen section analysis of sentinel node with preoperative positron emission tomography in the diagnosis of axillary lymph node status in breast cancer patients. Jpn J Clin Oncol 31:1–6
Van der Hoeven JJ, Hoekstra OS, Comans EF et al (2002) Determinants of diagnostic performance of [F-18] fluorodeoxyglucose positron emission tomography for axillary staging in breast cancer. Ann Surg 236:619–624
Wahl RL, Siegel BA, Coleman RE et al (2004) Prospective multicenter study of axillary nodal staging by positron emission tomography in breast cancer: a report of the Staging Breast Cancer with PET Study Group. J Clin Oncol 22:277–285
Fehr MK, Hornung R, Varga Z et al (2004) Axillary staging using positron emission tomography in breast cancer patients qualifying for sentinel lymph node biopsy. Breast J 10:89–93
Avril N, Rose CA, Schelling M et al (2000) Breast imaging with positron emission tomography and fluorine-18 fluorodeoxyglucose: use and limitations. J Clin Oncol 18:3495–3502
Fournier K, Schiller A, Perry RR et al (2004) Micrometastasis in the sentinel lymph node of breast cancer does not mandate completion axillary dissection. Ann Surg 239:859–863
Langer I, Marti WR, Guller U et al (2005) Axillary recurrence rate in breast cancer patients with negative sentinel lymph node (SLN) or SLN micrometastases: prospective analysis of 150 patients after SLN biopsy. Ann Surg 241:152–158
Barranger E, Grahek D, Antoine M et al (2003) Evaluation of fluorodeoxyglucose positron emission tomography in the detection of axillary lymph node metastases in patients with early-stage breast cancer. Ann Surg Oncol 10:622–627
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, J., Lee, J., Chang, E. et al. Selective Sentinel Node Plus Additional Non-Sentinel Node Biopsy Based on an FDG-PET/CT Scan in Early Breast Cancer Patients: Single Institutional Experience. World J Surg 33, 943–949 (2009). https://doi.org/10.1007/s00268-009-9955-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-009-9955-z