
Abstract
Background
We propose a new breast volume calculation method, treating the breast as an elliptical cone on craniocaudal and medial–lateral-oblique mammograms. This study aims to compare the accuracy and reproducibility of this proposed calculation method to the old Katariya method, which calculates breast volume as a circular cone on the craniocaudal mammogram only.
Materials and methods
From January 2005 to December 2006, 83 mastectomy patients with recorded breast weight and available preoperative mammographic films were included in the present study. Two surgeons independently measured breast height and width on the preoperative craniocaudal and medial–lateral-oblique mammograms. Breast volume was calculated as a circular cone in the craniocaudal view, and as an elliptical cone in both the craniocaudal and the medial–lateral-oblique mammograms. The accuracy of each method was determined and compared by linear regression analyses. Interobserver variability was assessed by bivariate correlation.
Results
The most accurate formula for calculating breast volume was the one that assumed the elliptical cone projection. The mean error of estimated breast volume using the elliptical cone (EC) formula is 3.8 cm3 (standard deviation [SD] = 133 cm3). The mean error of traditional circular cone (CC) formula is −51.3 cm3 (SD = 182 cm3). From a linear regression model, the correlation coefficient of estimated breast volume using EC formula measured 0.977, whereas that using the CC formula measured 0.952 (Fig. 1). Measurements were reproducible between the two independent observers; the Pearson correlation for the EC formula is 0.93 (p < 0.001), and that for the CC formula is 0.95 (p < 0.001).
Conclusions
Breast volume can be accurately determined from measurements made on mammograms. The proposed EC formula calculating breast volume on both the craniocaudal and the medial–lateral-oblique mammograms may be more accurate, as the horizontal and vertical dimensions of the breast are not always the same. In addition, height measurement on the medial–lateral-oblique film can eliminate the compression error as the craniocaudal film may miss the base of the breast and underestimate the breast volume. Taking both mammogram views for measurement is comparably reproducible to the traditional method. Reproducibility of measurement can be further enhanced by better defining the point of measurements.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
With increasing emphasis on the cosmetic outcome of breast surgery, the role of breast volume estimation becomes more important. It helps the surgeon predict the esthetic effect of various breast surgeries on women, and guides the choice of the most appropriate treatment.
Various methods of breast volume estimation have been described. These include displacement methods [1, 2], external casting [3], and anthropometric measurements [4, 5]. Breast volume estimation using mammography has been previously described [6–9]. Because mammography is a common investigative tool for patients with breast cancer, mammographic estimation is a readily available option for which no additional equipment is needed. It also allows preoperative estimations of breast volume, which are invaluable in planning operations.
Mammographic estimation of breast volume has previously been considered by Katariya’s group [7]. According to their original method, breasts are considered as circular cones for volume estimation. Height and diameter of breasts were obtained from the craniocaudal view of mammograms, to which the formula of circular cones volume was applied for estimation. As the base of breast is more often an ellipse rather than a regular circle, it is not uncommon to encounter large discrepancies between the diameters obtained from the craniocaudal view and the medial–lateral-oblique view of mammography. In the study, we proposed an elliptical modification (EC formula) of the Katariya method (CC formula) of mammographic breast volume estimation. We evaluated the accuracy and reproducibility of estimations using this modified method.
Patients and methods
We retrospectively reviewed the mammograms and operative records of patients who underwent mastectomies in the period January 2005 to December 2006. Patients with recorded specimen weight and available preoperative mammograms were included in the study. We only included patients with mammograms that contained nonmagnified images.
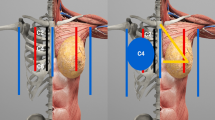
Height of breast (h) and width of breast base (2r) were determined by direct measurement on the mammograms (Fig. 1). Height of breasts from both the craniocaudal view (h CC ) and the medial–lateral-oblique view (h MLO ) mammograms was defined as the longest perpendicular distance from the pectoralis major to the skin adjacent to the nipple. Width of breast was defined separately for mammograms in the craniocaudal view and the medial–lateral-oblique view. Width in craniocaudal view (2r CC ) was established as the maximum horizontal distance from the medial side to the lateral side of the breast, as recorded on the mammograms. Width in medial–lateral-oblique view (2r MLO ) was the distance from lateral thoracic artery to where the skin crosses the pectoralis major.

Measurement on craniocaudal view and medial–lateral-oblique view mammograms. h MLO height of breast in medial–lateral-oblique view mammogram, h CC height of breast in craniocaudal view mammogram, 2r MLO width of breast base in medial–lateral-oblique view mammogram, 2r CC width of breast base in craniocaudal view mammogram
The estimated breast volume was calculated using both the original Katariya method (CC formula: 1/3π r 2 CC h CC ) and our modified formula (EC formula: 1/3π r CC r MLO h MLO ). The basic difference between Katariya’s method and our method is the difference in geometric assumptions. In our modified version, breast volume is estimated by assuming breasts to be elliptical cones rather than circular cones. All the mammographic measurements were done individually by two surgeons.
Recorded weight was the weight of specimens from either simple mastectomy or modified radical mastectomy (MRM), as noted in the operative record of patients. Since all MRM specimens contained axillary content, making them unavoidably heavier than simple mastectomy specimens, a generic adjustment of MRM specimen weight was made by subtracting 50 g from the recorded weight. The specimen volume was then calculated from specimen weight using the density of 0.958 g/cm3. This density was based on the assumption that breasts were equally composed of fibroglandular tissues, which has a density of 1 g/cm3, and of fatty tissue, which has a density of 0.916 g/cm3.
The accuracy and reproducibility of breast volume estimation using the CC formula and the EC formula was then measured. For accuracy, the mean value of estimated breast volumes by the two observers was taken. We then noted the mean error of estimated volume from specimen volume. The degree of linear association between estimated breast volume and specimen volume was also analyzed by linear regression. For reproducibility, the interobserver differences in various breast measurements and bivariate correlation of estimated breast volume by the observers were noted. All statistical calculations were performed with SPSS version 13 (Chicago, IL).
Results
A total of 139 patients underwent mastectomy in our center within the study period. Specimen weight and mammographic films were retrievable in 81 patients. Because two of the patients had bilateral disease and underwent bilateral mastectomy, there were 83 samples suitable for further analysis: 13 simple mastectomies and 70 MRMs.
The mean age of the patients was 57 (standard deviation [SD] = 14). The mean specimen volume was 568 cm3 (SD = 236). The mean estimated breast volume with the CC formula and the EC formula was 517 and 572 cm3, respectively. The mean error of estimated volume from specimen volume was −51.3 cm3 (SD = 182) by the CC formula and 3.8 cm3 (SD = 133) by the EC formula (Table 1).
We created a scatter plot of the specimen volume against the estimated breast volume by the two methods (Fig. 2). From this graph, we are convinced that a linear relationship existed between the estimated breast volume and specimen volume. We used linear regression to analyze this relationship. The correlation coefficient (R) of the estimated breast volume with the EC formula was 0.977, and that using the CC formula was 0.952. The regression equation from both estimation methods was also obtained. They both have slope approaching 1 (1.025 for the CC formula, and 0.966 for the EC formula).

Linear correlation of estimated breast volume and specimen volume
The interobserver difference in breast measurements made in the craniocaudal view and the medial–lateral-oblique view is shown in Table 2. A higher percentage difference is noted between observers in all breast measurements taken from the medial–lateral-oblique view mammograms. The Pearson correlation coefficient of the estimations by the two observers using the Katariya method was 0.949 (p < 0.001), while that using elliptical method was 0.926 (p < 0.001).
Discussion
The mathematical principle behind Katariya’s original method for mammographic breast volume estimation is to assume breasts as circular cones. This method is based on measurements made on craniocaudal view mammograms, which are more consistent between different observers. However, for women with large breasts, the base of the breast can sometimes be missed in craniocaudal view mammograms, leading to underestimation of both the height and the width of the breast [10]. In addition, experience from measuring mastectomy specimens showed that the base of the breast looks more like an ellipsis than a circle. Such observations inspired us to modify the Katariya method, applying it to the elliptical cone model, in order to address these issues.
The accuracy of both the original and elliptical estimations was assessed in this study. Both methods of estimation achieved very good correlation with the specimen volume, with Pearson correlation coefficients above 0.95. For error of estimation, the mean error using the EC formula was 3.8 cm3, in comparison with a mean error of −51.3 cm3 using CC formula. This indicates that the volume estimates using the elliptical cone method are slightly more accurate.
We have also assessed the reproducibility of measurements and estimations between observers. A greater interobserver percentage difference was noted in measurements made on medial–lateral-oblique view mammograms. The correlation of results between the two observers using both estimation methods was also noted, with a slightly inferior correlation noted when the EC formula was used.
In their study, Kalbhen et al. noted that the measurements made on medial–lateral-oblique view mammograms were less reproducible than those made on craniocaudal view images [9]. He suggested that the variable amount of axillary tissue present in medial–lateral-oblique view mammograms could make subsequent measurements liable for interobserver variation. In the present study, the medial–lateral-oblique measurements were made using the shadow of lateral thoracic artery as reference point. Theoretically, this could improve the interobserver variability by avoiding measurement of axillary content. However, such a method is less straightforward and requires additional training before practical use. As reflected in this study, a relatively greater mean percentage difference in medial–lateral-oblique measurements is still present. We believe that this problem could be overcome with additional experience and practice.
There are potential limitations to this study. Specimen volume was obtained by conversion of specimen weight using the assumed breast tissue density of 0.958 g/cm3. This assumption may not be true in every individual, as the amount of adipose and fibroglandular tissue within the breast varies among women [6]. Nevertheless, as the maximum error arising from inaccurate assumption of breast density is only 4%, we believe such systematic error should be negligible. In addition, breast volume is known to vary within menstrual cycle, which was not taken into account in this study [11]. Because both breast imaging and operation were both performed without regard to menstrual cycle in practice, such an effect was not specifically controlled in order to reflect a more realistic situation.
Conclusions
In conclusion, we have applied an elliptical cone model for breast volume estimation in mammograms. This method of estimation is as accurate and reproducible as the traditional method proposed by Katariya and colleagues. The accuracy of such measurements is invaluable for breast surgeons and breast cancer patients in choosing their suitable treatment options.
References
Bouman FG (1970) Volumetric measurement of the human breast and breast tissue before and during mammoplasty. Br J Plast Surg 23:263–264
Ward C, Harrison B (1986) The search for volumetric symmetry in reconstruction of the breast after mastectomy. Br J Plast Surg 39:379–385
Campaigne BN, Katch VL, Freedson P et al (1979) Measurement of breast volume in females: description of a reliable method. Ann Hum Biol 6:363–367
Smith DJ Jr, Palin WE Jr, Katch VL et al (1986) Breast volume and anthropomorphic measurements: normal values. Plast Reconstr Surg 78:331–335
Loughry CW, Sheffer DB, Price TE et al (1989) Breast volume measurement of 598 women using biostereometric analysis. Ann Plast Surg 22:380–385
Stomper PC, D’Souza DJ, DiNitto PA et al (1996) Analysis of parenchymal density on mammograms in 1353 women 25–79 years old. AJR Am J Roentgenol 167:1261–1265
Katariya RN, Forrest AP, Gravelle IH (1974) Breast volumes in cancer of the breast. Br J Cancer 29:270–273
Keddy RJ, Brebner DM (1980) Negative development xeroradiography of the breast: doses and clinical indications. Br J Radiol 53:325–330
Kalbhen CL, McGill JJ, Fendley PM et al (1999) Mammographic determination of breast volume: comparing different methods. AJR Am J Roentgenol 173:1643–1649
Cochrane RA, Valasiadou P, Wilson AR et al (2003) Cosmesis and satisfaction after breast-conserving surgery correlates with the percentage of breast volume excised. Br J Surg 90:1505–1509
Graham SJ, Stanchev PL, Lloyd-Smith JO et al (1995) Changes in fibroglandular volume and water content of breast tissue during the menstrual cycle observed by MR imaging at 1.5 T. J Magn Reson Imaging 5:695–701
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fung, J.T.K., Chan, S.W.W., Chiu, A.N.K. et al. Mammographic Determination of Breast Volume by Elliptical Cone Estimation. World J Surg 34, 1442–1445 (2010). https://doi.org/10.1007/s00268-009-0283-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-009-0283-0