
Abstract
Background
Gastroesophageal reflux (GER) is common in children with congenital diaphragmatic hernia (CDH), and the optimal management in these patients is not well established. The aim of this study was to assess whether a preventive fundoplication performed during the first surgery will improve GER and nutritional morbidity in patients with a left CDH.
Methods
Thus we studied one group of 17 patients treated with a one-step antireflux procedure (group A) and a group of 19 patients with only initial diaphragmatic repair (group B) between January 1994 and December 2004. The patients were classified in three stages, mild intermediate and severe form, based on anatomic criteria (liver position and patch requirement). Most of the patients with the severe form of disease were in group A. Clinical charts were compared between the two groups with a mean follow-up of 3 years.
Results
For patients with intra-abdominal liver and direct diaphragmatic closure, the duration of hospitalization was significantly longer in group A than in group B (p = 0.08). The incidence of GER was significantly lower in group A (17.6%) than in group B (52.6%) at 1-year follow-up (p < 0.5). In the last group, 30% required a fundoplication before 6 months. Seven patients (19%) required intermittent nutritional supplementation via nasogastric tube feeding; for these patients there was no difference between the two groups. A gastrostomy was performed in only one patient. Twelve percent of patients had growth retardation during most of their first year, again with no difference between the two groups.
Conclusions
Based on the published data, recommendations can be made regarding the efficacy of adding an antireflux surgery procedure to left CDH repair in only patients with intrathoracic liver and/or patch requirement.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastroesophageal reflux (GER) is common after congenital diaphragmatic hernia (CDH) repair, occurring in 28%–69% of patients [1–6]. It has been recognized as a significant contributing factor, delaying both artificial ventilation and hospitalization in CDH survivors [3, 4, 6]. The mechanisms responsible for pathological GER in this condition remain poorly established, but 15%–70% of the affected CDH patients remain symptomatic under medical treatment, and thus require surgical correction [1–5, 7]. Koot et al. [4] and Sigalet et al. [8] have supported Nissen fundoplication in early infancy if there is no result with medical therapy. We previously proposed performance of preventive fundoplication at the time of CDH repair [3].
The aim of the present study was to assess the efficiency of such a one-step surgical procedure in CDH repair.
Materials and methods
Materials
This is a retrospective study of 70 neonates admitted to our institution for CDH between 1994 and 2004. Fifty-seven of these infants were born in our hospital and 13 were referred postnatally. Sixty-three had a left-sided hernia; 18 of them died prior to surgery and 40 survived after 3 months. Four were discharged to other centers after their CDH repair. We reviewed the medical charts of the 36 remaining cases with a mean follow-up of 3 years (range: 6–132 months).
The infants in this series included 22 boys and 14 girls. The mean birth weight was 2,834 g (1,710–4,150 g; median, 2,875 g); the mean gestational age was 37.3 weeks (32–41 weeks; median, 38 weeks). Eleven patients had associated congenital anomalies, including three with neurological disease. High-frequency oscillatory ventilation (HFO) was used in 25 patients and nitric oxide (NO) inhalation support was required in 20. No extracorporeal membrane oxygenation was used.
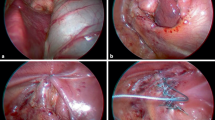
Surgical repair was performed through a subcostal abdominal incision. The diaphragmatic defect was repaired with direct closure in 20 patients and with a prosthetic patch in 16 patients. The surgery included a fundoplication in 17 cases (10 Nissen and 7 partial wrap) according to the surgeon’s option and peropertative hemodynamic stability. No gastrostomy tube was placed during the initial surgery.
Methods
We defined two groups of patients: group A when in which initial antireflux procedure was performed and group B in which no initial antireflux procedure was performed. In each group, we noted the following items:
-
Anatomical form: mild (when the diaphragmatic defect was repaired with direct closure and the liver was in an intra-abdominal position), intermediate (when the diaphragmatic defect was repaired using a prosthetic patch or the liver was in an intrathoracic position), severe (when the diaphragmatic defect was repaired using a prosthetic patch and the liver was in an intrathoracic position).
-
Duration of artificial ventilation
-
Duration of parenteral nutrition
-
Duration of hospitalization
-
Ponderal status (growth retardation was defined as weight under fifth percentile compared with the reference curves of Sempé)
-
Need for enteral nutrition support after hospitalization
-
Incidence of GER, assessed by clinical investigation, upper gastrointestinal UGI) series, 24-hour pH monitoring, or endoscopies.
Twenty-three of the 36 patients had had at least one GER investigation during the first year of life, 10 in group A and 13 in group B (Table 1).
Pathological GER was defined as follows:
-
persistent vomiting and recurrent respiratory symptoms despite medical treatment
-
pH of less than 4.0 for more than 5% of the time monitored
-
moderate and severe GER revealed by UGI
-
endoscopic biopsies showing at least moderate esophagitis
Statistical analysis was performed using the chi-square test (with continuity correction) and Fischer’s exact test for categorical data, and the Mann-Whitney test for continuous data. A p value of less than 0.05 was considered significant.
Results
Population
The significant differences between groups A and B were the presence of intrathoracic stomach herniation and hernia sac, which was significantly more frequent in group A. The two groups were therefore evaluated as homogeneous groups (Table 2). There were 16 patients with mild disease and 13 patients with the intermediate anatomical form; their repair carried out for patients in the two groups was similar. Six of the seven patients with a severe form of CDH were treated with a one-step fundoplication. One patient with this form could not have a fundoplication because of a hemodynamic instability during the diaphragmatic repair.
Postoperative care
There was no significant difference between the two groups in terms of duration of mechanical ventilation and parenteral nutrition. Table 3 shows that the duration of hospitalization was significantly longer in group A than in group B, but only for patients with the mild anatomical form of the disease (p = .008).
Seven patients had recurrent herniation during their first year of life, four with a severe form of CDH in group A and one with each anatomical form in group B. All patients were alive at a mean follow-up of 3 years.
Incidence of GER
Twelve of the 17 patients in group A and 6 of 19 patients in group B did not have any clinical problems and no proven pathological GER during the first year of life (p = .02). The incidence, during this period, of a proven pathological GER was 17.6% (3 patients of 17) in group A and 52.6% (10 patients of 19) in group B with a significant difference (p = .04).
Durations of artificial ventilation, parenteral nutrition, and hospitalization in group B were significantly longer for infants with pathological GER than for those without pathological GER (Table 4). We could not find a statistically significant correlation between anatomical form and GER in this group (Table 5).
Three patients with severe proven pathological GER in group B were lost to follow-up after one year. In this group, a patient with the severe form did not have a one-step fundoplication because of peroperative hemodynamic instability. He underwent surgical treatment for pathologic GER at 3 months of age. Two other group B patients with the intermediate form required a Nissen fundoplication during their first 5 months of life.
All patients in group A with pathological postoperative GER responded well to medical therapy. No initial fundoplication broke down within the 3-year follow-up.
Nutritional morbidity
There was no dysphagia after the 20 fundoplications. Three of the 17 patients in group A and 1 of the 16 patients in group B with a severe form had growth retardation after the first year of life. In group A, 2 patients had a severe anatomical CDH form and the other one had a mild form.
Seven patients required intermittent nutritional supplementation via nasogastric tube feeding without difference between the two groups. None of them had a mild anatomical form and 6 had a patch repair. The mean duration of this nutrition was significantly shorter for the 4 patients in group A (6–12 months; median, 10 months) than for the 3 patients in group B (18–108 months; median, 54 months) with a significant difference (p = 0.03). Only one patient with neurological disease in group A required placement of a gastrostomy tube.
Discussion
The association of proven GER and CDH has been described in prospective studies with an incidence in survivors ranging from 55% to 68% [4, 6]. It seems to be an important contributing factor in the overall morbidity of CDH. Despite the risk of GER requiring antireflux surgery after CDH repair, the efficacy of a preventive one-step fundoplication procedure has not been reported in the published literature. As in other studies, our patients with proven GER after diaphragmatic repair had a significantly longer duration of initial hospital stay than those without [3, 4, 9].
Severe GER after CDH repair may require fundoplication with a reported incidence of 44% to 57% [1, 5]. Several theories have been offered for physiopathology of GER in this population and may explain the high failure rate of medical treatment [3, 6, 8, 10–15]. Because GER seems to depend on several anatomical factors, we tried to establish a classification to define at-risk patients. We did not consider the position of the stomach in this classification, but the contribution of this factor to an association of postoperative GER remains controversial in survivors of CDH [1, 3, 9, 16]. Like Fasching et al. [1] and Koot et al. [4], we could not find, in our series, any parameter that could predict GER. However, there was a trend toward an increase in the incidence of proven gastroesophageal reflux in our patients with a thoracic liver and/or a patch repair, treated without initial fundoplication, but this was not statistically significant.
The results of this study demonstrate that patients with CDH who undergo initial fundoplication have significantly less pathological proven GER during early infancy than those treated with a standard CDH repair. Nevertheless, for patients with the mild anatomical form of CDH, the hospital stay was longer if preventive antireflux procedures had been performed. Therefore we suggest that preventive anti-reflux surgery is not effective in these patients.
We found that fundoplication in these infants is technically feasible even if the gastric fundus may in a few patients be too small to be wrapped circumferentially around the esophagus. Nevertheless the feasibility of this procedure may be limited by hemodynamic instability during the surgery in patients with severe CDH.
Failure to thrive is frequently described in CDH survivors with an incidence ranging from 20% to 56% [2, 5, 13, 17–19]. Growth failure in CDH patients is multifactorial, in part secondary to chronic lung disease, GER, and oral aversion. Moreover, in a retrospective analysis of CDH survivors, Muratore et al. [5] reported that extracorporeal membrane oxygenation (ECMO) was a predictive factor of growth failure during the first year of life. Our reported incidence of failure to thrive among patients with CDH after one year of age is only 11%. One explanation for this low rate may be that the majority of our children with growth retardation had a severe anatomical form of CDH but none of them was treated with ECMO. Another explanation might be that a preventive antireflux procedure was used in 48% of these infants.
The management of these patients is difficult, and there is no consensus in the literature [2, 5, 20]. Thirty-three percent of patients in the study by Muratore et al. [5] required a gastrostomy tube for supplemental feeding. However, we were very restrictive, compared to other authors, in performing gastrostomy because it may increase the risk of oral aversion [2].
Conclusions
This study points out the need to establish a classification in the CDH population for the management of GER. The pattern of the at-risk patient for pathological GER emerging from our study involves either use of a prosthetic patch during CDH repair or location of the liver in an intrathoracic position. The advantages of our proposed classification in 3 stages (mild, intermediate, and severe) lie in its simplicity based on anatomical criteria and the fact that it will be useful when comparing results.
From results of the present study, we therefore recommend that during repair of CDH, a preventive one-step antireflux procedure should be performed only in selected patients with the intermediate or severe anatomical form of CDH. Fundoplication is a feasible and effective procedure in very young infants with primary GER, and it may have an important palliative role in facilitating feeding in further selected cases.
References
Fasching G, Huber A, Uray E et al (2000) Gastroesophageal reflux and diaphragmatic motility after repair of congenital diaphragmatic hernia. Eur J Pediatr Surg 10:360–364
Jaillard SM, Pierrat V, Dubois A et al (2003) Outcome at 2 years of infants with congenital diaphragmatic hernia: a population-based study. Ann Thorac Surg 75:250–256
Kieffer J, Sapin E, Berg A et al (1995) Gastroesophageal reflux after repair of congenital diaphragmatic hernia. J Pediatr Surg 30:1330–1333
Koot VC, Bergmeijer JH, Bos AP et al (1993) Incidence and management of gastroesophageal reflux after repair of congenital diaphragmatic hernia. J Pediatr Surg 28:48–52
Muratore CS, Utter S, Jaksic T et al (2001) Nutritional morbidity in survivors of congenital diaphragmatic hernia. J Pediatr Surg 36:1171–1176
Stolar CJ, Levy JP, Dillon PW et al (1990) Anatomic and functional abnormalities of the esophagus in infants surviving congenital diaphragmatic hernia. Am J Surg 159:204–207
Nagaya M, Akatsuka H, J Kato (1994) Gastroesophageal reflux occurring after repair of congenital diaphragmatic hernia. J Pediatr Surg 29:1447–1451
Sigalet DL, Nguyen LT, Adolph V et al (1994) Gastroesophageal reflux associated with large diaphragmatic hernias. J Pediatr Surg 29:1262–1265
Khalaf MN, Porat R, Brodsky NL et al (2001) Clinical correlations in infants in the neonatal intensive care unit with varying severity of gastroesophageal reflux. J Pediatr Gastroenterol Nutr 32:45–49
Beaudoin S, Kieffer G, Sapin E et al (1995) Gastroesophageal reflux in neonates with congenital abdominal wall defect. Eur J Pediatr Surg 5:323–326
Cohen MD, Beck JM (1980) Hiatus hernia: a complication of postero-lateral diaphragmatic herniation (Bochdalek hernia) in infants. Clin Radiol 31:215–219
Koivusalo A, Rintala R, Lindahl H (1999) Gastroesophageal redux in children with a congenital abdominal wall defect. J Pediatr Surg 34:1127–1129
Naik S, Greenough A, Zhang Y et al (1996) Prediction of morbidity during infancy after repair of congenital diaphragmatic hernia. J Pediatr Surg 31:1651–1654
Qi B, Soto C, Diez-Pardo JA et al (1997) An experimental study on the pathogenesis of gastroesophageal reflux after repair of diaphragmatic hernia. J Pediatr Surg 32:1310–1313
Takamatsu H, Akiyama H, Noguchi H et al (1991) Association of hiatus hernia with postero-lateral diaphragmatic hernia (Bochdalek’s hernia). Eur J Pediatr Surg 1:244–246
Kamiyama M, Kawahara H, Okuyama H et al (2002) Gastroesophageal reflux after repair of congenital diaphragmatic hernia. J Pediatr Surg 37:1681–1684
Chiu PP, Sauer C, Mihailovic A et al (2006) The price of success in the management of congenital diaphragmatic hernia: is improved survival accompanied by an increase in long-term morbidity? J Pediatr Surg 41:888–892
Crankson SJ, Al Jadaan SA, Namshan MA et al (2006) The immediate and long-term outcomes of newborns with congenital diaphragmatic hernia. Pediatr Surg Int 22:335–340
Lund DP, Mitchell J, Karasch V et al (1994) Congenital diaphragmatic hernia: the hidden morbidity. J Pediatr Surg 29:258–262 discussion 262–264
Vanamo K, Rintala R, Sovijärvi A et al (1996) Long-term pulmonary sequelae in survivors of congenital diaphragmatic defects. J Pediatr Surg 31:1096–1099
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chamond, C., Morineau, M., Gouizi, G. et al. Preventive Antireflux Surgery in Patients with Congenital Diaphragmatic Hernia. World J Surg 32, 2454–2458 (2008). https://doi.org/10.1007/s00268-008-9738-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-008-9738-y