
Abstract
Gastroduodenal outlet obstruction is a complication of advanced gastrointestinal malignant disease. In the past it was usually treated by an open surgical bypass procedure. During the last decade, endoscopic self-expandable stents (SEMS) have been used. The aim of this study was to compare these two palliative strategies concerning clinical outcome and health economy. A series of 36 patients with incurable malignant disease and gastroduodenal outlet obstruction syndrome were treated in a prospective study. According to the attending hospital and endoscopist on duty, 21 of the 36 patients were endoscopically treated with SEMS and 15 underwent an open surgical gastroenteroanastomosis. Health economic evaluation was based on the monetary charges for each patient associated with the procedure, postoperative care, and hospital stay. The hospital stay was 7.3 days for the stented group compared with 14.7 days for the open surgery group (p > 0.05). The survivals were 76 and 99 days, respectively (NS). In the stented group all 15 patients (100%) alive after 1 month were able to eat or drink, and 11 (73%) of them tolerated solid food. In the surgical bypass group,9 out of 11 (81%) patients alive after 1 month could eat or drink, and 5 of them (45%) could eat solid food. The mean charges (U.S. dollars) during the hospital stay were $7215 for the stented group and $10,190 for the open surgery group (p < 0.05). Palliation of the gastroduodenal obstruction in patients with malignant disease were at least as good, and the charges were lower for the endoscopic stenting procedure than for an open surgical bypass.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Gastroduodenal outlet obstruction is often a complication of advanced malignant disease in the upper gastrointestinal tract. Gastric retention with nausea, vomiting, and nutritional problems adds to the already deteriorated well-being of the patient. In the past, the only available treatment has been surgical exploration. In cases of incurable disease, the operative alternatives were palliative resection or gastroenteroanastomosis, sometimes together with bypass of the bile ducts or intestines. Many patients with obstruction of the upper gastrointestinal (GI) tract are so affected by their disease, however, that open surgery is either not an alternative or can be carried out only at high risk. During the last decade expandable stents for enteral use have been developed that offer palliation. They are not only useful for patients unsuited for surgery and general anesthesia, they serve as a less invasive alternative that can be performed under conscious sedation [13].
There are quite a few albeit small studies of upper GI enteral stenting [4, 5]. These studies mostly focused on the technical aspects of the stenting procedure. The number of studies comparing the functional outcome between open bypass surgery and enteral stenting in the upper GI tract are limited. Functional outcome and costs are important variables when new techniques are adopted. It is also important to evaluate the functional outcome over a long period of time and, in case of palliative treatment, during the patient’s remaining lifetime. The same is true for costs, as high initial costs may be justified if additional costs are low.
The aims of the present study were to evaluate the lifelong results of the stenting procedure and to compare it with the performance of surgical bypass procedures conducted during the same time period. Study variables were complications, postoperative food intake, and procedure-related economic costs.
Materials and Methods
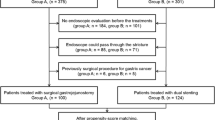
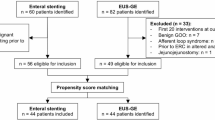
Between 1999 and 2004 a series of 36 consecutive patients with an outlet obstruction of the upper GI tract due to incurable malignant disease were treated at our institution, which is located at two different hospitals. The 21 consecutive patients with incurable malignant disease were treated with a gastroduodenal stent by one of two surgeons familiar with the stenting procedure. During the same period 15 patients underwent an open gastroenteroanastomosis. In the latter patients there was either preoperative uncertainty about the possibility of a radical resection, or they were treated by surgeons not familiar with gastroduodenal stenting or at the hospital where the stenting procedure had not been adopted. There was no active selection when choosing the method. All patients treated by stenting, however, had been diagnosed with incurable malignant disease preoperatively. The characteristics and comparability between the study groups are given in Table 1.
All patients had a history of upper GI retention. In the stented group, two patients were able to drink limited amounts but did not tolerate puree or solid food. In the open surgery group, four patients tolerated limited intake of liquid or puree.
Upper GI endoscopy was performed to locate the stricture. When a stricture was suspected further distally, a small-bowel radiography study was performed. Patients with a stricture of the distal small bowel did not undergo the stenting procedure.
Stenting was performed in the endoscopy unit. Patients were sedated with midazolam (Dormicum; Roche) and pethidine (Petidin; Pharmacia/Upjohn). A diagnostic endoscope (Olympus GIF-Q60) was advanced to the stricture, and a guidewire (Jagwire Super stiff Jagwire, Boston Scientific/Microvasive) was passed through the stricture. An endoscopic retrograde cholangiopancreatography (ERCP) catheter (Tandem XL; Boston Scientific/Microvasive) was advanced into the stricture over the guidewire, and the distal end of the stricture was located by injecting contrast medium (Omnipac 180 mg/ml; Nycomed Amersham) under fluoroscopic guidance. The length of the stricture was estimated by measuring the length of the catheter retrieved through the stricture. A stent 2 to 3 cm longer than the stricture was chosen. After withdrawing the endoscope, a therapeutic endoscope (Olympus GIF-2T20) with a 10F working channel was inserted over the guidewire. The stent was put in position by fluoroscopic and endoscopic guidance. The stents used (Wallstent Enteral Unistep; Boston Scientific/Microvasive) had a fully open diameter of 22 mm and a length of 60 or 90 mm.
Patients in the stent group were followed prospectively, and data concerning postoperative food intake was collected by interviews with a study nurse. In the open surgery group retro- or antecolic anastomosis or closure of the stomach distal to the anastomosis was performed depending on the surgeon’s choice. Data from these patients were collected retrospectively from hospital files. Patient in both groups were followed until they died.
Patients with strictures in the descending part of the duodenum had a percutaneous transhepatic bile duct stent placed before the enteral stenting procedure regardless of whether hyperbilirubinemia was present or not. Patients with previous endoscopic bile duct stenting or tumor growth close to the extrahepatic bile ducts underwent bile duct bypass performed at open surgery. When open surgery was performed, strictures of the GI tract distal to the duodenum were treated with an intestinal bypass if there was suspicion of an impending obstruction.
In both groups, patients were allowed to drink without restriction from the first postoperative day. Intake of puree and solid food was introduced individually according to the patient’s tolerance. Complications postoperatively and the need for additional surgical or endoscopic procedures were recorded together with the duration of the stay in the postoperative care unit, the in-hospital stay, and survival.
A procedure-related health economic evaluation was performed based on the charges associated with the procedures together with the charges for the stay in the postoperative care unit and the hospital stay. Charges for endoscopic and open surgical procedures during follow-up as well as the hospital stay associated with these procedures were included. In the surgery group the procedure cost was based on the time in the operating theater including all costs for theater staff and extra equipment such as staplers. The stented group costs were based on the cost of the endoscopic procedure, the cost of the stents and other equipment (e.g., ERCP catheters, guidewires), and the cost of the percutaneous transhepatic bile duct stenting.
The analyses were based on intention to treat, so all costs for the patient were assigned their initial group. Background data for the health economic evaluation are given in Table 2.
Benefit from the procedure was defined as a change in the clinical course after the procedure, leading to complete oral feeding or a change in the level of care (e.g., from hospital care to a nursing home) due to improved oral intake. Patents were classified as benefiting from the procedure or not.
Oral intake was recorded after 1 week and then 1, 2, and 3 months postoperatively.
Statistics
Nonparametric tests (e.g., Mann-Whitney U-test) were used for statistical analyses.
Results
There were no major differences concerning background characteristics, including diagnosis and location of the stricture. Details are given in Table 1.
The stent placement procedure was successful in all cases. In four patients the first stent was not long enough to pass the stricture, so an additional stent was inserted during the same procedure. In two cases the stent was placed too far distally, resulting in dislocation of the stent. This was discovered early postoperatively, and another stent was placed during a second session.
One patient underwent gastroenteroanastomosis 5 days after the stenting procedure owing to continued gastric retention; she died 6 days after the open surgery because of general weakness due to her malignant disease. One patient had a massive tumor hemorrhage 3 weeks after stent placement and underwent palliative resection. In two patients there was tumor growth through the stent after 6 months resulting in obstruction. It was treated with restenting. In one patient there was a stent obstruction due to impacted food, which was removed by upper GI endoscopy. No other complications were noted in the stent group.
Twelve patients had an antecolic route of the enteral limb, and three patients had closure of the stomach distal to the anastomosis during open surgery.
One patient in the gastroenteroanastomosis group was reoperated 1 month after the first procedure due to remaining gastric retention. Operative findings showed a massive peritoneal carcinosis and the patient underwent gastrostomy. Another patient in this group was treated with percutaneous endoscopic gastrostomy for the same reason.
Transhepatic bile duct stenting was performed in three patients before gastroduodenal stenting. One of these patients had hyperbilirubinemia. Among the patients treated with open surgery, two had an additional biliary-enteric bypass, and two patients had an intestinal bypass. None of these patients, however, had manifested jaundice or small intestinal or colonic mechanical obstructions at the time of surgery. The tumor location, however, suggested impending biliary or intestinal obstruction.
None of the patients required a stay in the postoperative care unit or intensive care unit (ICU) after the stenting procedure; the mean ICU stay after open surgery was 0.9 day (0–1 day). The mean postoperative hospital stay was 7.3 days (1–28 days) for the stented group compared with 14.7 days (6–48 days) for the gastroenteroanastomosis group (p < 0.05, Mann-Whitney U-test). Six patients in the stent group died within 30 days compared with four in the surgery group. No deaths were due to complications related to the surgical procedure. The mean survival after stent placement was 76 days (4–215 days) compared with 99 days (6–337 days) for the surgery group. The difference was not significant. Table 3.
Data on food intake are given in Figure 1. All 15 (100%) patients in the stent group who were alive after 1 month were able to eat or drink, and 11 (73%) of them could eat puree or solid food. The corresponding figures for the patients in the open surgery group are 9 of 11 (81%) and 5 of 16 (45%). Sixteen (76%) patients who underwent the stenting procedure were classified as having benefited from the procedure compared with six (40%) in the gastroenteroanastomosis group (Fig. 2).The mean charges during the hospital stay for the primary procedure were, for the stenting procedure, 64,939 Swedish kronors (SEK), or 7215 U.S. dollars (USD), compared to 91,712 SEK (10,190 USD) for the surgery group (p < 0.05) (Fig. 3). Charges for the initial procedure and all additional procedures until the patient died were 73,463 SEK (8163 USD) and 92014 SEK (10,224 USD) (NS) for the stented group and the open surgery group, respectively.

Oral intake after stenting procedure (a) and after open surgical gastroenteroanastomosis (b). Data are numbers of patients and percent of the group.

Patients who benefit from stenting and open surgical bypass procedure after the initial hospitalization. Benefit from the procedure was defined as a change in the clinical course leading to complete oral feeding or to a lower level of care. Number of patients and percentages are given.

Health economic evaluation of the two treatment strategies for costs during the initial hospital stay. Costs are based on all charges associated with the procedure plus charges for postoperative care and hospital use. 1 USD = 9 SEK.
Discussion
The present study indicates that gastroduodenal stents are valuable tools for restoring “feeding ability” in patients with advanced upper GI cancers. It also suggests that the results are at least equal to those seen with the open surgical bypass procedure but at a lower cost.
Our results showing good palliation with gastroduodenal stents are in accord with the findings of others [5, 6, 7, 8, 9, 10]. Our patients, however, had more eating problems before stent placement than is usually reported: As many as 90% of our patients could ingest nothing per os. The results thus demonstrate that stents are effective in patients with severe obstruction.
The literature regarding open surgery for gastroenteroanastomoses in symptomatic patients report a high frequency of complications and a poor outcome [11, 12, 13]. Modern surgery probably is associated with fewer complications, though, as suggested by our and other studies [14, 15]. A commonly reported problem with gastroenteroanastomoses is the long time (some times a few weeks) before they start to function [16, 17]. This probably is due to diminished motility in the dilated stomach and the unphysiologic passing of food. We noted a similar trend in our limited study population, although the time to resuming oral intake was shorter in the stented group. One explanation could be the more physiologic conditions for food passage in that group. Excluding the tumor-bearing portion distal to the gastroenteroanastomosis with a linear staple has been advocated to diminish this problem. Three of our patients were operated on with this technique [18, 19].
Although this was not a randomized study, the two groups were treated during the same time period and the treatment strategy selected depended only on the part of the city in which the patients lived and thus which of the two hospitals the patients attended. This protocol provided a good basis for comparison between the groups. In addition, however, a few patients who, after preoperative workup, might have had a curative resection were instead treated by a surgical bypass procedure. Some patients deemed unfit for operation underwent the endoscopic stenting procedure. Therefore patients in the open surgery group had somewhat less tumor burden and were somewhat younger than patients in the stented group.
Patients with stents underwent meticulous follow-up, whereas the costs for the open surgery group were extracted from the hospital charts. Their costs therefore may be underestimated.
Procedure-related costs could probably not be reduced further in the open surgery group, whereas the cost of stenting probably can be decreased. The use of multiple stents will decrease as experience with the procedure increases.
The costs were significantly lower for the stented group during the initial hospital stay. When calculating the costs for the patients remaining lifetime there was still a difference to the benefit of the stented group, although not statistically significant. This can be explained by the need for additional procedures in the stented group, but it may also be a result of the study design. Underestimation of costs in the open surgery group as previously mentioned is a possible explanation. For example, the costs of parenteral nutrition were not available owing to the study design. Another explanation could be the fact that home care palliative teams and hospice staff consider surgery to be the ultimate step and do not recognize the need for additional operative or endoscopic measures.
Advances in preoperative diagnostics will hopefully further diminish the number of patients who undergo exploratory laparotomy. Based on the findings of the present study, only patients who are potential candidates for curative resection and those with additional enteral stenosis should be considered for open surgery. Under these circumstances, however, a liberal approach to gastrointestinal bypass procedures have been suggested for patients with unresectable pancreatic cancer [20]. These patients have an extremely short mean survival time. In the present study, the mean survival was only 3 months in the best group. Therefore, it is impossible to determine whether patients with a long (> 6 months) life expectancy would do better with a gastroenteroanastomosis than with a stent. On the other hand, feeding ability was better in the stent group at all investigated time points.
An advantage of the stenting procedure is that an advanced abdominal tumor burden usually does not complicate or make the procedure impossible as it sometime does for open surgery or laparoscopy. Therefore stenting is probably a good alternative for patients with an advanced tumor burden. A future randomized study comparing the costs, functional outcome, and tumor biology of laparoscopic bypass and stenting procedures is needed.
Résumé
Le syndrome d’obstruction post-pylorique est une des complications des maladies malignes gastro-intestinales avancées. Par le passé, on les traitait habituellement par une dérivation chirurgicale traditionnelle. Pendant cette dernière décennie, les stents à expansion posés par voie endoscopique sont une solution alternative de plus en plus utilisée (SEMS). Les buts de cette étude ont été de comparer ces deux stratégies palliatives du point de vue de l’évolution clinique et économique. Trente six patients présentant une maladie maligne incurable et un syndrome d’obstruction post-pylorique ont été traités dans cette étude prospective. Selon l’hôpital et l’endoscopiste de garde, 21 de ces patients ont eu un stent « SEMS » et 15 ont eu une anastomose gastro-intestinale chirurgicale traditionnelle. L’évaluation économique des soins a été basée sur les coûts de chaque patient associés à l’intervention, les soins postopératoires et la durée de séjour. La durée de l’hospitalisation a été de 7.3 jours pour le groupe « SEMS » comparée à 14.7 jours pour le groupe de chirurgie par voie traditionnelle (p > 0.05). La survie a été de 76 et 99 jours, respectivement (n.s.). Les 15 patients du groupe ë SEMS » sont tous (100%) en vie après un mois et ils pouvaient manger et/ou boire; 11 (73%) parmi eux toléraient des aliments solides. Dans le groupe de dérivation chirurgicale, 9 sur 11 (81%) pouvaient manger et/ou boire après un mois et cinq (45%) toléraient des aliments solides. Les coûts moyens pendant la durée de séjour ont été de 7215 dollars US pour le groupe ë SEMS» et de US $10,190 pour le groupe chirurgie traditionelle (p < 0.05). Comparée aux dérivations chirurgicales tradtionnelle, la palliation endoscopique de l’obstruction gastroduodénale maligne est au moins aussi bonne et les coûts sont moindres.
Resumen
La obstrucción de la desembocadura gastroduodenal es una complicación de la enfermedad neoplásica maligna. En el pasado ha sido tratada mediante una derivación quirúrgica abierta. En la última década se han venido utilizando “stents” autoexpandibles. El propósito del presente estudio fue comparar estos dos métodos paliativos en cuanto al resultado clínico y el costo. 36 pacientes con enfermedad maligna incurable y síndrome de obstrucción gastroduodenal fueron tratados en el presente estudio. Según el hospital y el endoscopista de turno, 21 de ellos recibieron “stents” y 15 fueron sometidos a gastroenteroanastomosis abierta. La evaluación económica se hizo con base en los cargos asociados con el procedimiento, el cuidado postoperatorio y la estancia hospitalaria. La estancia hospitalaria fue de 7.3 días para el grupo de “stents” y de 14.7 días para el grupo de la cirugía abierta (p > 0.05). La supervivencia fue de 76 días y 99 días, respectivamente (n.s.). En el grupo de “stents” la totalidad de los 15 pacientes (100%) vivos al mes de efectuado el procedimiento pudieron comer o beber y 11 (73%) toleraron alimentos sólidos; 9 de 11 (81%) pudieron comer o beber al mes de practicada la derivación quirúrgica y 5 (45%) pudieron comer alimentos sólidos. El promedio de los costos durante la hospitalización fue de 7,215 dólares americanos en el grupo de “stents” y US $10,190 en el grupo de la cirugía abierta (p < 0.05). La paliación de la obstrucción gastroduodenal en la neoplasia maligna es por lo menos tan buena y los costos son menores con los procedimientos de “stent” en comparación con la derivación quirúrgica abierta.
References
TH Baron (2001) ArticleTitleExpandable metal stents for the treatment of cancerous obstruction of the gastrointestinal tract N. Engl. J. Med. 344 1681–1687 Occurrence Handle10.1056/NEJM200105313442206 Occurrence Handle1:STN:280:DC%2BD3Mzht1yltA%3D%3D Occurrence Handle11386268
MA Mauro RE Koehler TH Baron (2000) ArticleTitleAdvances in gastrointestinal intervention: the treatment of gastroduodenal and colorectal obstructions with metallic stents Radiology 215 659–669 Occurrence Handle1:STN:280:DC%2BD3c3ptlChug%3D%3D Occurrence Handle10831681
CL Zollikofer R Jost E Schoch et al. (2000) ArticleTitleGastrointestinal stenting Eur. Radiol. 10 329–341 Occurrence Handle10.1007/s003300050053 Occurrence Handle1:STN:280:DC%2BD3c7jtV2hsg%3D%3D Occurrence Handle10663766
K Mergener RA Kozarek (2002) ArticleTitleStenting of the gastrointestinal tract Dig. Dis. 20 173–181 Occurrence Handle10.1159/000067488 Occurrence Handle12566620
CA Ely ME Arregui (2003) ArticleTitleThe use of enteral stents in colonic and gastric outlet obstruction Surg. Endosc. 17 89–94 Occurrence Handle10.1007/s00464-002-8809-7 Occurrence Handle1:STN:280:DC%2BD3s%2FmtFKjtg%3D%3D Occurrence Handle12360374
M Kaw S Singh H Gagneja et al. (2003) ArticleTitleRole of self-expandable metal stents in the palliation of malignant duodenal obstruction Surg. Endosc. 17 646–650 Occurrence Handle10.1007/s00464-002-8527-1 Occurrence Handle1:STN:280:DC%2BD3s7nvFGmtw%3D%3D Occurrence Handle12404051
DG Adler TH Baron (2002) ArticleTitleEndoscopic palliation of malignant gastric outlet obstruction using self-expanding metal stents: experience in 36 patients Am. J. Gastroenterol. 97 72–78 Occurrence Handle11808972
R Razzaq HU Laasch R England et al. (2001) ArticleTitleExpandable metal stents for the palliation of malignant gastroduodenal obstruction Cardiovasc. Intervent. Radiol. 24 313–318 Occurrence Handle10.1007/s00270-001-0031-9 Occurrence Handle1:STN:280:DC%2BD38%2FosFymtw%3D%3D Occurrence Handle11815836
JH Kim BM Yoo KJ Lee et al. (2001) ArticleTitleSelf-expanding coil stent with a long delivery system for palliation of unresectable malignant gastric outlet obstruction: a prospective study Endoscopy 33 838–842 Occurrence Handle10.1055/s-2001-17340 Occurrence Handle1:STN:280:DC%2BD3MrisVWlsg%3D%3D Occurrence Handle11571678
HB Yim BC Jacobson JR Saltzman et al. (2001) ArticleTitleClinical outcome of the use of enteral stents for palliation of patients with malignant upper GI obstruction Gastrointest. Endosc. 53 329–332 Occurrence Handle10.1067/mge.2001.112842 Occurrence Handle1:STN:280:DC%2BD3Mzgt1WgsA%3D%3D Occurrence Handle11231392
NN Lo SG Kee R Nambiar (1991) ArticleTitlePalliative gastrojejunostomy for advanced carcinoma of the stomach Ann. Acad. Med. Singapore 20 356–358 Occurrence Handle1:STN:280:By2D38jksFw%3D Occurrence Handle1718211
PD Rooij ParticleDe A Rogatko MF Brennan (1991) ArticleTitleEvaluation of palliative surgical procedures in unresectable pancreatic cancer Br. J. Surg. 78 1053–1058 Occurrence Handle1718529
DW Weaver RG Wiencek DL Bouwman et al. (1987) ArticleTitleGastrojejunostomy: is it helpful for patients with pancreatic cancer? Surgery 102 608–613 Occurrence Handle1:STN:280:BieD3MfltVc%3D Occurrence Handle2443991
KD Lillemoe JL Cameron JM Hardacre et al. (1999) ArticleTitleIs prophylactic gastrojejunostomy indicated for unresectable periampullary cancer? A prospective randomized trial Ann. Surg. 230 322–330 Occurrence Handle10.1097/00000658-199909000-00005 Occurrence Handle1:STN:280:DyaK1MvitFahsA%3D%3D Occurrence Handle10493479
TA Sohn KD Lillemoe JL Cameron et al. (1999) ArticleTitleSurgical palliation of unresectable periampullary adenocarcinoma in the 1990s J. Am. Coll. Surg. 188 658–669 Occurrence Handle10.1016/S1072-7515(99)00049-6 Occurrence Handle1:STN:280:DyaK1M3osFyqsA%3D%3D Occurrence Handle10359359
SD Woods GJ Mitchell (1989) ArticleTitleDelayed return of gastric emptying after gastroenterostomy Br. J. Surg. 76 145–148 Occurrence Handle1:STN:280:BiaC1Mvntl0%3D Occurrence Handle2702446
RC Doberneck GA Berndt (1987) ArticleTitleDelayed gastric emptying after palliative gastrojejunostomy for carcinoma of the pancreas Arch. Surg. 122 827–829
Y Nakata K Kimura N Tomioka et al. (1999) ArticleTitleGastric exclusion for unresectable gastric cancer Hepatogastroenterology. 46 2654–2657 Occurrence Handle1:STN:280:DyaK1MvltFGgsQ%3D%3D Occurrence Handle10522059
BJ Ammori B Boreham (2002) ArticleTitleLaparoscopic devine exclusion gastroenterostomy for the palliation of unresectable and obstructing gastric carcinoma Surg. Laparosc. Endosc. Percutan. Tech. 12 353–355 Occurrence Handle10.1097/00129689-200210000-00009 Occurrence Handle12409703
TP Wade TJ Neuberger TJ Swope et al. (1994) ArticleTitlePancreatic cancer palliation: using tumor stage to select appropriate operation Am. J. Surg. 167 208–213 Occurrence Handle10.1016/0002-9610(94)90075-2 Occurrence Handle1:STN:280:ByuC2cvntV0%3D Occurrence Handle7508687
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Johnsson, E., Thune, A. & Liedman, B. Palliation of Malignant Gastroduodenal Obstruction with Open Surgical Bypass or Endoscopic Stenting: Clinical Outcome and Health Economic Evaluation. World J. Surg. 28, 812–817 (2004). https://doi.org/10.1007/s00268-004-7329-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-004-7329-0