
Abstract
Experience with the use of nylon fishing line for surgical sutures has been reported from several African countries. A recent publication suggested that fishing line and an injection needle may provide an atraumatic suture that is especially suitable for intracutaneous skin closures. This article provides further empirical support for such alternative technology. We describe a randomized, blinded clinical trial conducted in Butare (Rwanda) with 220 cutaneous wounds closed by intracutaneous sutures, with either the homemade suture or a commercial nylon thread (Ethilon). We compared the clinical outcomes as well as the costs of those two materials. There are no significant differences between the two sutures in terms of clinical findings or in the reported ease of use by the surgeons. The cost of a homemade atraumatic suture is US $0.07, which is less than one-thirtieth the cost of the commercial thread. The advantage of the commercial thread is the assurance of quality. We consider whether this quality assurance justifies the large price difference, and if the homemade suture should be recommended to surgeons in countries where the costs of surgical material often remain an obstacle for life-saving operations.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
The lack of surgeons and of material for surgical procedures limit access to adequate surgical treatment in Rwanda and many other African countries. There are increasing efforts to address the lack of surgeons through better training programs in several countries [1]. On the other hand, out-of-pocket payments for treatment and for the materials needed during surgical procedures are commonly requested from the patients themselves, thereby limiting their access to necessary medical attention. With increasing efforts to privatize the cost by introducing fee-for-service procedures in poor countries, surgery is becoming less available for the poor population. In some places even vital operations are performed only after a prepayment for surgical materials; such demands are lethal for some patients [2]. Costs for staff in poor counties are relatively low compared to the costs of surgical supplies, which are mostly imported. In developing countries the costs of surgical suture material constitutes one-third of the material costs for a given operation [3]. Reducing those costs should be a priority.
Efforts are needed to identify, evaluate, and promote affordable alternative surgical materials. The use of inexpensive fishing nylon thread has been proclaimed for hernia repair and abdominal wall and skin closures [4, 5, 6, 7]. Nevertheless, the use of cost-saving fishing nylon has not been widely accepted. The need to introduce the thread into traumatic needles with less sharpness than the single-use atraumatic needles may account for this lack of acceptance.
A technique for the self–production of sharp, nontraumatic, single-use armed sutures with the same benefits as the commercial products has recently been described [8]. This development may motivate surgeons to use this cost-reducing technique. To compare these two suture materials—homemade fishing line sutures and commercial nylon (Ethilon)—a clinical trial was initiated at the University Hospital of Butare in Rwanda.
MATERIALS AND METHODS
Fishing-line suture
Self-production of atraumatic sutures is simple. All that is needed is an injection needle and nylon fishing line. In our study a 23.5-gauge injection needle (Microlence; B. Braun; Tuttlingen, Baden Württemberg, Germany) and 0.25 mm fishing nylon from the local market (ultramid, or polyamid 6/6; BASF, Ludwigshafen, Rheinland–Pfalz, Germany) were used. The manufacturer of the fishing nylon confirmed the purity of the nylon (without additive or coating of the surface) –(BASF, quality assurance no. 8900300). To produce the atraumatic suture, the line is threaded into the cavity of the needle and fixed by squeezing its end with a clamp after having broken off the hub (Fig. 1). The thread is wrapped in gauze and autoclaved with the other surgical instruments.

Technique for self-production of an atraumatic intracutaneous suture. a. The suture is threaded through the sharp opening of the injection needle. b. The hub is broken from the needle by repeated bending at their junction, and it is removed by pulling it over the suture. c. The proximal end of the needle is pinched with the lock of a needle holder to fix the suture to the needle. d. The final product is a homemade atraumatic suture.
Commercial suture
The least expensive commercial surgical thread for skin closure is nylon. In this study Ethilon 3-0 (polyamid 6/6; Johnson & Johnson, New Brunswick, NJ, USA) was used with an FS 2 needle. Size 3-0 corresponds to a diameter of 0.200 to 0.249 mm and is comparable to that of the fishing line.
The costs in Rwanda of both sutures were recorded. The cost of the homemade suture included the salary of the local producer on a per-unit basis.
Patients
The study was approved by the Ethical Commission of the University in Butare. Included were all patients of all ages with uninfected surgical or traumatic wounds (grade I and II) at any site of the body. A precondition was that the surgeon judged that the wound could be closed by an intracutaneous suture. Multiple wounds on one patient were randomized separately. An agreement form had to be filled out and signed by the patient or his or her guardian. The primary endpoint was the difference in mean wound scores between those closed with the commercial suture versus those closed with the homemade suture. A significant difference of less than 5% between the two suture groups was regarded as not clinically meaningful. The sample size (200 cases) was calculated on the basis of a two-sample t-test, with a power of 0.8 and allowing a type I error of 0.05. From November 2002 to March 2003 a total of 199 patients with 220 wounds were recruited consecutively.
Skin Closure
If necessary, the wound was débrided. Hemostasis was achieved to the extent possible. The surgeon then decided whether the wound could be closed by an intracutaneous suture. If so, the wound was randomized using standard random number tables (Microsoft Exel), and either the fishing line suture (group A) or the commercial suture (group B) was used to perform a Halsted’s intracutaneous continuous skin closure. The wound was covered with gauze that was changed daily until removal of the suture, and only then was the patient informed about which suture had been used.
Observations
The baseline characteristics were recorded: sex, age, main diagnosis, the patient’s American Society of Anesthesiologists classification (ASA 1–4), the wound site, and the contamination grade (only class I and II). The qualifications of the surgeons (fully trained, in training, nurse) were evaluated and recorded, as were the time (in seconds per centimeter) they required for suturing, and their opinions regarding their handling of the suture. The axillary temperature of the patients was recorded daily. One surgeon who was not involved in the skin closures and not informed about the identity of the suture material used on the patients questioned the patients about pain and itching of the wound and checked for tenderness. He registered any complications and assessed the wounds at day 3 and on the day of suture removal using the Hollander wound score. This score describes objective and subjective signs of wound disturbances [9]. As erythema is difficult to evaluate in dark skin, the scoring method had to be modified (Table 1). The quality of the wound healing was classified as not disturbed (0–1 score = class A), having minor disturbance (2–4 score = class B), or having major disturbance (> 4 score = class C). The ends of the sutures emerging from both ends of the wounds were covered with Band-Aids before scoring to allow a blind evaluation. Finally, the ease of suture removal was evaluated, noting whether additional traction was required or if the suture tore. This part of the test could not be performed in a blind manner.
Statistical Methods
The underlying statistical methods were mostly descriptive. In some cases, however, standard tests for analyzing differences between the groups (fishing line versus Ethilon) were performed. A χ2 test was used to compare frequencies, the t-test and analysis of variance (ANOVA) to compare the mean parameter values among the study groups, and rank-sums tests for nonparametric approaches.
RESULTS
Baseline Characteristics
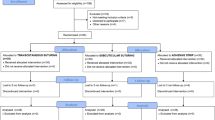
Among the initial 220 wounds enrolled in the study, 20 were eliminated owing to death of the patient (n = 3), checkout without further consultation (n = 10), or violation of the protocol (n = 8). Altogether, 200 wounds were included in the statistical evaluation.
There were no significant differences in the baseline characteristics between the group of patients sutured with fishing line (group A) and the group of patients sutured with commercial thread (group B) (Table 2).
Outcome
There was a significant difference in the time needed for suturing, depending on the qualifications of the surgeon, but no significant difference was found regarding the time needed for suturing in group A (62.85 s/cm) or group B (55.7 s/cm) (p = 0.6449). The opinion of the surgeons about handling the sutures was mostly positive for both materials (83% very practical), and there were no differences between suture groups (p = 0.6449) (Table 3). Problems associated with removing the suture were observed in 14 cases in group A (9 minor and 5 major problems) and 17 in group B (13 minor and 4 major problems). There was no significant difference between groups A and B (p = 0.72). Remarks on the patients’ charts indicated that accidental knots due to technical mistakes or backstitches during suturing were mostly responsible for these difficulties.
Among all wounds, 80.5% healed normally or with only minor disturbance. Healing (i.e., the number of wound healing points, classes A–C), was significantly associated with the length of the wound (p < 0.01); it was associated with the grade of contamination (grade I-II) (p = 0.06); the patients’ general condition (ASA status) (p = 0.07) was of borderline significance. There was no significant association with the site of the wound, the sex or age of the patient, or the quality of the suture material (p = 0.99) (Tables 3, 4).
Costs
A 3-0 Ethilon suture with a cutting needle costs US $2.30 if it is imported by Rwanda. The total per unit cost (US) of the homemade fishing-line suture is $0.07, which is 3% of the price of the commercial suture. This is based on the following calculations: 100 m of 0.25 mm fishing nylon cost (US) $1.10, or $0.006 for 50 cm. The price for a 23.5-gauge injection needle in Rwanda is $0.04. The price of the wrapping gauze is not calculated, as it is used later for the wound dressing. To produce and wrap 100 atraumatic fishing rope sutures takes 80 minutes, or 48 seconds per suture. The salary (including all costs) of a nurse in Butare is US $220 per month, corresponding to a labor cost of less than US $0.02 to make one suture.
DISCUSSION
Reports about the use of fishing line for surgical sutures have never been validated through clinical trials. In previous publications fishing line was used not only for skin closures but also for sutures that remain in the body, such as for abdominal closures or hernia repairs [4, 5, 6, 7]. In all these reports, traumatic reusable needles requiring introduction of the thread into an eyelet were used. The trauma of the reusable larger needles is an argument against this kind of suturing. With the homemade sutures and integrated needles, however, it is now possible to provide an option comparable to the use of commercial atraumatic sutures.
The results of the present study show that both sutures were rated as “practical” or “very practical” by all surgeons. No significant additional time was required for either suture. Regarding the clinical appearance of subjective symptoms, inflammatory reactions, wound infections, and removal of the sutures, there were no significant differences between the two materials. No difference in clinical effects could thus be identified in the trial comparing the homemade fishing line suture and the commercial one.
The only identifiable differences between the two sutures are their cost and the quality assurance offered by the commercial brand. Regarding the price difference, the money spent for one commercial thread would allow 30 surgical skin closures to be performed with the homemade fishing line suture. The implied savings to a surgical unit under circumstances where the price for the material of a cesarean section is around $20 is that every tenth operation could be performed for free.
It has been argued that the use of hollow needles carries a high risk that the surgeon might contract the human immunodeficiency virus (HIV) or hepatitis infection after an accidental needle puncture compared to the use of solid needles [9]. Although the risk is low, it is not negligible. It is therefore recommended that the nylon thread be inserted through the whole channel of the needle to minimize the collection of blood or other infectious material in the needle. Regardless of this additional risk, operations on HIV- or hepatitis-positive patients should be performed with special preventive strategies [10] and be reserved for surgeons with a minimal rate of puncture accidents.
The development of more affordable, locally adapted surgical materials is needed worldwide and for developing countries in particular. Quality assurance (QA) is important, as it offers valid, sustainable confirmation of manufacturing purity for a given product. International QA standards for health devices are high but unlikely to justify or account for the 30-fold difference in price between the two suture products. The outcome of the trial suggests that for these homemade sutures, which were sterilized prior to use, quality was more than adequate. Local production of cost-saving sutures such as those described in this article require compliance with appropriate QA standards but offer an affordable product nonetheless. Local production by surgical units warrants exploration.
Résumé
Des expériences avec l’emploi de ligne à pêche pour des sutures chirurgicales ont été rapportées de plusieurs pays africains. Une récente publication d’une méthode de fabrication domestique de sutures avec de la ligne à pêche et une aiguille à injection présente une suture atraumatique particulièrement appropriée pour la fermeture intracutanée de blessures de la peau. Cet article décrit une expérience randomisée et aveugle réalisée à Butare (Rwanda) avec 220 blessures cutanées fermées par des sutures intracutanées avec une suture de fabrication domestique ou avec un fil de nylon commercial (Ethilon). Les résultats cliniques et le coût de ces deux matériaux sont ensuite comparés. Il n’existe pas de différences significatives entre les deux sutures quant aux résultats cliniques ou quant à la facilité d’usage pour les chirurgiens. Le coût de la suture produite à la maison est de US $0.07, moins d’un trentième du coût du fil commercial, l’avantage du dernier étant la garantie de qualité. Il est discuté si cette garantie justifie l’immense différence de prix et si la suture de fabrication domestique devrait être recommandée aux chirurgiens dans des pays où le coût du matériel chirurgical représente souvent un obstacle pour des opérations vitales.
Resumen
Experiencias con el uso de sedal para suturas quirúrgicas han sido publicadas desde varios paises Africanos. Una publicación reciente de un método de producción artesanal de suturas con sedal de pesca y una aguja hipodérmica presenta una sutura atraumatica particularmente apropiada para el uso intracutáneo. Este artículo describe un ensayo clínico randomizado y ciego, realizado en Butare (Rwanda) en 220 heridas de piel que fueron cerradas mediante técnica intracutánea utilizando bien la sutura de fabricación artesanal o bien un hilo comercial de nilón (Ethicon), y compara tanto los resultados clínicos como el costo de estos dos materiales. No hubo diferencias significativas entre las dos suturas en cuanto a los resultados clínicos ni en la facilidad de su uso por parte de los distintos cirujanos. El costo de una sutura de fabricación artesanal es de US $0.07 lo que representa menos de la trigésima parte del costo del hilo comercial, cuya ventaja sigue siendo la garantía de seguridad de la calidad. Se discute si esta garantía de calidad justifica la importante diferencia en el precio y si el hilo de fabricación artesanal debería ser recomendado a los cirujanos en paises donde el coste del material quirúrgico muchas veces constituye un obstáculo para intervenciones de importancia vital.
References
Freudenberg S, Mkony C, Wilhelm T, et al. Medical education: the role of inter-institutional cooperation in surgical training and practice: a German-Tanzanian model. East Afr. Med. J. in press
OE Onwujekwe EN Shu PO Okonkwo (2000) ArticleTitleCommunity financing of local ivermectin distribution in Nigeria: potential payment and cost-recovery outlook Trop. Doct. 30 91–94 Occurrence Handle1:STN:280:DC%2BD3czgtFeksA%3D%3D Occurrence Handle10842555
C Bendinelli T Leal F Moncade et al. (2002) ArticleTitleEndoscopic surgery in Senegal: benefits, costs and limits Surg. Endosc. 16 1488–1492 Occurrence Handle10.1007/s00464-001-9188-1 Occurrence Handle1:STN:280:DC%2BD38nktlWmsw%3D%3D Occurrence Handle11988789
P Bewes (2000) ArticleTitleAbdominal closure Trop. Doct. 30 39–41 Occurrence Handle1:STN:280:DC%2BD3czgtFensQ%3D%3D Occurrence Handle10842526
AM Hodges (2001) ArticleTitleFishing line: a valuable suture material Trop. Doct. 31 98–99 Occurrence Handle1:STN:280:DC%2BD3M3mtVOkuw%3D%3D Occurrence Handle11321285
King M, Bewes P, James C, et al. Basic Methods and Instruments: Primary Surgery, vol. I, Oxford, Oxford Medical Publications, 1990;39–51
AO Longombe A Ralaimiarison KM Lusi (1993) ArticleTitleThe use of fishing nylon for surgery in rural areas in northeast Zaire Trop. Doct. 23 179–180 Occurrence Handle1:STN:280:ByuD1MfmsVM%3D
S Freudenberg S Samel J Sturm et al. (2001) ArticleTitleThe improvised atraumatic suture: a cost-reducing technique, not only for the tropics? Trop. Doct. 31 166–167 Occurrence Handle1:STN:280:DC%2BD3MzovFyjsg%3D%3D Occurrence Handle11444342
JE Hollander AJ Singer S Valentine et al. (1995) ArticleTitleWound registry: development and validation Ann. Emerg. Med. 25 675–685 Occurrence Handle1:STN:280:ByqB2MbptFM%3D Occurrence Handle7741347
A Pietrabissa S Merigliano M Montorsi et al. (1997) ArticleTitleReducing the occupational risk of infections for the surgeon: multicentric national survey on more than 15,000 surgical procedures World J. Surg. 21 573–578 Occurrence Handle10.1007/s002689900275 Occurrence Handle1:STN:280:ByiA2svitVY%3D Occurrence Handle9230652
Acknowledgments.
Many thanks go to the entire staff of the surgical department in Butare, where the study was performed. We also gratefully acknowledge the support of Joachim Brade for the statistical workup as well as the editorial input of Reinhart Freudenberg and Michael Trede. The authors are grateful to the German Academic Exchange Service (DAAD) for supporting financially the cooperation between the surgical departments and making this study possible.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Freudenberg, S., Nyonde, M., Mkony, C. et al. Fishing Line Suture: Cost-saving Alternative for Atraumatic Intracutaneous Skin Closure—Randomized Clinical Trial in Rwanda. World J. Surg. 28, 421–424 (2004). https://doi.org/10.1007/s00268-003-7323-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-003-7323-y