
Abstract
Chemical compositions of atmospheric fine particles like PM2.5 prove harmful to human health, particularly to cardiopulmonary functions. Multifaceted health effects of PM2.5 have raised broader, stronger concerns in recent years, calling for comprehensive environmental health-risk assessments to offer new insights into air-pollution control. However, there have been few studies adopting local air-quality-monitoring datasets or local coefficients related to PM2.5 health-risk assessment. This study aims to assess health effects caused by PM2.5 concentrations and metal toxicity using epidemiological and toxicological methods based on long-term (2007–2017) hourly monitoring datasets of PM2.5 concentrations in four cities of Taiwan. The results indicated that (1) PM2.5 concentrations and hazardous substances varied substantially from region to region, (2) PM2.5 concentrations significantly decreased after 2013, which benefited mainly from two actions against air pollution, i.e., implementing air-pollution-control strategies and raising air-quality standards for certain emission sources, and (3) under the condition of low PM2.5 concentrations, high health risks occurred in eastern Taiwan on account of toxic substances adsorbed on PM2.5 surface. It appears that under the condition of low PM2.5 concentrations, the results of epidemiological and toxicological health-risk assessments may not agree with each other. This raises a warning that air-pollution control needs to consider toxic substances adsorbed in PM2.5 and region-oriented control strategies are desirable. We hope that our findings and the proposed transferable methodology can call on domestic and foreign authorities to review current air-pollution-control policies with an outlook on the toxicity of PM2.5.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Impacts of air pollution imposed on human health are manifest in countries undergoing rapid industrialization and urbanization, whereas little attention is placed on local air-quality-monitoring measures or local coefficients regarding air-pollution-induced health-risk assessment (Bi et al. 2020; Liu et al. 2018). Global premature deaths linked mainly to ambient air-pollution exposure have exceeded seven million people every year (Forouzanfar et al. 2016; Liu et al. 2018; Lim et al. 2012; Wang and Komonpipat 2020). Atmospheric fine particles possess chemical compositions that prove harmful to human health, especially concerning cardiopulmonary diseases (TW EPA 2020). Fine particulate matter (PM2.5) is one of the major air pollutants derived from a complex mixture of chemicals found in both natural and anthropogenic sources. High PM2.5 concentrations can impose negative effects on cancer risks (e.g., IARC 2013; Ritz et al. 2018; Vedal et al. 2013; Wilhelm et al. 2011; Xing et al. 2016; Yang et al. 2018) and increase the risk of premature mortality and adverse respiratory health in children (Chen et al. 2016; Fan et al. 2016; Faraji et al. 2018; Liu et al. 2015; Lu et al. 2015). In addition, transport-related air pollution can stimulate an increase in death risk, particularly relevant to cardiopulmonary diseases (HEI—Health Effects Institute 2010; Park et al. 2008; Yang et al. 2019a, b). Air-quality deterioration is evidently getting worse in many parts of the world (Li et al. 2014; Song et al. 2017; Zhou et al. 2019, 2020). Assessing the impacts of ambient exposure to particulate matters like PM2.5 on human health is essential but challenging, which calls for health-risk assessment methods in consideration of long-term monitoring datasets.
Several studies have assessed the health effects of particulate matter in the past few decades, but there have been few studies focusing on site-specific estimates in different regions of the world and the lessons learned for improved methods and policy. The enduring uncertainty in characterizing the toxicity of particulate matter raises another important concern. A better understanding of chemical components or emission sources that are the most harmful to human health can assist decision-makers not only in developing air pollution regulations but also in exploring the biological mechanisms that detect the health effects of air pollution. Thermal power, biomass burning, and building materials are considered the major sources of PM2.5 emissions (Karambelas et al. 2018). The spatiotemporal variation of PM2.5 emissions has received increasing research attention over the past decade, especially in China and India (e.g., Gorai et al. 2018; Jin et al. 2017; Krishna et al. 2019; Xu et al. 2017; Xue et al. 2018; Yang et al. 2017). For instance, PM2.5 concentrations were found to relate closely with the gross domestic product and population size in China, and a dramatic difference in PM2.5 concentrations has been observed between eastern and western China (Jiang et al. 2018; Li et al. 2019; Yan et al. 2018).
Air-pollution-induced health risks can be assessed by various approaches, including the global burden of disease, epidemiological methods, and toxicological methods (Błaszczyk et al. 2017; Brauer et al. 2012; Forouzanfar et al. 2016; Lelieveld et al. 2015; Li et al. 2017). Epidemiological and toxicological methods are commonly used to describe and quantify the health risk of PM2.5 (Fantke et al. 2015; Sclar and Saikawa 2019; Hime et al. 2018; Jia et al. 2017; Kim et al. 2015a, b). However, the underlying principles as well as advantages and disadvantages of these two methods are very different. Epidemiological methods intend to investigate and track the relationship between PM2.5 concentration and disease occurrence. Findings from epidemiological studies have shown that the relationship of PM2.5 concentrations to adverse health effects is stronger than that of PM2.5 concentrations with total suspended particulates (Hwang et al. 2017; Li et al. 2019). Assessing the latent effects of long-term exposure to particulate matters on health is crucial; nevertheless, epidemiological research requires long-term PM2.5 monitoring datasets, which may be unavailable in most countries. Alternatively, toxicological methods focus on toxic materials and present results by carcinogenic (CRs) and non-CRs (Adami et al. 2011).
The exploration of the cause-and-effect relationship between PM2.5 and human diseases based on region-wide historical datasets is inclined to employ epidemiological and toxicological methods. It takes considerable time and efforts for toxicologists and epidemiologists to identify the linkage between a putative causal agent and a response. Evidence-based analyses utilize many of the same fundamental considerations in the two disciplines. Consistency in evidence for adverse health effects of short-term exposure to PM2.5 sustains countermeasures taken to control PM2.5 emissions (Brauer et al. 2012; Chan and Ng 2011; Wang et al. 2018). For example, Kan et al. (2007) indicated that an increase of 10 μg/m3 in PM2.5 concentration would lead to an increase of 0.95% in the mortality rate of lung diseases in Shanghai. Previous studies in the United States have also pointed out that exposure to PM2.5 would increase lung cancer (McDonnell et al. 2000; Jerrett et al. 2005). Long-term epidemiological studies on PM2.5 in Taiwan have reported the updates on lung and heart functions affected by PM2.5 as well as mortality rate (Wang 2011; Liou 2014; Lo et al. 2016). These studies have also indicated that health effects would vary with pollutant compositions from different sources. Particle components may impose more significant impacts on human health than PM2.5 level, and therefore the compositions of fine particles should be taken into account when assessing health hazards from PM2.5 pollution (Wang 2011; Liou 2014; Lo et al. 2016). This implies that health-risk assessments should involve methods from different perspectives when decision-makers and/or governments intend to revise or review air-pollution-control strategies. However, further investigation is required to explain the heterogeneity raised in health-effect estimates. The incorporation of epidemiological and toxicological disciplines into causal analyses could benefit the studies associating health effects with air pollutants (Pope et al. 2002; Brunekreef and Forsberg 2005; Krzyżanowski et al. 2005; Schlesinger 2007; Gao and Ji 2018; Li et al. 2019).
Both epidemiological and toxicological methods play an important role in health-risk assessment needed for establishing air-pollution-control policies (Karambelas et al. 2018; Li et al. 2018). As known, the spatiotemporal trends and characteristics of PM2.5 concentration may differ in the perspectives of urban type and population size (Aunan et al. 2018). Thus, health-risk assessment on PM25 would deliver much more convincing results if local air-quality-monitoring datasets and coefficients related to PM2.5 health-risk assessment are available. To date, many studies have discussed the relationship between PM2.5 and health risk (e.g., Lu et al. 2017; Pearce et al. 2011; Tai et al. 2010; Wang et al. 2015), whereas few studies have utilized local air-quality-monitoring datasets or coefficients related to PM2.5 health-risk assessment. Besides, urban development and the type of a city (e.g., commercial or industrial) can lead to different air-pollution problems. Multifaceted assessments are required for the formulation of air-quality-control policies. Thus, this study aims to provide recommendations on region-oriented air-quality control/regulation strategies (thresholds) grounded in health-risk assessments, and engaging epidemiological and toxicological methods based on the long-term monitoring datasets (2007–2017) collected in four regions of Taiwan. Our purpose of selecting different types of cities is to explore the distinction in pollution behavior between cities. Our proposed methodology is expected to support the review of current air- pollution-control policies with another outlook on toxic substances adsorbed in PM2.5, such that necessary adjustment in policies can be made, if any policy inadequacy occurs.
Methodology
Materials
Industrial development, economic growth, and urbanization may lead to high PM2.5 concentrations. In Taiwan, transboundary air pollution and poor atmospheric diffusion due to meteorological conditions and mountainous terrains are also considered responsible for high PM2.5 concentrations. PM2.5 concentrations and the hazardous substances adsorbed on PM2.5 surface can vary substantially from region to region. It is imperative to assess the causes of high PM2.5 concentrations and their impacts on human health region by region. The Environmental Protection Administration in Taiwan (Taiwan EPA) has established interactive models for the monitoring and control of environmental air pollution in recent years. A total of 76 air-quality-monitoring stations have been built and operated by the Taiwan EPA. This study was conducted based on hourly monitoring datasets of PM2.5 concentrations collected by the Taiwan EPA during 2007 and 2017.
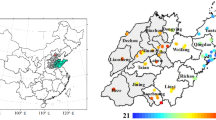
Table 1 shows the parameters used in the toxicological method, which were summarized from various sources. For assessing health risks associated with toxic air pollutants, we selected four air-quality-monitoring stations that provided at least 1 year of monitoring data of heavy metals related to PM2.5 (Fig. 1). The four selected stations are Stations Zhongshan, Chungming, Pingtung, and Dongshan, which represent northern, western, southern, and eastern regions of Taiwan, respectively. Table 2 displays the information of population, vehicles, and industrial facilities of the cities where the four selected stations are located. Station Zhongshan (denoted as A1) is located in Taipei City (northern Taiwan), which is a business city and has the highest densities of population and vehicles. Station Chungming (denoted as A2) is located in the Taichung City (western Taiwan), which has the highest density of industrial facilities. Station Pingtung (denoted as A3) is located in a periurban area that is close to an industrial park in Kaohsiung City (southern Taiwan), which exhibits complex pollution sources related to industrial production and transportation. Station Dongshan (denoted as A4) is located in Yilan County (eastern Taiwan), which has the lowest densities of population and vehicles. The four stations were selected according to geological location and social–economic environment in order to assess their difference, if any, in air pollution (PM2.5 concentrations) with respect to location, city type, and population size. The annual average and the standard deviation of PM2.5 concentrations coupled with population exposed to PM2.5 were used to calculate health risks at a regional scale.

Locations of air-quality-monitoring stations A1–A4 in the study area
Research Framework
This study intends to explore PM2.5 features and perform epidemiological and toxicological health-risk assessments for investigating adverse health effects caused by the inorganic components of PM2.5 in four regions of Taiwan (Fig. 2). First of all, the parameters of the toxicological method were identified based on PM2.5 and toxicological datasets collected in this study. Then, the long-term trends of PM2.5 concentrations monitored at Stations A1–A4 were analyzed. We next used epidemiological and toxicological methods to assess the health risks at Stations A1–A4. The site-specific affecting factors were also explored. In this study, the epidemiological method (excess risk (ER) ratio) was used to identify the population exposed to PM2.5 at each station, while the toxicological method (CR and hazard quotient (HQ)) was used to identify the toxicants adsorbed on PM2.5 surface and their concentrations at each station, where the exposure period and the frequency were also identified. The results of both methods at Stations A1–A4 were evaluated and compared.

Research framework
Epidemiological Method
Epidemiological studies on health effects of PM2.5 have reported that the relative risk (RR) would typically be considered a function of PM2.5 concentrations (Fantke et al. 2015). Epidemiological methods capable of extracting valid information from human exposures to toxic metals are crucial to the establishment of causal relationships between contaminants and specific health endpoints, such as death or disease. This study adopts epidemiological methods to establish the relationship between exposure dose and health risks based on long-term data.
According to the United States Environmental Protection Agency (US EPA 2013, 2014), the quantitative health-risk assessment of particulate matters can be conducted using epidemiological methods in consideration of air-quality information and the concentration-response function (HEI—Health Effects Institute 2010). According to the health-risk assessment of PM2.5, the World Health Organization (WHO) recommended that the concentration-response function of aerosols can be established and expressed in mortality and morbidity based on epidemiological and correlation results (Ross 2009). Several indicators such as RR and ER are commonly used to express quantitative exposure-response relationships between PM2.5 and health risks (Janssen et al. 2013; Lu 2009; Lu et al. 2015). Many studies adopted generalized linear models to carry out epidemiological assessments (Atkinson et al. 2012; Lu et al. 2015; Shah et al. 2013). Therefore, this study assumes that there is a linear relation between exposure and health outcomes (Atkinson et al. 2012). One of our study goals is to compare the health risks of PM2.5 exposure between the exposed and the unexposed group, and therefore ER was chosen for use in this study. Under the condition of limited local epidemiological data, ER can be converted from RR that represents all-cause mortality for all ages (Hwang et al. 2017). RR refers to a standardized increment in pollutant concentration, while ER denotes the attributable fraction among the exposed population of the whole population. RR and ER can be calculated by Eqs. (1) and (2), respectively (Chalvatzaki et al. 2019)
where X is the concentration of PM2.5 (μg/m3), and X0 is the baseline concentration of PM2.5.
RR can be estimated according to Hwang et al. (2017). For an increase of 10 µg/m3 in PM2.5 concentration, RR would be 1.02, with a 95% confidence interval = [1.007–1.040]. The threshold (baseline concentration) of the health effects caused by PM2.5 is the annual standard (15 µg/m3) released by the Taiwan EPA, which means an annual average concentration higher than 15 µg/m3 might cause adverse health effects. According to Eq. (1) and the baseline concentration (X0 = 15 μg/m3) of PM2.5, β (=ln[RR(X)]/(X – X0)) was set (calculated) as 0.0198 (=ln[1.02]/10) in this study.
Toxicological Method
PM2.5 contains a mixture of chemicals, while chemical hazards can be complex, for instance, metals and polycyclic aromatic hydrocarbons. There have been studies focusing on the chemical risks of PM2.5 (e.g., Betha et al. 2013; Hu et al. 2012; Park et al. 2008; Wu et al. 2009; Wu 2013; Zhou et al. 2020). The implementation of the toxicological method adopted in this study consists of four procedures, i.e., hazard identification, dose–response assessment, exposure assessment, and risk characterization (Barnes et al. 1988; Eregno et al. 2016). Hazard identification aims at identifying whether a substance is toxic or not. Once a substance is identified toxic, its carcinogenicity should also be investigated. For the dose–response assessment, the toxicity category of each substance can refer to the toxicity database. The exposure assessment identifies how a receptor exposes to a toxicant. Finally, risk characterization presents health risks by two categories: the CR and the non-CR (evaluated by HQ).
CR and HQ corresponding to heavy metals in PM2.5 through ingestion, dermal contact, and inhalation can be calculated by the following equations:
where EC is the exposure concentration (μg/m3), UR is the inhalation-unit risk ((μg/m3)–1), and RfC is the inhalation-reference concentration (mg/m3).
Residents living in the investigative area are potential receptors of airborne metals. EC shows the characteristics of receptor exposure, as shown below:
where Ci is the concentration of the target substance (μg/m3, i.e., heavy metals in this study), ED is the exposure duration (year), EF is the exposure frequency (day/year), ET is the exposure time (h/day), and AT is the average exposure time (h). It is noted that we refer to the EC parameters set by the Taiwan EPA (guideline for health risk assessment, https://www.epa.gov.tw/cpDownloadCtl.asp?id=6146) and the US EPA (US EPA 1995).
The exposure and the dose–response assessment are carried out in parallel. The exposure concentration of the receptor is calculated, simulated, or measured in the field to estimate the exposure amount (e.g., ED, ET, and EF) of the toxic substance in the environment. According to the residency preference disclosed in Taiwan (Ministry of Health and Welfare (MOHW) 2008), ED, EF, ET, and AT adopted in this study were set to 35 years, 365 days, 24 h/day, and 613,200 h/year, respectively. Therefore, Eq. (5) can be expressed as EC = \(\frac{{{\mathrm{Ci}} \times 35 \times 365 \times 24}}{{6135,200}}\).
According to the classification of carcinogenic elements defined by the International Agency for Research on Cancer of the WHO, arsenic, inorganic arsenic compounds, nickel compounds, cadmium, and cadmium compounds belong to Class I, lead compounds (inorganic) belong to Class 2A, and cobalt and cobalt compounds belong to Class 2B (IARC 2013). Nevertheless, copper, zinc, and manganese do not appear on the aforementioned classification list. Therefore, the CRs corresponding to copper, zinc, and manganese were not investigated in this study. Besides, the UR values for arsenic (inorganic), cadmium, cobalt, chromium (VI), nickel, and lead were disclosed in the regional screening levels (RSL) released by the US Environmental Protection Agency (Health effects assessment summary tables (HEAS), https://cfpub.epa.gov/ncea/risk/recordisplay.cfm?deid=2877).
CR represents the probability of a person undergoing cancer development involving lifetime exposure to carcinogenic hazards. The tolerable risk of CR for regulatory purpose falls within 【1 × 10−6, 1 × 10−4】(Wei et al. 2015). Besides, the overall potential of noncarcinogenic effects imposed by more than one chemical component can be assessed by the overall HQ that sums up all the HQs of a suite of chemical components. A HQ smaller than 1 indicates no adverse health effects being expected, while a HQ higher than 1 indicates a possible occurrence of adverse health effects. Table 1 shows the parameters used in the toxicological method of this study.
Results and Discussion
The trends of annual average concentrations of PM2.5 at Stations A1–A4 were presented at first. Then, the health-risk results obtained from epidemiological and toxicological methods were analyzed and discussed. Finally, new thresholds (acceptable upper limits of PM2.5 concentration) and strategies for air-quality control were recommended at a regional scale.
Preliminary Analysis on PM2.5 at Stations A1–A4 (2007–2017)
According to the monitoring data of hourly PM2.5 concentrations collected at Stations A1–A4 during 2007 and 2017, the minimum value was zero but the maximum value varied from station to station, from year to year. Governments and residents in Taiwan have raised serious concerns about air- quality deterioration, and therefore a number of air-pollution-control policies have been executed in recent years (TW EPA 2011, 2012, 2013). As a result, the annual average PM2.5 concentrations showed a decreasing trend during 2007 and 2017, especially in western and northern Taiwan (Fig. 3). We noticed that PM2.5 concentrations at all the four stations significantly decreased after 2013. Such mitigation has benefited from two main actions taken by the Taiwan EPA against air pollution since 2013, i.e., implementing air-pollution-control strategies (e.g., lowering the upper limit of the acceptable concentrations of PM2.5) and raising air-quality standards (i.e., reducing thresholds) for certain emission sources like industrial factories and power plants (TW EPA 2020). Besides, the Taiwan EPA has also developed strategies to reduce emissions from mobile pollution sources. For instance, the Air-quality Standards for Fine Suspended Particulates (PM2.5) (TW EPA 2012, 2013), the Stationary Pollution Source Air Pollutant Emissions Standards (https://oaout.epa.gov.tw/laW/EngLawContent.aspx?lan=E&id=81), and the Vehicular Air Pollutant Emission Standards (https://oaout.epa.gov.tw/laW/EngLawContent.aspx?lan=E&id=158). More policy information can be found on the website of the Air-Quality Protection Policy Planning (https://air.epa.gov.tw/EnvTopics/AirQuality_1.aspx) and the website of the Laws and Regulation Database of R.O.C. (https://law.moj.gov.tw/LawClass/LawHistory.aspx?pcode=O0020007). Because several industrial parks and a thermal power plant are located in the western region (highly urbanized), Stations A2 and A3 had higher maximal and average concentrations of PM2.5 than Stations A1 and A4. We noticed that the annual average concentrations of PM2.5 at Stations A1, A2, and A3 were higher than the annual standard (15 μg/m3) before 2013, but were significantly reduced after 2013.

PM2.5 concentration versus excess risk (ER) ratio at monitoring stations A1–A4 during 2007 and 2017
The surrounding area of Station A1 is the most urbanized area in Taiwan, but it is less industrialized than those of Stations A2 and A3. Thus, PM2.5 concentrations of Station A1 would be significantly affected by moving vehicles or transportation, whereas PM2.5 concentrations of Station A3 would be affected mostly by industrial development because Station A3 is located in a periurban area next to an industrial park. Although new techniques have been developed to reduce PM2.5 air pollution, PM2.5 would still be affected by meteorological conditions such as wind direction and speed. On the other hand, reducing PM2.5 emissions from industrial sectors may require changes in fuel generation from coal to other sources sustaining cleaner production, or requires more air-pollution control equipment, which would lead to increases in construction, operation, and maintenance costs. Besides, the establishment and development of new industrial parks may also be restricted. However, it is inevitable that the implementation of the aforementioned policy measures may become a barrier to industrial production and economic development. As for Station A4, its annual average PM2.5 concentrations appeared to be the lowest (Fig. 3). It is noted that Station A4 (eastern Taiwan) is located in a lowly industrialized and urbanized area and tourism is the main source of income for eastern Taiwan. Thus, the concentrations of PM2.5 and other air-pollution sources were lower at Station A4 than at Stations A1–A3.
Health-Risk Assessment Using the Epidemiological Method
In this study, the ER ratio was calculated based on the annual average concentration of PM2.5. Figure 3 illustrates the trends and ranges of ER ratios obtained from the epidemiological method at a yearly scale for Stations A1–A4 (2007–2017). We noticed that all the ER ratios of the four stations were very low (<1%, with a 95% confidence interval of【0, 2.4878】) and the ER ratio decreased (<0.6% after 2013) as PM2.5 concentrations decreased over time. Station A3 (southern Taiwan) had the highest ER ratio (about 0.7% in 2007) than the other three stations in each year because it had the highest annual average PM2.5 concentrations among the four stations. The ER ratios at Station A1 (in Taipei City) significantly reduced to <0.4% after 2013. The ER ratios at Station A4 (eastern Taiwan) were near zero after 2016 because the annual average PM2.5 concentrations of this station were lower than the annual standard released by the Taiwan EPA, which meant that almost no health effect was imposed on human beings.
Health-Risk Assessment Using the Toxicological Method
To investigate the current health hazards and identify the hotspot(s) of high health risks related to PM2.5 in Taiwan, a comprehensive assessment is needed, especially when health-risk data are unavailable in many regions. The toxic metals in PM2.5 were also investigated. Table 3 presents the concentration range of each toxic metal in PM2.5 at Stations A1–A4, referring to several reports about toxic metals in PM2.5 (Huang 2001, 2005; Tseng 2006; Wang 2000; Weng 2014). These toxic metals have been detected nearby Stations A1–A4 for more than 1 year. Among the four stations, Station A2 contained the largest variety of metals and had the highest concentration in each metallic category, except for Ni. The concentration of Ni was the highest at Station A4. The average of concentration of each metallic category was higher at Station A3 than at Station A1. The concentration in each metallic category was mostly the lowest at Station A4, except for Ni.
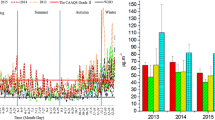
Figure 4 illustrates the maximum and annual average CR values obtained from the toxicological method based on PM2.5 concentrations and the relevant toxic metal contents. The calculation of CR values was based on PM2.5 concentrations and heavy-metal contents. To be more precise, the CR was calculated for hourly frequency and then it was averaged to get the annual average values for each station. The maximum CR value was the maximum of hourly CR values in each year. On account of the large gaps between the two groups, the maximum and average CR values were plotted separately (Fig. 4), which were, in general, unacceptable in regard to health effects. This pointed out that high carcinogenic health risks occurred at the four stations in each year. More precisely, the maximal CR value was high even though the annual average CR value was low in each year, implying that such high risk might not last for a long time, but could cause serious adverse health effects on certain occasions. Thus, these occasions should be unveiled for further investigation. For instance, the reason why Station A2 had the highest maximal and annual average CR values in each year was due to its largest variety of toxic metals, despite its less high annual average concentrations of PM2.5 (Fig. 2 and Table 3). Although the annual average CR values at Station A2 decreased from 2.33 × 10–3 (2007) to 1.31 × 10–3 (2017), these values were still much higher than the tolerable upper limit (1 × 10–4) of CR. In contrast, Station A3 had the highest annual average PM2.5 concentration but a less high annual average CR value in each year. Station A4 had the lowest annual average concentration of PM2.5, but its CR values were not the lowest. The results indicated that Station A4 had low annual average concentrations of PM2.5 but high toxicological health risks, which deserved to be explored in depth, as shown below.

Results of health-risk assessment on carcinogenic risks (CR) and hazard quotient (HQ) at monitoring stations A1–A4
The results of non-CRs based on the HQ are shown in Fig. 4. Overall, the average HQ values were unacceptable at all stations, except for Station A1 (HQ value < 1). The HQ results also indicated that health risks were high at Stations A2–A3, but the HQ values did decrease at all stations in recent years. Figure 4 presents both the annual average and the maximum of HQ values in each year. Station A3 had the highest annual concentrations of PM2.5, but its maximum HQ value was not the highest in each year, implying that PM2.5 emitted around this station did not contain many toxic metals. In contrast, Station A4 had the lowest annual average concentration of PM2.5, but its HQ value was relatively high in each year, implying that the concentrations of toxic substances (e.g., Mn, Ni, and Pb) adsorbed on PM2.5 surface were high at this station (Table 3). According to TW EPA (2013), cement plants can cause an increase in PM2.5 concentrations and such emissions are accompanied with heavy metals (adsorbed in PM2.5) because cement plants have complex fuel sources (including wastes). Station A4 had the lowest annual average concentrations of PM2.5 but high HQ values, which suggested that the amounts of heavy metals would be the key driver affecting the health risks at this station.
According to the CR and HQ results, the health-risk assessment should consider not only PM2.5 concentrations but also the concentrations of toxic substances associated with PM2.5.
Comparison between the Epidemiological and Toxicological Methods
The geographical locations and land uses of Stations A1–A4 are different (A1, north_urban; A2, west_urban near an industrial park; A3, south_peri-urban and near an industrial park; A4, east_peri-urban). Thus, emission sources and health risks should be investigated at a regional scale. It was noted that the health risks obtained from epidemiological and toxicological methods showed decreasing trends from 2007 to 2017 (Figs. 3 and 4). Although there is no tolerable upper limit recommended by authorities for the ER ratio, a lower ER ratio would be favorable. But the health risks obtained from the toxicological method in the four regions were not acceptable (Fig. 4). Thus, the health impact of toxic metals on human beings should be explored further.
We noticed that the results of epidemiological and toxicological methods were not consistent. For instance, the highest epidemiological health risk occurred in the southern region (Station A3, Fig. 3), whereas the highest toxicological health risk occurred in the western region (Station A2, Fig. 5). Taking geographical location into consideration, CR and HQ values were the highest in western Taiwan but the lowest in northern Taiwan in 2007, 2012, and 2017 (Fig. 5). Station A2 did not have the highest annual average concentration of PM2.5 even though it is located within an urban area with industrial development. However, high health risks (CR and HQ) were found in the surrounding area of Station A2 because there were complex air-pollution sources near this station. Due to the limitation of the epidemiological method, the health risk was described only by PM2.5 concentrations. In contrast, the toxicological method described health risks through heavy-metal components adsorbed on PM2.5 surface. According to the results obtained from both methods, low annual average concentrations of PM2.5 did not necessarily result in low health risks. This phenomenon could be observed in eastern Taiwan (Station A4). The results pointed out that a station (such as Station A4) with low annual average concentrations of PM2.5 might have high contents of toxic heavy metals in PM2.5, leading to high health risks. However, when making countermeasures against PM2.5 pollution, a station with low PM2.5 concentrations would be easily ignored even though it actually had high toxicological health risks. According to these findings, the pollution-control strategy of PM2.5 should also be implemented at areas (e.g., the eastern region in Taiwan) with low PM2.5 concentrations but high health risks.

Comparison results of health-risk assessments with respect to a carcinogenic risks (CR) and b hazard quotient (HQ) at monitoring stations A1–A4 in 2007, 2012, and 2017
We further explored the emission sources of the heavy-metal components of PM2.5 in the eastern region. It was speculated that industrial and transportation emissions would constitute PM2.5 emission sources. Station A4 is located in a periurban area with the lowest densities of population and vehicles, and therefore is expected to have the lowest PM2.5 concentration and health risks. However, the health risk obtained from the toxicological method was high at Station A4. The reason might be that several cement plants are located near Station A4 such that many kinds of heavy metals constitute emission particles, despite the low density of industrial facilities in this region. In order to better understand the high concentrations of heavy metals at Station A4, we refer to several research reports released by the local environmental protection agency in recent years. These reports indicate that the cement industry and traffic loads caused by tourism and human activities are the main emission sources of PM2.5 in this area (Yilan County Environmental Protection Bureau (Yilan County EPB) 2014, 2015, 2017a, b, 2019a, b).
We next investigated Station A1, which is located in a business city with the highest densities of vehicles and population. Air pollution is expected to come mainly from transportation in this city. Table 3 supports this claim, i.e., emissions of heavy metals such as Pb and V in this city come from transportation (HEI—Health Effects Institute 2010). However, the health risks obtained from both methods at this station were not the highest. On the other hand, Station A2 had the highest density of industrial facilities. Thus, the results of health-risk assessment showed that the city embracing Station A2 had the highest CR values (Fig. 5). Station A3 is located in a periurban area near an industrial park. This could be the reason why high annual average concentrations of PM2.5 occurred here. However, the toxicological health risk at Station A3 was not the highest because fewer heavy metals were contained in PM2.5 here (Table 3 and Figs. 4, 5). Nevertheless, its epidemiological health risk was the highest (Fig. 3). These results showed again that the epidemiological and toxicological health risks were not consistent.
It is worth mentioning that Taiwanese terrains bring certain influence on air pollution. Mountainous terrains and wind directions may trap air pollutants in some areas. In Taiwan, mountains with elevations reaching 4000-m run mainly from north to south, while the wind usually blows from west to east, and therefore air pollutants would usually be blocked in the regions surrounding Stations A1 and A2. This phenomenon is especially obvious in winter. It is also noted that the whole western Taiwan can be affected by long-range transboundary air pollution, especially smog from China, in winter. For these reasons, PM2.5 pollution in Taiwan is more serious in winter.
Following the above results, the thresholds for issuing air-pollution warnings should be adjusted for areas with low PM2.5 concentrations but high toxicological health risks, despite the threshold of 15 μg/m3 released by the Taiwan EPA. This study intends to recommend the acceptable upper limits of PM2.5 concentration for the four regions surrounding Stations A1–A4 in consideration of both the toxicological health-risk assessment (CR and HQ) and the statistical analysis based on hourly PM2.5 concentrations. The results are shown in Fig. 6. Taking year 2017 as an example and referring to the Risk Characterization Handbook of US EPA (2001) and TW EPA (2001), the tolerable upper limits of CR and HQ are 1 × 10–4 and 1, respectively, which could be utilized to calculate the acceptable upper limit of PM2.5 concentration recommended for each station in this study. For example, referring to Eqs. (3) and (4), the recommended acceptable upper limit of PM2.5 concentration corresponding to CR (=1 × 10–4) at Station A1 can be calculated by 1 × 10−4/(The percentage of toxic heavy metal in PM2.5) × EC × UR. The results indicated that there were 50%, 37%, 31%, and 71% of hourly PM2.5 data lower than the annual standard (15 μg/m3) at Stations A1–A4, respectively. The acceptable upper limits of PM2.5 concentration derived from CR at Stations A1–A4 were 23 μg/m3, 0.1 μg/m3, 16.7 μg/m3, and 7.4 μg/m3, respectively, subject to the tolerable upper limit (i.e., 1 × 10–4) of CR (US EPA 2001). The acceptable upper limits of PM2.5 concentration derived from HQ at Stations A1–A4 were 10.4 μg/m3, 3.2 μg/m3, 23.9 μg/m3, and 4.3 μg/m3, respectively, subject to the tolerable upper limit (i.e., 1) of HQ (US EPA 2001). Comparing these derived acceptable upper limits of PM2.5 concentration, the current annual standard (15 μg/m3) seems less strict about health protection against air-quality deterioration. It is advised that the acceptable upper limit of PM2.5 concentration should be redefined region by region. For instance, the acceptable upper limit for Station A1 was 23.0 μg/m3 subject to the tolerable upper limit of CR while being 10.4 μg/m3 subject to the tolerable upper limit of HQ. Therefore, 10.4 μg/m3 would be the recommended annual standard for PM2.5 concentration in this region. For Station A2, the recommended annual standard for PM2.5 concentration would be 0.1 μg/m3 because the acceptable upper limits of PM2.5 concentrations were 0.1 μg/m3 (by CR) and 3.2 μg/m3 (by HQ). Even though it is unlikely to reduce PM2.5 concentrations to 0.1 μg/m3 in the circumstances, the result does highlight the high toxicity of PM2.5 at Station A2, which deserves cautious air-pollution control and/or strategy. Therefore, the most important problems to tackle at Station A2 are to reduce PM2.5 concentrations and the toxic emission amount by targeting the main emission sources (e.g., industrial production) of PM2.5 toxicity. In other words, it is very important to consider PM2.5 concentrations and the heavy metals in PM2.5 at the same time. The recommended annual standard for PM2.5 concentration at Station A3 would be 16.7 μg/m3 because the acceptable upper limits of PM2.5 concentration were 16.7 μg/m3 (by CR) and 23.9 μg/m3 (by HQ). For Station A4, the recommended annual standard for PM2.5 concentration would be 4.3 ug/m3 because the acceptable upper limits of PM2.5 concentration were 7.4 μg/m3 (by CR) and 4.3 μg/m3 (by HQ). It is noted that the recommended annual standards for PM2.5 concentration in regions surrounding Stations A1, A2, and A4 are stricter (lower than 15 μg/m3). These results suggest that the annual standard for PM2.5 concentration should be refined at a regional scale because the number and the types of heavy-metal components in PM2.5 could vary from region to region.

Tolerable upper limits of PM2.5 concentration derived from CR and HQ for the four regions surrounding Stations A1–A4 (2017)
Site-specific PM2.5 Emission Sources for Air-Pollution Control
According to the above results, the pollution-control strategy of PM2.5 should be site-specific in response to the regional recommendation for the annual standard for PM2.5 concentration. Making PM2.5 pollution-control strategies in many perspectives would be effectual, especially for hotspots. Heavy metals can serve as indicators of PM2.5 emission sources such that toxicological health-risk assessment coupled with social factors like business and transportation types would help identify PM2.5 emission sources.
In sum, according to the handbook (TW EPA 2020) released by the Taiwan EPA, the prevention and control strategies implemented in the recent decade contain the actions taken against stationary pollution sources (e.g., regulation of total emissions, total mass-based control, and emission control of a single manufacturer) and mobile pollution sources (nonstationary pollution sources). Effective mitigation of air pollution can be observed from long-term monitoring datasets, which reveals that such mitigation is indebted to a suite of strategies, rather than a single strategy. It is noted that the actions aiming to reduce the total amount of PM2.5 concentrations were implemented at first, which indeed led to a continual reduction in PM2.5 emissions in the study area and thus helped reduce health risks (Fig. 3). It is also observed that the control strategies have continued driving PM2.5 concentrations to approach the annual standard (15 μg/m3) released by the Taiwan EPA. However, the hypothesis that low PM2.5 concentrations are harmless to human health still remains in question. Therefore, we next seek to explore, in contrast to traditional views, other possibilities (factors) that affect PM2.5 in order to reinforce the protection of human health. In addition to epidemiological health-risk assessment, this study assessed health risks in view of toxicological substances associated with PM2.5 and obtained new findings. There were cases under the condition of low PM2.5 concentrations that the epidemiological method disclosed low health risks, whereas the toxicological method disclosed high health risks (Figs. 3 and 4). This raises a warning that air-pollution control needs to consider toxic substances adsorbed in PM2.5 and region-oriented control strategies are desirable. We hope that our findings and transferable methodology can call on domestic and foreign authorities to review current air-pollution-control policies with an outlook on the toxicity of PM2.5.
Conclusion
PM2.5 is one of the most serious air pollutants that bring detrimental health risks to residents. While PM2.5 control policies and regulations are usually characterized by lacking a review of their effectiveness and impacts on health and environment, it is advised that the review should take PM2.5-related health risks into consideration and then adjust, if necessary, control strategies into region-oriented ones based on the feedback from the review. In particular, the control strategy should consider different features of PM2.5 emissions and metal toxicity compositions at four stations. For instance, the control strategy for Station A3 needs to consider industrial development. This study used epidemiological and toxicological methods to explore health risks induced from PM2.5 based on long-term datasets of air pollution, heavy metals, and toxic substances at four air-quality-monitoring stations (Stations A1–A4) that represent four separate regions covering the whole Taiwan. The results showed that under low PM2.5 concentrations (e.g., Station A4), the epidemiological method did not disclose a high health risk, whereas the toxicological method did disclose a high health risk. That is to say, toxic substances may reside in PM2.5 and cause high health risks under the condition of low PM2.5 concentrations. Such findings would lead to distinct policy recommendations on air-pollution control for different regions. In other words, the toxicity in PM2.5 should be regarded as an assessment indicator for air-pollution control. Besides, the acceptable upper limits of PM2.5 concentration derived from the tolerable upper limit of HQ at Stations A1–A4 were 10.4 μg/m3, 3.2 μg/m3, 23.9 μg/m3, and 4.3 μg/m3, respectively, which indicate that the current annual standard (15 μg/m3) is less strict about health protection against air-quality deterioration. It is suggested that the annual standard for PM2.5 concentration should be redefined on a regional scale because the heavy-metal components in PM2.5 dangerously affect human health and vary from region to region. Governments and decision-makers are advised to take both epidemiological and toxicological health-risk assessments into consideration when planning to modify and/or formulate air-pollution-control policies.
Future researches should pay more attention to the diverse range of health-risk factors from epidemiological and toxicological studies, as well as an increase in the sampling frequency of heavy metals in PM2.5. Besides, researchers are advised to consider both the emission amount and substances associated with PM2.5. For instance, the industrial emissions of heavy metals are considered an important PM2.5 emission source in Taiwan and, even under the condition of low PM2.5 concentrations, may bring significant amounts of toxic substances in PM2.5, which endanger human health (referring to the cases of Stations A2 and A4). More extensive and comprehensive researches on PM2.5 can be carried out if data of more air-quality-monitoring stations and the relevant toxic substances can be available.
Data Availability
The datasets generated in this study are available from the corresponding author on reasonable request.
References
Adami HO, Berry SCL, Breckenridge CB, Smith LL, Swenberg JA, Trichopoulos D, Pastoor TP (2011) Toxicology and epidemiology: improving the science with a framework for combining toxicological and epidemiological evidence to establish causal inference. J Toxicol Sci 122(2):223–234
Atkinson RW, Cohen A, Mehta S, Anderson HR (2012) Systematic review and meta-analysis of epidemiological time-series studies on outdoor air pollution and health in Asia. Air Qual Atmos Health 5(4):383–391
ATSDR, Agency for toxic substances and disease registry. US Public Health Service, USA. https://www.atsdr.cdc.gov/
Aunan K, Ma Q, Lund MT, Wang S (2018) Population-weighted exposure to PM2. 5 pollution in China: an integrated approach. Environ Int 120:111–120
Barnes DG, Dourson M, Preuss P, Bellin J, Derosa C, Engler R, Ghali G (1988) Reference dose (RfD): description and use in health risk assessments. Regul Toxicol Pharmacol 8(4):471–486
Betha R, Pradani M, Lestari P, Joshi UM, Reid JS, Balasubramanian R (2013) Chemical speciation of trace metals emitted from Indonesian peat fires for health risk assessment. Atmos Res 122:571–578
Bi C, Chen Y, Zhao Z, Li Q, Zhou Q, Ye Z, Ge X (2020) Characteristics, sources and health risks of toxic species (PCDD/Fs, PAHs and heavy metals) in PM2. 5 during fall and winter in an industrial area. Chemosphere 238:124620
Błaszczyk E, Rogula-Kozłowska W, Klejnowski K, Kubiesa P, Fulara I, Mielżyńska-Švach D (2017) Indoor air quality in urban and rural kindergartens: short-term studies in Silesia, Poland. Air Qual Atmos Health 10(10):1207–1220
Brauer M, Amann M, Burnett RT, Cohen A, Dentener F, Ezzati M, Van Donkelaar A (2012) Exposure assessment for estimation of the global burden of disease attributable to outdoor air pollution. Environ Sci Technol 46(2):652–660
Brunekreef B, Forsberg B (2005) Epidemiological evidence of effects of coarse airborne particles on health. Eur Respir J 26(2):309–318
CalEPA—California Environmental Protection Agency, USA. https://oehha.ca.gov/
Chalvatzaki E, Chatoutsidou SE, Lehtomäki H, Almeida SM, Eleftheriadis K, Hänninen O, Lazaridis M (2019) Characterization of human health risks from particulate air pollution in selected European. Cities Atmos 10(2):96
Chan CC, Ng HC (2011) A case-crossover analysis of Asian dust storms and mortality in the downwind areas using 14-year data in Taipei. Sci Total Environ 410:47–52
Chen R, Hu B, Liu Y, Xu J, Yang G, Xu D, Chen C (2016) Beyond PM2. 5: the role of ultrafine particles on adverse health effects of air pollution. Biochim Biophys Acta 1860(12):2844–2855
Environmental Protection Bureau of Yilan County Government (2015) Yilan County fine suspended particulate air quality test and cause analysis project. http://ws.e-land.gov.tw/Download.ashx?u=LzAwMS8yMDE1eWlsYW4vMjUzL1JlbEZpbGUvOTYwMy8xMDczMzQvMjAxNTExMTYwNDM4NTAucGRm&n=MTA05bm05bqm6Ieq6KGM56CU56m26KiI55WrLVYyLnBkZg%3D%3D&icon=..pdf
Eregno FE, Tryland I, Tjomsland T, Myrmel M, Robertson L, Heistad A (2016) Quantitative microbial risk assessment combined with hydrodynamic modelling to estimate the public health risk associated with bathing after rainfall events. Sci Total Environ 548:270–279
Fan J, Li S, Fan C, Bai Z, Yang K (2016) The impact of PM2.5 on asthma emergency department visits: a systematic review and meta-analysis. Environ Sci Pollut Res Int 23(1):843–850
Fantke P, Jolliet O, Evans JS, Apte JS, Cohen AJ, Hänninen OO, Loh MM (2015) Health effects of fine particulate matter in life cycle impact assessment: findings from the Basel Guidance Workshop. Int J LIfe Cycle Assess 20(2):276–288
Faraji M, Pourpak Z, Naddafi K, Nodehi RN, Nicknam MH, Shamsipour M, Mesdaghinia A (2018) Effects of airborne particulate matter (PM10) from dust storm and thermal inversion on global DNA methylation in human peripheral blood mononuclear cells (PBMCs) in vitro. Atmos Environ 195:170–178
Forouzanfar MH, Afshin A, Alexander LT, Anderson HR, Bhutta ZA, Biryukov S, Cohen AJ (2016) Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388(10053):1659–1724
Gao Y, Ji H (2018) Microscopic morphology and seasonal variation of health effect arising from heavy metals in PM2. 5 and PM10: one-year measurement in a densely populated area of urban Beijing. Atmos Res 212:213–226
Gorai AK, Tchounwou PB, Biswal SS, Tuluri F (2018) Spatio-temporal variation of particulate matter (PM2.5) concentrations and its health impacts in a Mega city, Delhi in India. Environ Health Insights 12:1178630218792861
HEI—Health Effects Institute (2010) Traffic-related air pollution: a critical review of the literature on emissions, exposure, and health effects (No. 17). Health Effects Institute. Panel on the health effects of traffic-related air pollution
Hime NJ, Marks GB, Cowie CT (2018) A comparison of the health effects of ambient particulate matter air pollution from five emission sources. Int J Environ Res Public Health 15(6):1206
Hu X, Zhang Y, Ding Z, Wang T, Lian H, Sun Y, Wu J (2012) Bioaccessibility and health risk of arsenic and heavy metals (Cd, Co, Cr, Cu, Ni, Pb, Zn and Mn) in TSP and PM2. 5 in Nanjing, China. Atmos Environ 57:146–PM152
Huang JY (2001) Analysis of composition of TSP, PM10 and PM2.5 particles in fixed source flue emissions. Master thesis. https://hdl.handle.net/11296/a58p79
Huang YL (2005) Establishing an exposure factor database for air pollution exposure and risk assessment studies. The National Science Committee of the Executive Yuan, Special Research Project, NSC
Hwang SL, Lin YC, Guo SE, Chou CT, Lin CM, Chi MC (2017) Fine particulate matter on hospital admissions for acute exacerbation of chronic obstructive pulmonary disease in southwestern Taiwan during 2006–2012. Int J Environ Health Res 27(2):95–105
IARC (2013) Outdoor air pollution a leading environmental cause of cancer deaths. World Health Organization, International Agency for Research on Cancer, Lyon, France
IRIS—Integrated Risk Information System. US Environmental Protection Agency. https://iris.epa.gov/AtoZ/?list_type=alpha
Janssen NAH, Fischer P, Marra M, Ameling C, Cassee FR (2013) Short-term effects of PM2. 5, PM10 and PM2. 5–10 on daily mortality in the Netherlands. Sci Total Environ 463:20–26
Jerrett M, Burnett RT et al. (2005) “Spatial analysis of air pollution and mortality in Los Angeles”. Epidemiology 16(6):727–736
Jia YY, Wang Q, Liu T (2017) Toxicity research of PM2. 5 compositions in vitro. Int J Environ Res Public Health 14(3):232
Jiang P, Yang J, Huang C, Liu H (2018) The contribution of socioeconomic factors to PM2. 5 pollution in urban China. Environ Pollut 233:977–985
Jin Q, Fang X, Wen B, Shan A (2017) Spatio-temporal variations of PM2.5 emission in China from 2005 to 2014. Chemosphere 183:429–436
Kan H, London SJ et al. (2007) “Differentiating the effects of fine and coarse particles on daily mortality in Shanghai, China”. Environ Int 33(3):376–384
Karambelas A, Holloway T, Kinney PL, Fiore AM, DeFries R, Kiesewetter G, Heyes C (2018) Urban versus rural health impacts attributable to PM2.5 and O3 in northern India. Environ Res Lett 13(6):064010
Kim KH, Kabir E, Kabir S (2015a) A review on the human health impact of airborne particulate matter. Environ Int 74:136–143
Kim SY, Sheppard L, Larson TV, Kaufman JD, Vedal S (2015b) Combining PM2.5 component data from multiple sources: data consistency and characteristics relevant to epidemiological analyses of predicted long-term exposures. Environ Health Perspect 123(7):651–658
Krishna RK, Ghude SD, Kumar R, Beig G, Kulkarni R, Nivdange S, Chate D (2019) Surface PM2. 5 estimate using satellite-derived aerosol optical depth over India. Aerosol Air Qual Res 19(1):25–37
Krzyżanowski M, Kuna-Dibbert B, Schneider J (eds) (2005) Health effects of transport-related air pollution. WHO Regional Office, Europe
Lee CT (2018) The 2018 project of chemical speciation monitoring and analysis of fine particulate matter (PM2.5). The National Science Committee of the Executive Yuan, Special Research Project, NSC
Lelieveld J, Evans JS, Fnais M, Giannadaki D, Pozzer A (2015) The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525(7569):367
Li PH, Yu J, Bi CL, Yue JJ, Li QQ, Wang L, Liu J, Xiao Z, Guo L, Huang BJ(2019) Health risk assessment for highway toll station workers exposed to PM2.5-bound heavy metals. Atmos Pollut Res 10(4):1024–1030
Li T, Zhang Y, Wang J, Xu D, Yin Z, Chen H, Kinney PL (2018) All-cause mortality risk associated with long-term exposure to ambient PM2.5 in China: a cohort study. Lancet Public Health 3(10):e470–e477
Li Z, Ma Z, van der Kuijp TJ, Yuan Z, Huang L (2014) A review of soil heavy metal pollution from mines in China: pollution and health risk assessment. Sci Total Environ 468–469:843–853. https://doi.org/10.1016/j.scitotenv.2013.08.090
Li Z, Wen Q, Zhang R (2017) Sources, health effects and control strategies of indoor fine particulate matter (PM2.5): a review. Sci Total Environ 586:610–622
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, Aryee M (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859):2224–2260
Liou SH (2014) Epidemiological investigation of fine suspended particles (PM2.5). Environmental Protection Agency Report. NSC102-EPA-F-003-001. https://www.epa.gov.tw/DisplayFile.aspx?FileID=4D80E83B65D18EDC&P=b6f9cd19-3224-44bd-ab1e-854bc5519cbb
Liu J, Chen Y, Chao S, Cao H, Zhang A, Yang Y (2018) Emission control priority of PM2. 5-bound heavy metals in different seasons: A comprehensive analysis from health risk perspective. Sci Total Environ 644:20–30
Liu X, Zhai Y, Zhu Y, Liu Y, Chen H, Li P, Zeng G (2015) Mass concentration and health risk assessment of heavy metals in size-segregated airborne particulate matter in Changsha. Sci Total Environ 517:215–221
Liu Y, Wu J, Yu D, Hao R (2018) Understanding the patterns and drivers of air pollution on multiple time scales: the case of northern China. Environ Manag 61(6):1048–1061
Lo WC, Shue RH, Chan CC, Lin HH (2016) The attributable mortality burden due to PM2.5 exposure in Taiwan. Formos J Med, 20(4):396–405
Lu YH (2009) Simulation and analysis of the particle and heavy metal pollution in atmosphere. Master thesis. https://hdl.handle.net/11296/ev9468
Lu F, Xu D, Cheng Y, Dong S, Guo C, Jiang X, Zheng X (2015) Systematic review and meta-analysis of the adverse health effects of ambient PM2. 5 and PM10 pollution in the Chinese population. Environ Res 136:196–204
Lu X, Lin C, Li Y, Yao T, Fung JC, Lau AK (2017) Assessment of health burden caused by particulate matter in southern China using high-resolution satellite observation. Environ Int 98:160–170
McDonnell WF, Nishino-Ishikawa N et al. (2000) “Relationships of mortality with the fineand coarse fractions of long-term ambient PM10 concentrations in nonsmokers”. J Expo Anal Environ Epidemiol 10(5):427–436
Ministry of Health and Welfare (MOHW) (2008) Compilation of exposure factors. http://tci.ncl.edu.tw/cgi-bin/gs32/gsweb.cgi?o=dnclret&s=id=%22RF10001254340%22.&searchmode=basic&tcihsspage=tcisearch_opt2_search
Park EJ, Kim DS, Park K (2008) Monitoring of ambient particles and heavy metals in a residential area of Seoul, Korea. Environ Monit Assess 137(1-3):441–449
Pearce JL, Beringer J, Nicholls N, Hyndman RJ, Tapper NJ (2011) Quantifying the influence of local meteorology on air quality using generalized additive models. Atmos Environ 45(6):1328–1336
Pope III CA, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K, Thurston GD (2002) Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 287(9):1132–1141
Ritz B, Liew Z, Yan Q, Cui X, Virk J, Ketzel M, Raaschou-Nielsen O (2018) Air pollution and autism in Denmark. Environ Epidemiol 2(4):e028. https://doi.org/10.1097/EE9.0000000000000028
Ross MA (2009) Integrated science assessment for particulate matter. US Environmental Protection Agency, Washington DC, USA, p 61–161
Schlesinger RB (2007) The health impact of common inorganic components of fine particulate matter (PM2.5) in ambient air: a critical review. Inhal Toxicol 19(10):811–832
Sclar S, Saikawa E (2019) Household air pollution in a changing tibet: a mixed methods ethnography and indoor air quality measurements. Environ Manag 64(3):353–365
Shah AS, Langrish JP, Nair H, Mcallister DA, Hunter AL, Donaldson K et al. (2013) Global association of air pollution and heart failure: a systematic review and meta-analysis. Lancet 382(9897):1039–1048
Song L, Song H, Lin J, Wang C, Yu M, Huang X, Du L (2017) PM2.5 emissions from different types of heavy-duty truck: a case study and meta-analysis of the Beijing-Tianjin-Hebei region. Environ Sci Pollut Res 24(12):11206–11214
Tai AP, Mickley LJ, Jacob DJ (2010) Correlations between fine particulate matter (PM2. 5) and meteorological variables in the United States: Implications for the sensitivity of PM2. 5 to climate change. Atmos Environ 44(32):3976–3984
Tseng KS (2006) Characterization of the compositions of coarse and fine atmospheric particulates collected in the Pingtung urban area. Master thesis. https://hdl.handle.net/11296/2ny28r
TW EPA (2020) Air quality protection policy planning. https://air.epa.gov.tw/EnvTopics/AirQuality_1.aspx
TW EPA (2011) Guideline for health risk assessment. https://www.epa.gov.tw/cpDownloadCtl.asp?id=6146
TW EPA (2012) The annual report of air pollution control in Taiwan (R.O.C.) in 2012. https://air.epa.gov.tw/EnvDownload/AirQuality/92%E5%B9%B4%E8%87%B3105%E5%B9%B4%E7%A9%BA%E6%B0%A3%E6%B1%A1%E6%9F%93%E9%98%B2%E5%88%B6%E7%B8%BD%E6%AA%A2%E8%A8%8E/101%E5%B9%B4%E7%A9%BA%E6%B0%A3%E6%B1%A1%E6%9F%93%E9%98%B2%E5%88%B6%E7%B8%BD%E6%AA%A2%E8%A8%8E.pdf
TW EPA (2013) The annual report of air pollution control in Taiwan (R.O.C.) in 2013. https://air.epa.gov.tw/EnvTopics/AirQuality_8.aspx
TW EPA. Air quality protection policy planning. https://air.epa.gov.tw/EnvTopics/AirQuality_1.aspx
TW EPA. Laws and regulation database. https://law.moj.gov.tw/LawClass/LawHistory.aspx?pcode=O0020007
TW EPA. Stationary pollution source air pollutant emissions standards. https://oaout.epa.gov.tw/laW/EngLawContent.aspx?lan=E&id=81
TW EPA. Taiwan air quality monitoring network. http://taqm.epa.gov.tw/taqm/en/YearlyDataDownload.aspx
TW EPA. Vehicular air pollutant emission standards. https://law.moj.gov.tw/LawClass/LawAll.aspx?pcode=O0020003
US Environmental Protection Agency. Health effects assessment summary tables (HEAST), US Environmental Protection Agency. https://www.epa.gov/
US EPA (1995) Guidance for risk characterization at the U.S. Environmental Protection Agency. U.S. Environmental Protection Agency, Science Policy Council, Washington, DC. https://www.epa.gov/sites/production/files/2014-11/documents/guidelines_exp_assessment.pdf
US Environmental Protection Agency Provisional peer reviewed toxicity values for superfund. https://hhpprtv.ornl.gov/
US EPA (2013) Draft technical guidance for assessing environmental justice in regulatory analysis 2013b. Washington, D.C. http://yosemite.epa.gov/sab/sabproduct.nsf/0/0F7D1A0D7D15001B8525783000673AC3/$File/EPA-HQOA-2013-0320-0002[1].pdf
US EPA (2001) Risk characterization handbook. https://www.epa.gov/risk/risk-characterization-handbook
US EPA (2014) Framework for human health risk assessment to inform decision making
Vedal S, Kim SY, Miller KA, Fox JR, Bergen S, Gould T (2013) NPACT epidemiologic study of components of fine particulate matter and cardiovascular disease in the MESA and WHI-OS cohorts. National particle component toxicity (NPACT) initiative report on cardiovascular effects. Research report, 178
Wang CK (2000) The study of atmospheric aerosols in Taiwan—the characteristics and sources of particles in Kao-hsiung and Taipei areas. Master thesis. https://hdl.handle.net/11296/re792a
Wang F, Zhou Y, Meng D, Han M, Jia C (2018) Heavy metal characteristics and health risk assessment of PM2.5 in three residential homes during winter in Nanjing. China Build Environ 143:339–348
Wang J, Wang S, Voorhees AS, Zhao B, Jang C, Jiang J, Hao J (2015) Assessment of short-term PM2.5-related mortality due to different emission sources in the Yangtze River Delta, China. Atmos Environ 123:440–448
Wang SL (2011) Chemical and toxicological characterization of airborne fine particulates (Pm2.5) as a risk factor associated with lung cancers in Taiwan. Ministry of Science and Technology report: NSC100-3112-B400-005
Wang Y, Komonpipat S (2020) Revisiting the environmental Kuznets curve of PM2.5 concentration: evidence from prefecture-level and above cities of China. Environ Sci Pollut Res 1–13. https://doi.org/10.1007/s11356-020-07621-x
Wei X, Gao B, Wang P, Zhou H, Lu J (2015) Pollution characteristics and health risk assessment of heavy metals in street dusts from different functional areas in Beijing, China. Ecotoxicol Environ Saf 112:186–192
Weng MJ (2014) Chemical composition and source apportionment of ambient fine particulates in Taichung and Pingtung area. Master thesis. http://hdl.handle.net/11455/91681
Wilhelm M, Ghosh JK, Su J, Cockburn M, Jerrett M, Ritz B (2011) Traffic-related air toxics and term low birth weight in Los Angeles County, California. Environ Health Perspect 120(1):132–138
Wu CA (2013) Field monitoring, chemical analysis, and control strategies of fine particles (PM2.5) in the Atmosphere of Kaohsiung City
Wu CF, Wu SY, Wu YH, Cullen AC, Larson TV, Williamson J, Liu LJS (2009) Cancer risk assessment of selected hazardous air pollutants in Seattle. Environ Int 35(3):516–522
Xing YF, Xu YH, Shi MH, Lian YX (2016) The impact of PM2. 5 on the human respiratory system. J Thorac Dis 8(1):E69
Xu G, Jiao L, Zhang B, Zhao S, Yuan M, Gu Y, Tang X (2017) Spatial and temporal variability of the PM2. 5/PM10 ratio in Wuhan, Central China. Aerosol Air Qual Res 17:741–751
Xue X, Chen J, Sun B, Zhou B, Li X (2018) Temporal trends in respiratory mortality and short-term effects of air pollutants in Shenyang. China Environ Sci Pollut Res Int 25(12):11468–11479
Yan D, Lei Y, Shi Y, Zhu Q, Li L, Zhang Z (2018) Evolution of the spatiotemporal pattern of PM2.5 concentrations in China—a case study from the Beijing-Tianjin-Hebei region. Atmos Environ 183:225–233
Yang B, Guo J, Xiao C (2018) Effect of PM2.5 environmental pollution on rat lung. Environ Sci Pollut Res 25(36):36136–36146
Yang J, Seo JH, Jeong NN, Sohn JR (2019a) Effects of legal regulation on indoor air quality in facilities for sensitive populations—a field study in Seoul, Korea. Environ Manag 64(3):344–352
Yang Q, Yuan Q, Yue L, Li T, Shen H, Zhang L (2019b) The relationships between PM2.5 and aerosol optical depth (AOD) in mainland China: about and behind the spatio-temporal variations. Environ Pollut 248:526–535
Yang TT, Hsu CY, Chen YC, Young LH, Huang CH, Ku CH (2017) Characteristics, sources, and health risks of atmospheric PM2.5-bound polycyclic aromatic hydrocarbons in Hsinchu, Taiwan. Aerosol Air Qual Res 17(2):563–573
Yilan County Environmental Protection Bureau (Yilan county EPB) (2014) Air quality operation and maintenance management and air quality monitoring survey and cause analysis plan in areas with high concentration of fine suspended particulates (PM2.5). https://www.ilepb.gov.tw/OpenAttch_id.ashx?guid=8bbb0aa9-5c39-479d-be93-bc1986498fa7
Yilan County Environmental Protection Bureau (Yilan county EPB) (2015) Air quality operation and maintenance management, PM2.5 and harmful air pollutants source monitoring and promotion plan. https://www.ilepb.gov.tw/OpenAttch_id.ashx?guid=1ca408ba-5fdf-4704-ae71-bcfe9d6227de
Yuan CS (2015) Tempospatial distribution and transboundary transportation of atmospheric fine particle across Bashi channel, Taiwan Strait, and South China Sea. The National Science Committee of the Executive Yuan, Special Research Project, NSC
Yilan County Environmental Protection Bureau (Yilan county EPB) (2017a) Air quality improvement and maintenance and environmental monitoring plan. https://www.ilepb.gov.tw/OpenAttch_id.ashx?guid=0023a2a5-1f75-4c31-9611-eea0077ea860
Yilan County Environmental Protection Bureau (Yilan county EPB) (2017b) Mobile pollution source inspection and control and locomotive exhaust regular inspection service management plan. https://www.ilepb.gov.tw/OpenAttch_id.ashx?guid=1e658871-19ef-400a-83e5-ca83ec7b28e3
Yilan County Environmental Protection Bureau (Yilan county EPB) (2019a) Air quality improvement and maintenance and environmental monitoring plan. https://www.ilepb.gov.tw/OpenAttch_id.ashx?guid=14cb2d56-1b73-4364-a4e9-a4c8e5e5117f
Yilan County Environmental Protection Bureau (Yilan county EPB) (2019b) Traffic air quality monitoring survey project. https://www.ilepb.gov.tw/OpenAttch_id.ashx?guid=4e05d9b0-de29-4a6b-8757-a5a4708490f5
Zhou Y, Chang FJ, Chang LC, Kao IF, Wang YS (2019) Explore a deep learning multi-output neural network for regional multi-step-ahead air quality forecasts. J Clean Prod 209:134–145
Zhou Y, Chang LC, Chang FJ (2020) Explore a multivariate Bayesian uncertainty processor driven by artificial neural networks for probabilistic PM2.5 forecasting. Sci Total Environ 711:134792
Acknowledgements
The authors gratefully acknowledge support from the Ministry of Science and Technology, Taiwan, ROC (Grant number: MOST 106-3114-M-002-001-A, MOST 108-2119-M-002-017-A, and MOST 107-2811-M-002-3118). The datasets provided by the Environmental Protection Administration, Taiwan, ROC, are acknowledged. The authors would like to thank the editors and anonymous reviewers for their constructive comments that are greatly contributive to improving the paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wang, YS., Chang, LC. & Chang, FJ. Explore Regional PM2.5 Features and Compositions Causing Health Effects in Taiwan. Environmental Management 67, 176–191 (2021). https://doi.org/10.1007/s00267-020-01391-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00267-020-01391-5