
Abstract
This study examines the adoption of latrines provided as part of reconstruction efforts after the 2004 tsunami in India. Primary data from 274 households encompassing 1154 individuals were collected from 14 villages. GLM and GLMM tests indicate that sex (more females adopted than males) is a statistically significant factor in latrine adoption (p = 0.046 and p = 0.005, respectively), while income, education, and male age cohorts were significant only in the GLM model. Regression analyses show that six social and demographic variables are somewhat predictive of latrine usage (R2 = 0.123). Thus, while quantitative methods provided a contextual summation, qualitative methods ultimately explained why individuals chose to adopt or abandon the latrines. Interviews (n = 76) and focus group discussions (n = 14) revealed that latrine adoption is influenced by cultural conceptualizations of purity, pollution, and space. For example, conceptualizations of purity and pollution led some households to deem latrines as profane and thus a barrier to the entry of gods, while spatial constraints forced others to convert latrine space to other beneficial uses (e.g., puja room and storage area). Finally, the cost of pumping septic tanks and shared infrastructure arose as barriers to latrine adoption. These barriers underscore the importance of economics as well as community demand, capacity, and cohesion in latrine adoption.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Access to toilets remains a pressing challenge. More than two billion people lack access to improved sanitation, with many resorting to open defecation (OD), which is also understood to include urination and menstrual hygiene management (WHO/UNICEF 2017). To combat poor access to sanitation, the United Nations’ (UN) Sustainable Development Goal 6 seeks to achieve access to improved sanitation for all. This is an ambitious goal, especially considering that providing access to sanitation is just the first step. Adoption and consistent use—which requires changing behaviors and often changing culture—is the second and often more difficult step. This study investigates which factors led to latrine adoption or abandonment among households that were provided latrines cost-free as part of reconstruction after the 2004 tsunami in India. We define adoption as consistent and sustained usage at least six months after the introduction of latrines (Hulland et al. 2015).
The coast of southeastern India, and the districts of Nagapattinam, Tamil Nadu and Karaikal, Puducherry in particular, were severely affected by the 2004 Indian Ocean tsunami. The model for reconstruction—which consisted of memorandums of understanding (MoUs) between local governments and nonprofits—promised new disaster-resistant houses with attached latrines to all affected populations. As a result, thousands of households gained access to improved sanitation. While the tsunami ushered in a unique opportunity to reconstruct civil and environmental infrastructure on a grand scale, the outcomes in terms of sanitation are contentious. A leading national newspaper, in a recent article on post-tsunami reconstruction titled “Open defecation still a scourge in Nagapattinam,” claimed that “toilets in several tsunami rehabilitation colonies are in total disarray” (The Hindu 2016). The article contends that latrines were constructed upon a “wrong understanding of the [local] terrain” and that residents were not adequately sensitized, the combination of which sent residents “back to the stone age.” News coverage has continued, with another article arguing that sanitation infrastructure has now “crumbled,” making it impossible for residents to “evade the inevitability of defecating in the open” and further resulting in “school and college-going girls shedding dignity and self-respect” (The Hindu 2017). The article goes on to claim that such poor reconstruction outcomes will make it impossible for the region to be declared OD free for years to come.
Rather than hitching to the polemicized view that the introduction of latrines was an unequivocal “failure,” we operate from an antecedent foundation that failure and success are heterogeneous across both individuals and space as a function of complex interactions among the built environment (i.e., latrine) and numerous social, physical, and hyrdrometeorological systems. We harness this theoretical foundation—rooted in geographic understandings of people, spaces, places, and their interactions—to investigate latrine adoption in India. The specific research questions are, in the case of 14 reconstructed villages in Nagapattinam and Karaikal districts that were provided latrines: (1) what is the rate of latrine adoption and (2) which factors influence latrine adoption? The objective is to better understand how such factors manifest and how they can be addressed or incorporated in future humanitarian aid for sanitation.
Background
The Sanitation Landscape
Sanitation is a matter of hygiene, health, and human rights. In 2010, the UN General Assembly recognized access to improved sanitation as a universal human right, even going so far as to situate it as a precursor to attaining other human rights (UNGA 2010). The right to sanitation (which equates to a recognition with no guarantee of access), development agendas such as the UN Sustainable Development Goals, and programs to alleviate poverty and boost economies underlie efforts to provide improved sanitation throughout the Global South. However, providing sanitation infrastructure is only the first part of the equation: the second and more difficult part is getting people to use the infrastructure. This is especially critical, because lessons from the latter part of the equation can be leveraged to inform the former.
In the absence of improved sanitation, pathogens are not safely segregated and are more capable of moving through fecal–oral, water, and land routes to infect a greater number of people. Improved sanitation, on the other hand, disrupts transmission routes and helps prevent communicable diseases such as cholera and giardiasis, zoonoses such as schistosomiasis and trachoma, vector-borne diseases such as malaria and dengue, and chronic conditions such as malnutrition and stunting (Bartram and Cairncross 2010; Freeman et al. 2017). Beyond public health, sanitation is also an integral component of environmental management (e.g., soil quality and ground, surface, and drinking water quality) and women’s empowerment initiatives (Hirve et al. 2015; Deilami et al. 2017).
Billions of dollars, extensive resources, and numerous supranational programs have been deployed to provide improved sanitation. Still, more than two billion lack access and OD remains widespread in many parts of the world. India continues to lag behind on the sanitation ladder. A staggering 60% of Indians lack access to improved sanitation (World Bank 2017), and OD is so prevalent that it has emerged as a public health priority (Spears et al. 2013; Coffey and Spears 2017). To address the sanitation gap and discourage OD, the Government of India initiated the Total Sanitation Campaign program in 1999 and Swachh Bharat Abhiyan (Hindi for “Clean India Mission”) program in 2014. The programs, which were not directly utilized for latrine construction at the study sites, aim to furnish every Indian household with access to improved sanitation and to change behavior through community capacity building, the deployment of sanitation “foot soldiers,” and shaming the practice of OD (GoI 2018; KPMG 2018). However, concealed in the latrine adoption figures of such programs lies the intrinsic flaw of measuring whether individuals have access rather than measuring whether the infrastructure is actually used. That is, global, regional, and national measures merely quantify how many individuals have access to sanitation, whereas the number who actually (consistently) use the infrastructure is necessarily less due to factors of cost, culture, and suitability of infrastructure to the respective biophysical and engineered environment.
Latrine Adoption in India
Several factors, indicators, and motivators affect latrine adoption in India. On the environmental side, compatibility with climate, soil type, land use, and other physical features have been identified as governing factors (Paterson et al. 2007; O’Reilly and Louis 2014). For example, pit latrines and leach pits may not be suited to coastal environments with high water tables and/or monsoon climates (Ludwig and Browder 1992). In terms of resource availability, land security (i.e., access to private or communal land to support sanitation infrastructure) and access to an adequate quantity of water have been identified as limiting factors (Routray et al. 2015; McMichael 2018). On the latter, it is recognized that “toilet users are water users..., therefore access to water is key” (O’Reilly 2012: p. 8). Water is physically required to flush toilets, perform ablutions, and wash hands, yet access to one resource (latrine) does not guarantee access to the other (water). Quality of infrastructure impacts latrine adoption. For example, beneficiaries in rural North India were less likely to use latrines when quality was deemed insufficient, pits were dug too shallow, or pit volume was too small to meet household demand (Jewitt et al. 2018; Rashid and Pandit 2018).
Several studies have also investigated social, economic, and cultural underpinnings of latrine adoption in India. In line with Diffusion of Innovations Theory (Katz 1961; Rogers 2003), individuals are more likely to adopt latrines when they perceive that the infrastructure is more convenient or saves time compared to current and alternative methods (Dickinson et al. 2015). Similarly, individuals are more likely to adopt latrines when they perceive health benefits, such as lower incidence of diarrhea, hookworm, and other waterborne diseases (Jha 2003; Pattanayak et al. 2007). However, the perception that latrines reduce disease burden is not always accepted by beneficiaries (Banda et al. 2007), and there is little evidence that perceived long-term health benefits are actually achieved (McMichael and Robinson 2016). Socioeconomic status and social location are also variables in the latrine adoption calculus. For example, middle class populations were more likely to use latrines in Kolkata (Juran and Lahiri-Dutt 2017), whereas populations below the poverty line were more likely to use latrines in Odisha (Pattanayak et al. 2009; Dickinson et al. 2015). In the latter case, subsidies to build latrines led to greater latrine construction among relatively poorer households. Engaging aspects of sociology and community, evidence also shows that peer pressure and shaming (i.e., creation of a “social contract”) lead to increased adoption (Pattanayak et al. 2007; O’Reilly et al. 2016). These studies also argue that previous experience using latrines and prior existence of latrines in a community lead to greater adoption.
Gender has been established as a determinant of latrine adoption in India. Much of this stems from the reality that women—especially young and newlywed women—seek privacy from male onlookers who may stare, gossip, harass, or commit sexual violence (Khanna and Das 2015; Caruso et al. 2017). Thus, a safe space is engineered when a latrine door can be locked and areas near the latrine are well-lit. While greater adoption rates are partly due to women actively seeking personal safety, elevated rates of female adoption are also a function of males seeking to “protect” female relatives from the androcentric societies they inhabit—in essence subverting female agency in an effort to preserve chastity and family reputation. Gender dynamics are variable when latrine infrastructure confronts social systems. Recent explorations suggest that cultural expectations may actually dissuade women from introducing latrines because they add to women’s gender-delineated roles. Latrines can increase the economic, temporal, and opportunity costs of women who are tasked with stocking latrines with a source of water (i.e., to flush “pour-flush” latrines) as well as cleaning (O’Reilly 2006; Routray et al. 2015). Thus, while latrines address some aspects of gender, they may also increase women’s daily labor to the point that “if women do not work, toilets may not get used” (O’Reilly 2012: p. 8).
Latrine adoption in India is also impacted by epistemological conceptualizations of purity, pollution, and space. These paradigms, heavily influenced by Hinduism, situate bodily fluids (e.g., feces, urine, and menstrual fluids) as inherently profane, which in turn presents obstacles to latrine adoption (Barnard and Spencer 2002; Tagat and Kapoor 2018). As articulated by Jewitt (2011), “taboos surrounding human feces have often (but not always, and not everywhere) created barriers to the development of more effective and/or sustainable excreta-management systems [in India]” (p. 610). These perceptions of human waste ultimately interact with how physical space is arranged, used, and not used. For example, socio-cultural and religious beliefs—rooted in Vaastu Shastra, which provides guidelines for the spatial layout of houses and settlements based on Hinduism (Sarkar 2008)—dictate that latrines and human waste sully the household, automatically turning domestic space from pure to profane. In practice, these perceptions cause some to resist the introduction and adoption of latrines in favor of maintaining a relatively pure space, which typically results in OD.
Given the range of environmental and social factors, latrine adoption in India is not ubiquitous. For example, Barnard et al. (2013), in a study on latrine adoption in Odisha, found that 39% of newly introduced latrines remained unused. Furthermore, only 37% of households and 47% of individuals used the latrines for defecation. In a similar study in rural North India, Coffey et al. (2014) found that 55.4% of households with latrines opted for OD, with another 18.3% having at least one household member that practiced OD. Patil et al. (2013), in a study of 80 villages in Madhya Pradesh, found that while government efforts increased the number of households with latrines by 19%, there was only a 10% reduction in OD. In rural Tamil Nadu, Banda et al. (2007) found that 16.7% of households with a latrine still practiced OD, while Yogananth and Bhatnagar (2018) found that 45.2% of households with a latrine still practiced OD. Finally, in a study in West Bengal and Himachal Pradesh, O’Reilly et al. (2016) found that latrines were used 1.51 times per day per capita. However, and in contrast to aforementioned studies, individuals tended to use latrines for defecation and opted to urinate in areas outside of the household and village.
This study advances the literature on sanitation in India by investigating which factors influence latrine adoption in the context of large-scale disaster reconstruction. Furthermore, this study is unique because it: (1) combines quantitative, qualitative, and ethnographic methodological approaches; (2) is one of relatively few studies in India not conducted in the North (many studies are located 1000–2000 km from the study area and thus in different socio-physical landscapes); and (3) examines latrine adoption in the long-term (roughly 10 years after the introduction of infrastructure compared to six months to 1–2 years as is common in other studies).
Study Area and Methods
This study was conducted in the southeastern coastal districts of Nagapattinam (Tamil Nadu) and Karaikal (Puducherry), India, which were devastated by the 2004 Indian Ocean tsunami. The model for reconstruction, consisting of MoUs between local governments and humanitarian agencies, promised new disaster-resistant houses to all affected populations. Furthermore, all houses were required to have an attached latrine (GoP 2005; GoTN 2005). Latrines were introduced through a “provision and adoption” model in which the infrastructure was provided cost-free with little to no education or sensitization.
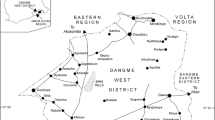
Fourteen reconstructed villages (selected randomly from 35) were examined across three field visits from 2015 to 2017 (Fig. 1). The 14 study sites, seven each in Nagapattinam and Karaikal, average about 200 households and have been occupied since roughly 2007 (Table 1). The study sites are both urban and rural (seven of each) as delineated by official political jurisdictions (i.e., territorial boundaries) and functional governance (i.e., municipal or panchayat governments, which differ in composition, organization, and powers). The sites also comprise different religions (e.g., Hindu, Muslim, and Christian), livelihoods (e.g., fishing, agriculture, and daily wages), and social locations (e.g., middle income, low income, and scheduled caste). Twelve villages were relocated and two were reconstructed in situ (one in each district). Each village was visited 2–3 times encompassing the dry (May–August) and monsoon (October–December) seasons.

The study area and study sites
This study employs a mixed methods approach aimed at triangulating narratives and establishing rigor and reliability in research findings (Baxter and Eyles 1997). First, proportional random sampling was used to survey households in each study village, resulting in 274 households (minimum of 18 at each site) totaling 1154 individuals (nmale = 581, nfemale = 573). The survey considered subjects age five and above, leaving the sample population with an average household size of 4.2. The structured, mostly close-ended survey instrument gathered categorical and continuous data on the age of all household members; sex of all household members; total household income; highest completed level of education in the household; whether the household is in a rural or urban territory; and whether each household member uses (or does not use) the latrine and why (or why not).
Data were analyzed using generalized linear model (GLM) and generalized linear mixed model (GLMM) tests to identify if six socioeconomic and demographic factors (age, sex, education, income, household size, and rural–urban) impact latrine adoption. GLM(M) tests were employed due to their ability to analyze complex situations, handle mixtures of categorical and continuous data, and account for the simultaneous effects of multiple variables (Nelder and Baker 2006). The use of parallel GLM and GLMM tests is appropriate in this case. GLM treats individuals as autonomous units capable of making decisions in their own right, while GLMM controls for random effects within the household, or the assumption that individuals (and thus behaviors) within each household are relatively similar and should thus be treated as a quasi single unit. Together, the tests consider both the intra-household (i.e., individual) and household scales, rendering each test insightful in its treatment of data. This is important because, while many households are universal in their adoption or abandonment of latrines, a considerable number of households (10.2%) demonstrated mixed latrine usage (i.e., some members adopted while others abandoned the latrines). Finally, stepwise binomial logistic regressions were used to test the predictive value of the six independent socioeconomic and demographic variables (age, sex, education, income, household size, and rural–urban) against the dependent variable of usage status. All analyses were conducted using SPSS version 21.0.
Given difficulties measuring anthropic phenomena (i.e., behaviors) in absolute or quantitative terms (Crampton and Elden 2006), survey data were triangulated with several layers of qualitative data. First, the survey ended with an open-ended question on why individuals chose to adopt or abandon the latrines (multiple responses permitted). The responses generated descriptive data on rationale that govern behaviors related to latrine infrastructure, geography, and socio-cultural dynamics. Next, a subset of surveyed households (n = 76, minimum of five at each site) were purposively selected for follow-up interviews lasting 30–60 min. The interviewees were purposefully selected to access knowledge and lived experiences from households that exhibited a range of interactions with the latrines. Furthermore, the interviews were “mobile interviews” (Macpherson 2016), which enabled interviewees to escort the interviewer to latrine and sanitation features, discuss tangible issues in real space, and “teach” the interviewer about latrine infrastructure challenges. This approach also allowed the interviewer to apply observational theories (Reckwitz 2002), cultivate rapport, and challenge positionality by placing interviewees in command. Finally, a focus group discussion (FGD) with 6–9 participants was organized at each of the 14 villages. FGDs lasting 45–60 min offered a dialogic setting in which residents shared how the latrines were introduced, their level of input, the existence of any sensitization campaigns, and issues related to using or not using the latrines over time and across seasons. Collectively, this mixed methods approach helped to verify, refute, and add nuance to the findings.
Results
Latrine Adoption Rates
Most households (71.5%) reported that all members adopted their latrines (Table 2). A minority of households (14.6%) abandoned their latrines, while the remaining households practiced either intermittent (e.g., during monsoon season, at night, and times of illness) or mixed use (i.e., only a portion of the household uses the latrine). These rates mirror the individual level, in which most adopted the latrines (76.1%), a minority did not (17.2%), and the remaining use latrines intermittently. Most males and females adopted the latrines, but female adoption is 6.6% points greater. While the urban and rural settings both had a majority of latrine adopters, rural households and individuals adopted at greater rates. Finally, type of infrastructure appears to matter as individuals provided with leach pits adopted latrines at a rate of only 53.1% (remaining 34.7% practice OD and 12.2% practice intermittent use).
Statistical Results
Comparative statistical analyses identified variables that significantly impact latrine adoption (Table 3). Four variables are significant at the individual (GLM) level: sex (women more likely to adopt compared to males); male age cohorts (specific cohorts of males (40–44 and 70–74) are more likely to adopt than other male cohorts); income (adoption and income are positively associated); and education (adoption and education are positively associated). However, sex is the only significant variable when the household was considered as a quasi single unit (i.e., GLMM). Some of these results are visible in Fig. 2, which shows relatively higher rates of latrine adoption among women compared to men across the ages, and Fig. 3, which plots latrine adoption against household income.

Percent who practice open defecation by age and sex

Percent who practice open defecation by income
Regression analyses produced an R2 value of 0.126 for the set of six socioeconomic and demographic variables (age, sex, education, income, household size, and rural–urban). However, two of the variables were insignificant (urban–rural and age), so a second regression was conducted with the remaining variables of significance generating an R2 value of 0.123. Ultimately, the quantitative model was only weakly predictive of latrine adoption (which is not abnormal for social scientific studies with a large sample size), justifying our inclusion of qualitative analyses to better understand latrine adoption.
Rationale for Latrine Adoption and Abandonment
Survey respondents were asked to state their rationale for adopting, abandoning, or using latrines intermittently. The open-ended, multiple response question revealed the top rationale for adoption as: convenience and comfort (81.1%); privacy, safety, and security (41.2%); hygiene, purity, and “naturalness” (31.7%); and that latrines are “modern” (12.0%). Alternatively, top rationale for abandonment were: “it’s [OD] what we always did” (50.5%); hygiene, purity, and “naturalness” (50%); location of latrine in the house (36.4%); low-quality construction (28.3%); limited space is too valuable to use as a latrine (21.2%); and convenience and comfort (18.7%). Lack of water supply and “it’s [OD] free to go outside” also arose as rationale among nonadopters (17.2 and 13.1%, respectively). Finally, latrine adoption is not black and white. Individuals who use latrines intermittently stated that they do so during the monsoon and inclement weather (65.4%); in times of illness (44.9%); for cost efficiency (i.e., a rate that will not fill the septic tank, which requires payment for pumping); and during the night (19.2%). Overall, findings demonstrate that reasons to use latrines are multifaceted, with stated rationale linked to issues of health, economics, latrine quality, culture, and space. These rationale will be deconstructed as the crux of the discussion section.
Discussion
Quantitative Interpretations of Latrine Adoption
Findings demonstrate that most subjects—whether classified by setting (rural or urban), age, sex, income, or education level—adopted newly provided latrines in Nagapattinam and Karaikal. Sex (greater female adoption) was a statistically significant factor, which aligns with previous studies in India and the bulk of the sanitation literature. No significant difference was found in adoption between rural and urban populations, although adoption rates were higher among rural households and individuals compared to the urban setting. This finding contradicts conventional development narratives in which urban–rural hierarchies “automatically” result in higher adoption rates among urban populations (Tumwine et al. 2003; Montgomery et al. 2009). While rural areas may have less access to infrastructure and exhibit less community demand (in terms of population) than urban areas, this finding suggests that, once latrines are introduced, rural adoption rates can be as high and even higher. Furthermore, greater income and education may not significantly influence latrine adoption in the case of Nagapattinam and Karaikal. While both factors were significant (p < 0.0001) at the individual scale (GLM), they were insignificant (income p = 0.666, education p = 0.275) at the household scale (GLMM). This again problematizes conventional notions of development and previous studies in which income and education were positively associated with latrine adoption (Torras and Boyce 1998; Bouabid and Louis 2015; Dickinson et al. 2015). Ultimately, these contexts are extremely complex and, given the findings, there is a need to transcend overly simplistic comparisons to instead focus on the features present within specific political territories and populations, such as levels of capacity, built and natural environment attributes, and the lived experiences of those who inhabit the geographies of question.
Findings reveal higher rates of adoption compared to similar studies in India. Overall, only 14.6% of households abandoned their latrines, compared to 39% in Odisha (Barnard et al. 2013) and 55.4% in Haryana, Madhya Pradesh, Bihar, Rajasthan, and Uttar Pradesh (Coffey et al. 2014). There are many potential factors at play. A first caveat is that most subjects were provided septic tanks, which often demonstrate higher uptake compared to leach pits that are the focus of many other studies (see Coffey et al. 2014; Gupta et al. 2016). Second, most studies on latrine adoption in India have been conducted in the North, whereas this study was conducted in the South. North and South India not only exhibit marked differences in culture, language, and religion, but also in levels of economic development, education, women’s rights, and social mobility—which are generally greater in the South (Epstein 1962; Dyson and Moore 1983). These contrasts are particularly evident in the relatively well-off territories of Tamil Nadu and Puducherry where the study took place. However, we caution that this North-South divide may not carry over to the sphere of sanitation, as demonstrated in recent studies in Tamil Nadu by Yogananth and Bhatnagar (2018) in which 45.2% of households with latrines still practiced OD, and O’Reilly et al. (2017) in which caste relations arose as the most formidable barrier to adoption. Furthermore, this study utilizes a longitudinal perspective in which research was conducted roughly 10 years after latrines were introduced. This lag in sampling allowed study participants to interact with the latrines for an adequate period of time, observe their utility across the seasons, maintain and improve the latrines or let them fall into disrepair, and ultimately choose to adopt, abandon, or use latrines intermittently. Lastly, surveys and surveyors are imperfect. While the survey was piloted and designed to be as straightforward as possible, there is always the possibility that the questions and surveyor were not objective, not to mention that respondents may have neglected to provide accurate information for reasons manifold (e.g., positionality, subalterneity, recall error, and the nature of discussing an inherently private matter). While we posit these critiques for the sake of discussion and research clarity, our task as researchers was to be objective as possible and record responses at face value.
While both statistical tests established sex (greater female adoption) as significantly greater, the remaining variables and regression analyses provided limited insight on underlying factors. Thus, while quantitative methods facilitated an initial interrogation of the research questions, they failed to capture the entire story. We, therefore, argue that more insightful were the qualitative methods, which uncovered the socio-cultural dynamics that ultimately manifest in latrine adoption or abandonment.
Qualitative Deconstruction of Latrine Adoption
Qualitative data—in the form of stated rationale for latrine adoption/abandonment and quotes from interviews and FGDs—help illustrate the underlying catalysts and barriers to latrine uptake in Nagapattinam and Karaikal. Prominent justifications are discussed in this and the subsequent section, with some justifications being more physical, environmental, and tangible (e.g., latrine quality, climate, and monetary costs) while others are shaped by deeply embedded socio-cultural dynamics.
The number one rationale for adopting latrines is convenience and comfort (reported by >81% of adopters). Participants claimed that it is more convenient and comfortable to use a latrine on their premises compared to traveling a longer distance to the coastline, riverbank, or shrubby area. As argued by an FGD participant in Sellur, “Why would I want to walk to the river and get wet and dirty when I can just go in my house? It’s easier and faster and you don’t have to deal with other people.” This quote, representative of most who perceived latrines as relatively convenient and comfortable, leads to the second most cited rationale of privacy, security, and safety (reported by >41% of adopters). While this rationale was primarily voiced by women, it was also reported by several patriarchs who stated that they value the safety latrines provide for female household members. This finding is best captured by a female in Kottucherrymedu who said, “It’s better to use the toilet because outside I get a panic from safety issues,” and the patriarch of the family who quickly chimed in: “The toilet is safer for my family. Now I don’t have to worry about them as much.” Finally, it should be mentioned that the top two rationale (convenience and comfort followed by privacy, security, and safety) tended to be cited by elderly participants. Elderly respondents stressed that they value a latrine on the premises due to issues of mobility, joint pain, and being close to family members in the event of a fall or health complications.
The third most common rationale (reported by >31% of adopters) is that latrines are more hygienic, pure, and “natural.” Respondents stressed that a latrine on the premises is healthier and more hygienic than OD because the household controls usage, maintenance, and, most importantly, cleanliness. As argued by an interlocutor in MGR Nagar: “We maintain our toilet and keep it in good condition, so it’s a clean place and better than going outside. People who complain about the smell [of their toilet] don’t keep their toilet clean!” Finally, 12% of respondents contend that latrines are a symbol of modernity. Adopters emphasized that having and using a latrine are milestones along the trajectory of achieving (global) middle class status.
Qualitative Deconstruction of Latrine Abandonment
The most cited rationale for abandoning latrines (reported by 50.5% of nonadopters) was that OD is the dominant historical method of relieving oneself. This response is difficult to distill since it requires unpacking the human ecology and behavioral psychology of complex communities and cultures. However, it can be dissected by examining why OD is the dominant historical method of relieving oneself. The reason, which is the second most cited rationale among nonadopters (50%), is that OD is more hygienic, pure, and “natural.” As shared by an interlocutor in Kallikuppam: “We prefer to go outside because it’s cleaner and freer. There is no smell and the air is fresh and clear. It’s more natural.” This perception is rooted in a purity-pollution binary borne out of Hinduism. This socially constructed binary, which extends far beyond interpersonal relations and untouchability, situates bodily fluids, such as urine, feces, and menstrual fluids as inherently profane. These perceptions are even codified in Vaastu Shastra (Sanskrit for “science of architecture”), a religious text that provides detailed schematics to auspiciously configure houses and settlements according to the Hindu cosmology. Based on Vaastu Shastra and dominant cultural-religious practices related to the sacred and profane, many households argued that latrines sully the household and therefore render it an impure space. In addition to sullying domestic space, participants claimed that latrines make food prepared in the household impure (especially when it shares a wall with the kitchen) and that it is embarrassing and insulting to serve such food to guests. Moreover, participants claimed that Lakshmi, an important Hindu goddess who is worshiped every morning, may not enter the house if a latrine is present. Lakshmi—who is very sensitive to impurities—brings health, wealth, prosperity, and good luck. However, if a latrine is present then she may not bless the household with good fortune. These perceptions ultimately caused some to resist latrines in favor of maintaining a relatively pure domicile, which typically results in OD.
The spatial location of the latrine in the household, raised by 36.4% of interviewees, was the third most cited concern among non-adopters. This rationale is an extension of the purity-pollution binary in which individuals stated that they would be willing to use the latrines if they were situated in a more preferable location. For example, many nonadopters contended that they would use latrines if they did not share a wall with the kitchen; the septic tank was not located near the house; or the washroom and latrine were in separate rooms (i.e., one cannot obtain purity through bathing if the washroom and latrine share the same space). However, some claimed that they would only use a latrine if it is detached from the household. These contentions are best upheld by a participant in Melavanjore who argued, “The toilet is attached to the house and that’s a bad thing, it makes the house dirty and it can affect your life,” and another in Vettakaramedu who voiced:
We have water coming to the toilet room and we have enough water supply, but we still don’t use it [latrine]. The reason is that the septic tank was put in front of the house near the entryway, so we feel it’s not a good symbol of our house—it’s a bad symbol, it’s a bad thing! Guests have to walk over the tank to get into our house. The front of the house is also used to welcome gods, but if the tank is there then the gods might not come in. We never used the toilet. We filled it with cement so it can never be used!
These data demonstrate that a rigid form of spatio-cultural or theo-spatial semiotics is at play that impedes latrine adoption. While it is well established in the sanitation literature that intersections of purity and pollution underlie adoption (Srinivas 2002; Doron and Raja 2015), our findings on movements of the gods reinforce and add a new dimension to this important factor of adoption. An acknowledgment and incorporation of such dynamics remains key to improving future latrine introduction and sensitization campaigns in the region, such as existing Total Sanitation Campaign and Swachh Bharat Mission programs. It must be noted that several village leaders were provided house layouts prior to construction, and some were even offered a selection of 3–4 similar layouts. All layouts included an attached latrine and all clearly demarcated its location—including layouts that positioned the latrine adjacent to spaces later deemed offensive from the standpoint of purity (e.g., kitchen). However, no village leaders raised concerns to developers. Looking back, one interviewee from New Kallar commented:
The NGO shared a model of the tsunami house with us. We looked at it and thought, “OK, we’re getting a free house and that’s good enough for us.” That is what we needed at the time, so there was not any discussion. But after moving into the house and facing problems we realized that there were many things we needed differently.
Low quality construction and dissatisfaction with latrine infrastructure arose as the next top concern among non-adopters (cited by >28%). Some latrine pans were broken and some septic tanks were absent, unconnected to the latrine, or left incomplete by developers. Others complained that inferior construction materials (e.g., poor quality and broken bricks, weak cement due to too high of a sand to cement ratio) led tanks fill with precipitation during the monsoon season, leading to abandonment or intermittent use. Still others complained that the septic tanks are too small to accommodate the household or that a shared septic tank was installed in which neighboring houses are connected to a single tank. In the former case, some households began using the latrines, but ceased once the tanks filled. Pumping requires hiring a private company 1500–3000 Indian Rupees depending on volume, as lamented by a participant in MGR Nagar:
We used the toilet, but then we quit because the tank was full and the company said we would have to pay Rs. 2000 for pumping. We just left it full and started going outside. The tank has been sitting full for the past 3 years.
Another household in MGR Nagar also struggled with pumping their septic tank:
Our tank is full, but we are saving up money to do other work on the house. We might work on the kitchen or maybe a puja room [Hindu prayer room], we haven’t decided yet. We were happy using the toilet, but we prefer to spend pumping costs on another purpose for the family.
These cases demonstrate that some users, after having an adequate duration to observe latrine utility over time, elected to abandon their latrines based on economics, family goals, and marginal returns. These cases align with a recent study by Jewitt et al. (2018) in which improved sanitation became unimproved sanitation over time while others resorted to “stacking,” or alternating between a range of sanitation options due to seasonal and other factors.
Much has been written on shared and public latrines (see Fuller et al. 2014; Heijnen et al. 2015), but little has been written on shared septic tanks. In cases of joint tanks, households that abandoned their latrines were adamant that they will not contribute to pumping costs since they do not use their latrines. On the other hand, households that use their latrines contended that nonadopters are stingy, uncooperative, and have contributed to the tank being full due to bathing (i.e., water from bathing inadvertently drips into the latrine pan) and occasional latrine usage that they stubbornly deny. Regardless of who is correct, this context emphasizes the importance of community demand, capacity, and cohesion when appraising the long-term sustainability of joint and centralized infrastructure. Simply put, the questions of ‘for whom’ and ‘who pays’ remain vital, especially when there is no method to opt out.
Spatial constraints and the relative value of space also arose as chief concerns. More than 21% of latrine nonadopters cited that their houses are small and densely concentrated, leaving little functional space to satisfy the full range of domestic and cultural activities. Houses constructed by humanitarian agencies after the tsunami consist of a small living room, bedroom, kitchen, and combined bathroom/washroom. This one bedroom, nuclear-style layout cannot readily accommodate families greater than three or four, and many households are occupied by 5–7 persons given the cultural norm of extended families. This lack of functional space situates space occupied by latrines as highly valuable—especially when filtered through the lens that relieving oneself outside is “what we’ve always done” and that “it’s free to go outside.” Confronting scarcity of space, many households converted latrines to other uses, as shared by a household in Kizhakasakudimedu:
The houses are close together and small, so space is limited and shouldn’t be wasted on a toilet. Instead, it should put to better use and the outside can be used as a toilet. We used the toilet to make a puja room. We’ve gone [to the bathroom] outside our whole lives, so that’s not a problem and it’s comfortable for us. I’m happy with the toilet situation now because I go outside just like I used to before the tsunami, but now I also have a puja room.
A household in Samanthanpettai agrees with these sentiments:
Our tsunami house is fine. We were given a house with a toilet that we were able to change into a proper puja room. At the old house we didn’t have a proper puja room, and we never cared about having a toilet. If I don’t have one I’m fine, because I never had a toilet before anyway. Now with the toilet room we were able to make a puja room—at our old house we only had a small shelf on the wall as a puja room. Other people have used the toilet to store water and firewood, even goats.
Quite interesting here is that latrine space, often perceived as impure, is being converted into sacred space to worship the Hindu pantheon (even Lakshmi, whom many are concerned about deterring). Thus, while some households perceive latrine space as indelibly profane (i.e., prima facie, even if unused), some believe that it can be repurposed for other functions, even religious, as long as the space has not been used for its intended purpose. These examples demonstrate that trade-offs are being made in which available space is being allocated to the most valuable functional purpose. Families are (re)configuring space based on satisfying cultural and functional ends, which ultimately requires them to choose certain activities (e.g., puja room and storage) over others (e.g., latrine use). These frictions are particularly evident at the urban scale, where latrines must confront the same spatial barriers while likely being located inside the household due to physical constraints presented by dense and vertical urban housing development.
Convenience and comfort was reported as justification for latrine abandonment among 18.7% of nonadopters. Interestingly, convenience and comfort was the number one justification among adopters, who argue the opposite is true. Finally, lack of water supply was cited by 17.2% of nonadopters, which partly supports the argument that latrine users are necessarily water users: you cannot use one (latrine) without the other (water). The study sites are located in the Cauvery River basin, which demonstrates empirical water scarcity and stress (i.e., lack of renewable resources to support self-sufficiency and >80% usage-availability ratio). It appears that this context presents a barrier to both water supply and latrine adoption.
A final finding is that most non-adopters are not offended at having been provided with latrines. Paraphrasing several nonadopters, if they could go back in time they would still want their houses to come equipped with a latrine because “it’s an insult not to include a toilet as part of a modern house.” As shared by an interviewee in Sellur: “Everybody knows that a toilet is part of a pakka house [concept in Hindi denoting a good quality, concrete house]. If they didn’t give me a toilet then I would think, ‘what, I don’t deserve one?’ ” These perceptions are not only based on status and comparisons with others, but also on dominant epistemological beliefs that states and citizenhood are founded on principles of access to basic human services, such as education, healthcare, food, and water—although such access often remains unmet. The fact that humanitarian agencies and governments promised “modern” houses and infrastructure also likely led to expectations of gaining access to services and systems that mirror more Western configurations. This scenario gives rise to a situation in which, although the free infrastructure may be low quality, unused, or unwanted, it was still appreciated and perceived by beneficiaries as something they deserve or are entitled to as citizens of a modern society. However, we argue that this finding should not comfort development and humanitarian agencies, but instead underscore their need to introduce more sensitive and culturally valuable infrastructure from the outset.
Conclusions
This study advances the sanitation literature by examining latrine adoption in post-disaster South India. All study participants were provided a free house with an attached latrine as part of reconstruction after the 2004 Indian Ocean tsunami. This study is unique because it investigates latrine adoption in the long-term (roughly 10 years after introduction), employs a mixed methods approach with both statistical and ethnographic findings, and is one of relatively few studies not conducted in North India.
Quantitative findings indicated that most households (71.5%) and individuals (76.1%) adopted latrines in Nagapattinam and Karaikal. Sex was the only significant factor across both statistical tests (GLM p = 0.046, GLMM p = 0.005), with female adoption greater than male adoption. Income, education, and male age cohorts were significant in the GLM test, but not when random effects were considered at the household scale (GLMM). Income and education were thus difficult to interpret and warrant further investigation: both variables are either significant or insignificant depending on which test is conducted, yet the distribution of data show that both tests are justifiable and appropriate to report. Regression analyses indicated that six socioeconomic and demographic variables (age, sex, education, income, household size, and urban–rural) are somewhat predictive of adoption (R2 = 0.123).
Qualitative findings revealed that decisions to adopt or abandon latrines are multifaceted, with rationale portending to issues of purity, pollution, space, as well as economics, latrine quality, and culture writ large. Qualitative data surface several interesting dynamics. First, two rationale (hygiene, purity, and “naturalness” and convenience and comfort) were reported by both adopters and nonadopters, demonstrating that issues that intersect with health, culture, and behavior are not black and white but in fact interpreted very differently among individuals who reside in the same socio-geographical context. Second, the intersection of latrines with religion and culture is extremely complex in Nagapattinam and Karaikal. Hindu and dominant cultural conceptualizations of purity dictate that bodily fluids are inherently profane, creating a formidable barrier to latrine adoption. Other deterrents include costs associated with pumping septic tanks, resistance to sharing sanitation infrastructure, and tradeoffs due to spatial constraints. Houses provided to families after the tsunami are small, leaving little space to satisfy domestic and cultural functions. Given scarcity of space, the impurity of latrines, and the fact that individuals have historically practiced OD, latrine space is extremely valuable and was sometimes converted to other beneficial uses (e.g., water and firewood storage, puja room, and goat pen). These semiotic and spatio-cultural dimensions of latrine adoption should be of interest to scholars focusing on human ecology of the built environment and practitioners involved in infrastructure development and behavior change.
To inform future aid for sanitation, a starting point is to relinquish preconceived notions on where or among who latrine adoption will be greatest. Rather, adoption can be fostered by harnessing a holistic view of the people, place, and infrastructure in a way that considers their multiple overlaps. For example, latrine introduction may be more successful if the latrine is detached from the household. Further, economic costs of pumping septic tanks should be considered beforehand, especially when costs do not align with the income level of beneficiaries. In such cases, infrastructure based on leach pits or ecological sanitation may be more appropriate, yet these methods present their own set of environmental and socio-cultural barriers. Next, community cohesion and capacity should be gauged prior to implementing shared sanitation infrastructure, which may unintentionally create conflict between latrine users and nonusers. Finally, it is important to recognize that latrine adoption is about changing behavior, which often requires changing culture. Thus, it is essential to perceive sanitation as part of a larger meta-structure in which latrine introduction and sensitization must harmoniously operate.
References
Banda K, Sarkar R, Gopal S, Govindarajan J, Harijan BB, Jeyakumar MB, Mitta P, Sadanala ME, Selwyn T, Suresh CR, Thomas VA, Devadason P, Kumar R, Selvapandian D, Kang G, Balraj V (2007) Water handling, sanitation and defecation practices in rural southern India: a knowledge, attitudes and practices study. Trans R Soc Trop Med Hyg 101(11):1124–1130
Barnard A, Spencer J (eds) (2002) Pollution and purity. In Encyclopedia of social and cultural anthropology. Routledge, New York, NY
Barnard S, Routray P, Majorin F, Peletz R, Boisson S, Sinha A, Clasen T (2013) Impact of Indian Total Sanitation Campaign on latrine coverage and use: a cross-sectional study in Orissa three years following programme implementation. PLoS ONE 8(8):e71428
Bartram J, Cairncross S (2010) Hygiene, sanitation and water: forgotten foundations of health. PLoS Med 7(11):e1000367. https://doi.org/10.1371/journal.pmed.1000367
Baxter J, Eyles J (1997) Evaluating qualitative research in social geography: establishing ‘rigour’ in interview analysis. Trans Inst Br Geogr 22(4):505–525
Bouabid A, Louis GE (2015) Capacity factor analysis for evaluating water and sanitation infrastructure choices for developing communities. J Environ Manag 161:335–343
Caruso, BA, TF Clasen, C Hadley, KM Yount, R Haardorfer, M Rout, M Dasmohapatra, HLF Cooper (2017) Understanding and defining sanitation insecurity: women’s gendered experiences of urination, defecation and menstruation in rural Odisha, India. BMJ Global Health 2. https://doi.org/10.1136/bmjgh-2017-000414
Coffey D, Gupta A, Hathi P, Khurana N, Spears D, Srivastav N, Vyas S (2014) Revealed preference for open defecation: evidence from a new survey in rural North India. Econ Political Wkly 49(38):43–55
Coffey D, Spears D (2017) Where India goes: abandoned toilets, stunted development and the costs of caste. Harper Collins, Noida
Crampton JW, Elden S (2006) Space, politics, calculation: an introduction. Soc Cult Geogr 7(5):681–685
Deilami K, Hayes JF, McGree J, Goonetilleke A (2017) Application of landscape epidemiology to assess potential public health risk due to poor sanitation. J Environ Manag 192:124–133
Dickinson KL, Patil SR, Pattanayak SK, Poulos C, Yang J (2015) Natures call: impact of sanitation choices in Orissa, India. Econ Dev Cult Change 64(1):1–29
Doron A, Raja I (2015) The cultural politics of shit: class, gender and public space in India. Post Stud 18(2):189–207
Dyson T, Moore M (1983) On kinship structure, female autonomy, and demographic behavior in India. Popul Dev Rev 9(1):35–60
Epstein TS (1962) Economic development and social change in South India. Oxford University Press, Bombay
Freeman MC, Garn JV, Sclar GD, Boisson S, Medlicott K, Alexander KT, Penakalapati G, Anderson D, Mahtani AG, Grimes JET, Rehfuess EA, Clasen TF (2017) The impact of sanitation on infectious disease and nutritional status: a systematic review and meta-analysis. Int J Hyg Environ Health 220(6):928–949
Fuller JA, Clasen T, Heijnen M, Eisenberg JNS (2014) Shared sanitation and the prevalence of diarrhea in young children: evidence from 51 countries, 2001–2011. Am J Trop Med Hyg 91(1):173–180
Government of India (2018) Sanitation behaviour change. Ministry of Drinking Water and Sanitation, New Delhi
Government of Pondicherry (GoP) (2005) G.O.Ms.No. 29 Revenue department – relief and rehabilitation – policy on reconstruction of permanent houses and infrastructure facilities for the tsunami affected people – participation of NGOs/voluntary agencies, etc. 15 March 2005. Revenue Department, Government of Pondicherry
Government of Tamil Nadu (GoTN) (2005) Guidelines for evaluation of NGO’s/other agencies to be followed by District Collectors as per G.O.Ms.No. 25 NC(iii) Dept. 13 Jan. 2005. Government of Tamil Nadu
Gupta A, Coffey D, Spears D (2016) Purity, pollution, and untouchability: challenges affecting the adoption, use, and sustainability of sanitation programmes in rural India. In: Bongartz P, Vernon N, Fox J (eds) In Sustainable sanitation for all: experiences, challenges, and innovations. Practical Action Publishing, Rugby, p 283–298
Heijnen M, Routray P, Torondel B, Clasen T (2015) Shared sanitation versus individual household latrines in urban slums: a cross-sectional study in Orissa, India. Am J Trop Med Hyg 93(2):263–268
Hirve S, Lele P, Sundaram N, Chavan U, Weiss M, Steinmann P, Juvekar S (2015) Psychosocial stress associated with sanitation practices: experiences of women in a rural community in India. J Water Sanit Hyg Dev 5(1):115–126
Hulland K, Martin N, Dreibelbis R, Valliant JD, Winch P (2015) What factors affect sustained adoption of safe water, hygiene and sanitation technologies? A systematic review of literature. EPPI-Centre, University College of London, London
Jewitt S (2011) Geographies of shit: spatial and temporal variations in attitudes towards human waste. Prog Hum Geogr 35(5):608–626
Jewitt S, Mahanta A, Gaur K (2018) Sanitation sustainability, seasonality and stacking: improved facilities for how long, where and whom? Geogr J 184(3):255–268
Jha PK (2003) Health and social benefits from improving community hygiene and sanitation: an Indian experience. Int J Environ Health Res 13(S1):S133–S140
Juran L, Lahiri-Dutt K (2017) Waterscapes in transition: changing uses and perceptions of water in middle class homes in Kolkata, India. Water Hist 9(4):433–451
Katz E (1961) The social itinerary of technical change: two studies on the diffusion of innovation. Hum Organ 20(2):70–82
Khanna T, Das M (2015) Why gender matters in the solution towards safe sanitation? Reflections from rural India. Glob Public Health 11(10):1185–1210
KPMG (2018) The making of “Swachh” India: lessons from the Swachh Bharat Mission – driving behavior change at scale. KPMG in India
Ludwig HF, Browder G (1992) Appropriate water supply and sanitation technology for developing countries in tropical monsoon climates. Environmentalist 12(2):131–139
Macpherson H (2016) Walking methods in landscape research: moving bodies, spaces of disclosure and rapport. Landsc Res 41(4):425–432
McMichael C (2018) Toilet talk: eliminating open defecation and improved sanitation in Nepal. Med Anthropol 37(4):294–310
McMichael C, Robinson P (2016) Drivers of sustained hygiene behavior change: a case study from mid-western Nepal. Soc Sci Med 163:28–36
Montgomery MA, Bartram J, Elimelech M (2009) Increasing functional sustainability of water and sanitation supplies in rural Sub-Saharan Africa. Environ Eng Sci 26(5):1017–1023
Nelder, JA and RJ Baker (2006) Generalized linear models. In Encyclopedia of statistical sciences, S Kotz, CB Read, N Balakrishnan, B Vidakovic, and NL Johnson (eds.). https://doi.org/10.1002/0471667196.ess0866.pub2
O’Reilly K (2006) “Traditional” women, “modern” water: linking gender and commodification in Rajasthan, India. Geoforum 37(6):958–972
O’Reilly K (2012) Geography matters: the importance of land, water and space in sanitation studies. wH2O. J Gend Water 1(1):8–9
O’Reilly K, Dhanju R, Louis E (2017) Subjected to sanitation: caste relations and sanitation adoption in rural Tamil Nadu. J Dev Stud 53(11):1915–1928
O’Reilly K, Louis E (2014) The toilet tripod: understanding successful sanitation in rural India. Health Place 29:43–51
O’Reilly K, Louis E, Thomas EA, Sinha A (2016) Combining sensors and ethnography to evaluate latrine use in India. In: Thomas EA (ed.) Broken pumps and promises: incentivizing impact in environmental health. Springer, Heidelberg, p 195–209
Paterson C, Mara D, Curtis T (2007) Pro-poor sanitation technologies. Geoforum 38:901–907
Pattanayak SK, Yang J, Dickinson KL, Patil SR, Paharaj P, Poulos C (2007) Promoting latrine use: ‘midline’ findings from a randomized evaluation of a community mobilization campaign in Bhadrak, Orissa. Working Paper 07-02. Research Triangle Institute, Durham
Pattanayak SK, Yang J, Dickinson KL, Poulos C, Patil SR, Mallick R, Blitstein J, Praharaj P (2009) Shame or subsidy revisited: randomized evaluation of social mobilization for sanitation in Orissa, India. Bull WHO 87(8):580–587
Patil SR, Arnold BF, Salvatore AL, Briceno B, Ganguly S, Colford Jr. JM, Gertler PJ (2013) The effect of India’s Total Sanitation Campaign on defecation behaviors and child health in rural Madhya Pradesh: a cluster randomized controlled trial. PLoS Med 11(8):e1001709
Rashid M, Pandit D (2018) Determination of appropriate service delivery level for quantitative attributes of household toilets in rural settlements of India from users’ perspective. Environ Manag 61(4):637–649
Reckwitz A (2002) Toward a theory of social practices: a development in culturalist theorizing. J Soc Theory 5(2):243–263
Rogers EM (2003) Diffusion of innovations, fifth edition. Free Press, New York, NY
Routray P, Schmidt W-P, Boisson S, Clasen T, Jenkins MW (2015) Socio-cultural and behavioural factors constraining latrine adoption in rural coastal Odisha: an exploratory qualitative study. BMC Public Health 15:880. https://doi.org/10.1186/s12889-015-2206-3
Sarkar B (2008) A practical approach to Vaastu Shastra. Peacock Books, New Delhi
Spears D, Ghosh A, Cumming O (2013) Open defecation and childhood stunting in India: an ecological analysis of new data from 112 districts. PLoS ONE 8(9):e73784. https://doi.org/10.1371/journal.pone.0073784
Srinivas T (2002) Flush with success: bathing, defecation, worship, and social change in South India. Space Cult 5(4):368–386
Tagat A, Kapoor H (2018) ‘Sacred nudging’ and sanitation decisions in India. India Rev 17(3):301–319
The Hindu (2016) Open defecation still a scourge in Nagapattinam. 26 Dec 2016
The Hindu (2017) Tsunami houses: free, but at what cost? 21 Dec 2017
Torras M, Boyce JK (1998) Income, inequality, and pollution: a reassessment of the environment Kuznets Curve. Ecol Econ 25(2):147–160
Tumwine J, Thompson J, Katui-Katua M, Mujwahuzi M, Johnstone N, Porras I (2003) Sanitation and hygiene in urban and rural households in East Africa. Int J Environ Health Res 13(2):107–115
United Nations General Assembly (UNGA) (2010) Resolution adopted by the General Assembly on 28 July 2010: A/RES/64/292 - the human right to water and sanitation. Agenda item 48, 64th session of the United Nations General Assembly (3 Aug 2010). UNGA, New York, NY, USA
World Bank. 2017. “Improved sanitation facilities (% of population with access).” World Bank Open Data. Available at https://data.worldbank.org/indicator/SH.STA.ACSN
World Health Organization and United Nations Children’s Fund (WHO/UNICEF) (2017) Progress on drinking water, sanitation and hygiene: 2017 update and SDG baselines. WHO and UNICEF, Geneva
Yogananth N, Bhatnagar T (2018) Prevalence of open defecation among households with toilets and associated factors in rural south India: an analytical cross-sectional study. Trans R Soc Trop Med Hyg 112(7):349–360
Acknowledgements
Thanks for support from Sanam Aksha and the Laboratory for Interdisciplinary Statistical Analysis (LISA) at Virginia Tech.
Funding
Sustainable Water Undergraduate Research Fellowship from the Virginia Water Resources Research Center (VWRRC), and a New Investigator Award from the National Aeronautics and Space Administration (NASA) and Virginia Space Grant Consortium (VSGC).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Juran, L., Adams, E.A. & Prajapati, S. Purity, Pollution, and Space: Barriers to Latrine Adoption in Post-disaster India. Environmental Management 64, 456–469 (2019). https://doi.org/10.1007/s00267-019-01202-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00267-019-01202-6