
Abstract
Defining the ideal dimensions and proportions of the human face has been attempted for centuries, popularised in the Renaissance period by artists including Leonardo Da Vinci. The lips are part of the lower third of the face and are central to lower face aesthetics and the overall symmetry of the face. They also place an important part in conveying facial emotions and expressions. Full lips with well-defined Cupid’s bow have always been associated with youth and beauty. The approval of hyaluronic acid use for tissue augmentation and the prevalence of social media have caused an exponential increase in lip augmentation procedures (Linkov et al. in Arch Plast Surg 46(3):248–254, 2019), as such researchers and aestheticians have focused on characterising the ideal lips mathematically to help guide clinicians. This narrative review will summarise the available evidence in the literature pertaining to the ideal lips, taking into account age, ethnicity and gender differences.
Level of Evidence III
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Facial aesthetics involves the analysis of individual components of the face. The concept of facial aesthetics dates as far back as the Ancient Greek times [2]. Humans have long tried to characterise beauty through various rules and canons. Symmetry and harmony are considered to be attractive [3]. The lips occupy the lower third of the face and play an important role in determining the overall aesthetic perception of the face; they are also essential in conveying facial expressions and emotions, an integral part of everyday life. Cosmetic surgery to modify and enhance the lips has been gaining popularity in recent years (4). Because of this, numerous studies have attempted to characterise the ideal lips in order to guide treatment. This narrative review aims to examine the current evidence in the literature pertaining to the ideal lips, taking into account ethnic, gender and age differences. The author also discusses how these potential influencing factors should be taken into consideration when planning lip procedures.
Horizontal Thirds
In his publications on the human anatomy, Da Vinci divided the face into equal horizontal thirds. The upper third extends from the trichion (midline of the hairline) to the glabella (region between the eyebrows); the middle third measures from the glabella to the subnasale (where the nasal septum meets the upper white lip); and the lower third extends from the subnasale to the menton/gnathion (the most inferior point of the chin) (Fig. 1). These are considered to be the ‘ideal’ facial proportions. In reality, the facial thirds are rarely equal in height. The relative height of the horizontal thirds is known to show ethnic variations. In East Asians, the middle third is often larger than the upper third [5]. In Caucasians, the lower third is larger than the upper and middle thirds [6]. As the lips occupy much of the lower third of the face, the height of the lower third has important implications for the size and dimensions of the ideal lips for that particular face. The lower third of the face can be split further into horizontal thirds. The upper third is the upper lip, extending from the subnasale to the stomion, and the middle third is the lower lip, extending from the stomion to the labiomental crease. Lastly, the lower third corresponds to the soft tissue chin, extending from the labiomental crease to the gnathion (Fig. 2).

Facial horizontal thirds according to Da Vinci

The lower third of the face divided into further thirds
Vertical Fifths
According to Da Vinci’s drawings, the ideal mouth or lip width should occupy the central fifth of the face (Fig. 3). To the best of the author’s knowledge, no studies to date have corroborated or refuted the applicability of this canon. One study proposed that the ideal lip width is the equivalent of four iris diameters [7].

Facial vertical fifths according to Da Vinci
Anatomy and Landmarks of the Lips
The upper lip encompasses the region bordered by the base of the nose, the two nasolabial folds laterally and the inferior border of the upper vermillion lip. The upper lip describes both the white upper lip and the vermillion (pink) lip. Cupid’s bow constitutes two paramedian elevations in the upper vermillion lip. The philtral columns are two vertical raised columns on either side of the midline within the white upper lip; the philtral dimple sits between the philtral columns. In some individuals, congenital causes or iatrogenic lip augmentation can result in loss of definition of the philtral columns, which can be corrected using dermal fillers. The lower lip extends from the superior free edge of the lower vermillion lip to the oral commissures laterally and the labiomental crease (Fig. 4). The labiomental crease is an inverted U-shaped crease across the chin, which corresponds to the gingivolabial crease intraorally [8]. Through the use of synthetic morph frontal digital images of young Caucasian women, the most attractive lip surface area was found to be 9.5% of the lower third of the face [9].

The anatomy of the lips
The Golden Ratio
The golden ratio, denoted by the symbol \(\phi\) (phi), is a naturally occurring irrational number where a/b = (a + b)/a. It is also known as the Fibonacci ratio or the ‘divine proportions’. The ratio is widely found in nature and art; it has also been applied in facial aesthetics [10]. It has been suggested that our brains naturally perceive proportions obeying the golden ratio as attractive. Indeed, functional magnetic resonance imaging (fMRI) has shown that attractive facial proportions evoke a neural response in the reward regions of the brain [11].
The golden ratio has been used to describe a number of facial proportions pertaining to the lips. The balance of the upper and lower lips is a key determinant of lip attractiveness. It is widely accepted that the lower vermillion lips should be fuller than the upper vermillion lips; the ideal ratio of upper to lower lips should conform to a golden ratio of 1:1.6 [12]. In a study of 18–25-year-old Caucasian women, it was found that an upper to lower lip ratio of 1:2 was considered the most attractive, in support of the golden ratio [9]. On lateral view, if a straight line is drawn from the subnasion to the pogonion (the most anterior point of the chin on lateral view), the upper lip should protrude 3.5 mm beyond the line, and the lower lips 2.2 mm (Fig. 5) [13]. This works out to be a ratio of 1.6:1, again conforming to the golden ratio.

The golden ratio of the upper and lower lips in profile view
Despite the rule, one should bear in mind the natural ethnic differences. Wong et al. [14] compared lip parameters in Caucasians, Korean-Americans and Chinese-Americans. They found that Chinese women had a mean upper to lower lip ratio of 1:1.25, and Korean women had a ratio of 1:1.11. Caucasian women had the thinnest upper lips in comparison, with a ratio of 1:1.43. Unsurprisingly, there are ethnic differences in lip size preferences. In a survey of laypersons, it appears that Asian people prefer smaller lips than their Caucasian counterparts , whilst Hispanics prefer larger lips [15]. African-American people naturally have fuller lips on frontal and profile views; studies have demonstrated that they also prefer lips that are more protrusive on profile view compared to Hispanics and Japanese counterparts [16].
Nasolabial Angle
The nasolabial angle is defined as the angle between the columella and a line intersecting the subnasale and labrale superius (the most anterior point of the upper lips) [19] (Fig. 6). It is a crucial aspect of facial attractiveness on profile view. It is dependent not only on the protrusiveness of the lips, but also on the position and shape of the nasal tip. One group has reported the ideal nasolabial angle to be 93.4°–98.5° in men and 95.5°–100.1° in women as rated by the general population [20], which is comparative to the values of 93.9°–97.3° in men and 96.8°–100.2° in women as judged by rhinoplasty surgeons [21].

Nasolabial angle
Labiomental Angle
The labiomental angle forms the transition from the lower lip to the soft tissue chin. It is the angle formed by a tangent from the sublabiale to the labrale inferius (the most anterior point of the lower lips) and a tangent from the sublabiale to the soft tissue pogonion (most prominent midline point of the soft tissue chin) (Fig. 7). It is one of the most important points of the facial profile as an observer’s perception of the lower face is often draw to this region [22]. It has been suggested that a labiomental angle of approximately 107°–118° is the most appealing [23]. As with the nasolabial angle, there are two determinants of the labiomental angle—the lips and the chin. Although the chin projection plays a more dominant role in determining this angle, it is still worth considering when assessing a patient for lip fillers. If a patient has a chin that is short in the sagittal plane and retrusive in profile, having more prominent lips will exaggerate the weak chin. Even if the lips on their own look aesthetically pleasing, they may not improve the overall appearance of the face due to the imbalance in facial proportions. Patients that seek lip fillers may benefit from a concomitant genioplasty to improve the overall proportions of the lower face. The size of the lips and their fullness in profile should be considered in relation to chin retrusion or prominence. A greater degree of lip protrusion is more acceptable when either a large nose or chin is present [24], highlighting the relevance of the nasolabial and labiomental angles in lip aesthetics.

Labiomental angle
Age Differences
With aging, there is progressive flattening and lengthening of the philtrum. Concomitantly, there is a loss of protrusion of the upper lips, inversion of the vermillion and loss of Cupid’s bow [25]. Studies have reported a significant elongation of the lip, causing a redistribution between lip length (which increases) and the vermillion height (which decreases) [26, 27]. This is an important consideration in lip rejuvenation as arguably, the end result should be aesthetically pleasing but also age-appropriate. When dealing with an older patient, one should be conscious of the natural effects of aging on their lips ad philtrum and avoid over-correction, which can lead to unnatural results.
Gender Differences
The neoclassical canon of horizontal thirds was historically used to describe the ideal female face. In a study of Caucasian men and women in their 20s, the absolute height of the lower third of the face, chin length, upper and lower lip height were significantly greater in males than in females. Interestingly, the vermillion lip heights were not significantly different between the sexes. In both genders, the lower vermillion height was greater than the upper vermillion height, consistent with conventional views in facial aesthetics. However, women had comparatively larger upper vermillion lips, greater lower lip height relative to the chin height and the lower third of the face when compared to men [28]. This reflects that in general, and in the contemporary ideal, the average female face is smaller and shorter than the male face [4]. The same study disputed the neoclassical canon whereby the lower third of the face should be divided into three more equal thirds occupied by the upper lips, lower lips and chin. In both sexes, the lower lips occupied less than one-third, the upper lips approximately one-third and the chin just over one-third (39.7–40.3%). The aesthetic trend is for lip augmentation in women but not in men as fuller lips produce a feminising look and women prefer fuller lips than men [29]. This trend may be a reflection of preference for evolutionary sexual dimorphism.
There is also a sexual difference in the effects of aging on the lips. Men are more resistant to developing rhytids of the lips due to the presence of thicker skin and more subcutaneous fat surrounding the terminal hair follicles [30].
Ethnic Differences
As mentioned above ideal upper to lower lip vermillion ratio of 1:1.6 is generally described with regard to the ideal lips in a Caucasian women, who have comparatively the thinnest upper lips of all ethnicities [31]. Chinese and Korean women have a mean lip ratio of 1:1.25 and 1:1.11 and have fuller lips in general [14, 32]. To reflect the natural discrepancies in lip thickness, the absolute measurement of attractive lips has shown to be different. A thickness of 6.0 mm and 14.6 mm for the upper and lower vermillion lips has been proposed to be attractive in Caucasian female faces, whilst measurements of 6.3 mm and 13.9 mm were proposed to be attractive in Asian females, suggesting that for Asian faces, a more even upper and lower vermillion thickness is considered to be more attractive, and thus does not follow the Vitruvian thirds theory nor the golden ratio [32]. People of Afro-Caribbean origin tend to have the greatest lip volume compared to any other ethnic group. Because of the protective effect of increased melanin in their skin, they are less prone to developing fine lines in and around the lip; their vermillion lips tend to retain volume even with aging [33]. In contrast, Caucasian lips are more prone to the effects of aging. Bone resorption and loss of fat pads result in loss of structural support for the lower face, and the oral commissures turn downwards with a reduction in vermillion volume [26].
In a cross-cultural analysis, it was found that plastic surgeons that practice in Asia and the Middle East preferred the largest lips, followed by those that practised in Latin America. Surgeons in Europe preferred the smallest lips. The ethnicity of the surgeon also impacted on lip size preference. Non-Caucasian surgeons preferred larger lips compared to their Caucasian counterparts. Interestingly the surgeons’ preferences differed from that of the general public. Those living in Latin America reported a preference for the largest lips followed by those living in America and Europe. Laypeople living in Asia preferred the smallest lips [15].
The Ideal Lips as Portrayed in the Media
The studies so far have used photographs of laypersons, but it is interesting to consider whether there are differences in the lips of people represented in the media compared laypersons. One group compared the photographs of models from fashion magazines with of hospital employees. They found that although lip width was not significantly different between the two groups, both upper and lower lip height were significantly greater in models compared to non-models. The preference for fuller lips in models was also reflected in the greater upper lip height at the point of the angle of cupid’s bow and laterally at the angles of the upper and lower lips [34]. The assumption made by the study was that models have aesthetically beautiful lips; the results though do seem to reflect the overall preference for fuller lips in the current aesthetic landscape. Although this study has not been corroborated, similar studies using photographs of models and actresses from the past and in the future may yield information on how the trend for lip aesthetics has changed over the years.
Contemporary Ideals
Whilst there are many rules and canons used in facial aesthetics, beauty is an ever-evolving concept that is subject to trends. It has been observed with noses and eyebrows that the preferred ideal has changed over time [35, 36]. Heidekrueger and colleagues in a survey across 35 countries found that 60% of the survey takers reported a 1:1 lip ratio as the most attractive in women, a distinct difference from the golden ratio [37]. The authors suggested that despite inter-cultural differences, there may be a ratio of upper to lower lip which appears pleasing across most cultural and geographical locations. In the same study, older participants preferred smaller lower lips, whilst younger participants preferred larger ones, mirroring the natural progression of volume loss as one ages. There has been no change in the lower third facial ratio for 2500 years. For both men and women, the stomion to gnathion distance should be approximately 70% of the subnasale to gnathion distance, which conforms to the rule of thirds [38].
Studies have disputed the applicability of the golden ratio in lip aesthetics in modern times. A review of photographs of Miss universe and Miss Universe Thailand found that they have thinner lower to upper lip height ratio than the golden ratio; the authors argued that golden facial ratios are invalid in modern perception of beauty [10]. This has been backed up by Pallett and colleagues, whom through their experiments using female Caucasian faces found that average length and width ratios for the face are optimally attractive [2]. This may be due to influences from evolutionary process [39] and cognitive process [40].
Consideration in Lip Augmentation and Rejuvenation
Before carrying out any procedure, the natural asymmetry of the lips should be noted and the client informed. Lip augmentation can enhance the degree of asymmetry if treatment is not planned carefully. Many practitioners will attempt to compensate for the natural asymmetry by injecting a slightly greater volume of filler into the smaller side [41]. There are no fatty tissues in the lips; hence, hyaluronic acid fillers can be injected at either surface level (mid-dermal) or deeper down (submucosal level), above the orbicularis oris muscle. Filler use for lip treatment can be broadly speaking divided three separate areas with different desired outcomes.
-
Injection into the philtral columns can enhance definition and be used to achieve an apparent reduction in the perceived length.
-
Injection along the vermillion border can be used to give better definition of the lips on frontal view. It can be used to evert the lip border, improving the labial profile view.
-
Injections into the body of the vermillion lips are used to augment the overall volume of the lips and can be achieved using a needle (retrograde linear or serial puncture) or a cannula technique. Injections should stop medial to the oral commissures to avoid ‘duck lip’ appearance. These injections should be placed deep.
In older patients, peri-oral lines are recommended to be treated simultaneously through the use of fillers and/or botulinum toxin. The greater degree of atrophy in the lips, the greater risk of an unnatural result. The author recommends the use of softer fillers in the lips of older patients to avoid unnatural results.
In younger patients, sometimes a lack of fullness in the lips is due to elongation and flattening of the philtral columns rather than the fact that the vermillion lips themselves are very thin. Superficial injections using the retrograde linear technique can be placed into the philtral columns and the vermillion border to produce more eversion of the upper lips and shortening the philtrum [42].
The lips should be injected from right to centre and left to centre. It is desirable to stretch the lips as it is being injected to ensure the injection starts near the end of the lip; a firm surface helps to improve the uniformity of distribution of filler material. The needle should be introduced at 45° into the potential vermillion space and then redirected to a 20° angle. A low and steady injection technique again helps to distribute the filler evenly within this potential space [43].
The patient’s ethnicity and country of residence should be taken into consideration when planning treatment. Hispanics have naturally larger lips and prefer larger lips [31]. Asian laypersons prefer smaller lips, whilst surgeons in Asia prefer the largest lips [37]. This discrepancy is curious but highlights that a surgeon’s concept of ideal lip may not be the same as that of the patient. They should not let their preference and opinion guide the treatment alone. The author proposes that although there is not a universally applicable ideal lip, awareness of lip size preference based on ethnicity is a useful starting point for guiding treatment. Afro-Caribbean and Hispanics prefer the largest lips, followed by Caucasians and Asians.
The peri-oral region as a whole should be taken into consideration. In profile view, the lips should be in balance against the nose and chin. Penna and colleagues [44] found that the labiomental angle was wider in attractive females compared to non-attractive ones. With aging, the mentalis muscle becomes more active, deepening labiomental crease and shortening the chin. Botulinum toxin injection into the muscle will counteract this and widen the labiomental angle [45].
Autologous Fat Grafting
The transfer of autologous fat has been performed since the 1890s [46]. The concept of lipostructure was developed by Coleman [47,48,49]. Autologous fat transfer has been used as a technique in facial recontouring and enhancement for both cosmetic and reconstructive purposes [50]. It has been particularly useful in the context of lip reconstruction in those with cleft lip repairs [51]. Lipostructure allows tissues to be sculpted into the desired three-dimensional shape; it has the advantages of being completely biocompatible and integrates into local host tissues. Utilisation of autologous fat removes the possibility of allergy, rejection and extrusion. However, attention is required as fatty tissues are delicate structures that are easily damaged by mechanical and chemical insults. Careful consideration is required for the method of harvesting, transfer and the eventual placement of the fat. Fatty tissues are living tissues that need nutrition to survive. Therefore, placement of small amounts of fat in multiple tunnels assumes the utmost importance in the quest for graft uptake and survival as well as the optimal aesthetic outcome [47]. Autologous fat transfer is expensive but can be an appealing option for patients given its biocompatible nature. The longevity of the results is hugely variable and often short-lived; for more sustained results, repeated treatments are required [52]. Whilst the need for serial treatments can be likened to hyaluronic acid (HA) fillers, autologous fat graft entails the additional process of harvesting and refining the graft, adding to the cost; despite this, the downtime from the procedure is still fairly minimal. Compared to HA fillers, the results can be more variable with fat grafts as the graft take and survival depends on the harvest technique and depth of injection. It has been suggested that autologous fat when combined with allogenic dermal graft gives a longer-lasting increase in vermillion show and lateral lip projection when compared to autologous fat injection alone [53]. There can be undesirable side effects such as fat tissue accumulation leading to submucosal enlargement [54]. It has also been argued that free fat grafts are less effective in enhancing the vermillion border than the body of the lip, possibly due to the thinness of the orbicularis oris muscle in the vermillion border and the relative hypermobility of the region [55]. In the author’s opinion, fat grafts can be used in a selective group of patients that have well-defined vermillion borders that do not need further enhancement and have a preference for using autologous material and/or are particularly against or intolerant of HA fillers. They should probably not be the procedure of choice in most given the reliability of other options. The modern HA fillers used have excellent tissue integration and allow enhancement and eversion of the vermillion borders, all of which make them the treatment of choice for most clients.
Expanded Polytetrafluoroethylene
Expanded tetrafluoroethylene was first introduced in 1997 as a soft-tissue filling substance [56] and has been used to achieve correction of deep nasolabial folds as well as lip augmentation [57]. Like liquid silicone, the literature has reported a serious of deleterious side effects associated with its use, the commonest of which include migration extrusion infection, shrinkage and granulomatous foreign body reaction [58,59,60] .
Silicone Implants
Silicone implants are a relatively new method for lip augmentation, most commonly in the cosmetic setting, although the use of silicone implants in adult patients with a history of cleft lip repairs has been reported, with success in enhancing upper vermillion lip volume [61]. There are a variety of silicone implants available, such as injectable liquid silicone and PermaLip ImplantTM. The complications of liquid silicone include granuloma formation, beading and migration [62], and the numerous reports of complications associated with the use of liquid silicone have led to many opponents of its use [63]. PermaLip ImplantTM appears to be superior to liquid silicone and has fewer complications [64]. Certainly, multiple groups have reported its successful use with good patient satisfaction [64, 65]. The permanent nature of silicone implants and reversibility via surgical removal is major advantages. When compared to expanded polytetrafluoroethylene, silicone implants have a lower risk of capsular contraction as its non-porous surface is able to resist tissue ingrowth [64]. It can be argued that a permanent filler would be more cost-effective for the patient in the long term, provided that there are no major complications requiring revision. HA fillers and autologous fat grafts can both be expensive as repeated sessions are needed to maintain results. HA fillers tend to produce more reproducible results than fat transplant but still last a variable duration depending on the choice of product used and the patient. Serial treatment with HA fillers can lead to undesirable collagen deposition [64]. Silicone implants can be a successful one-off procedure in experienced hands, but are hard to use in razor-thin lips. Another disadvantage is that they cannot be used to correct asymmetries of the lip. In contrast, HA fillers can be used to correct the underlying asymmetry of the lips to a certain degree. There is also an issue with graft palpability and visibility when smiling with non-autologous grafts, and even though the implant can be reversed through removal, there is always the risk of scarring and causing asymmetry of the lips [66].
In the author’s opinion and with the current evidence, HA fillers are the optimal lip filler of choice for most patients, with virtually no downtime and natural reversibility should suboptimal results occur. Silicone implants may be useful in those seeking a one-off permanent solution, with naturally reasonable labial height. Of note, the procedure should be carried out by experienced surgeons to reduce the need for resizing of fillers and other complications.
Minimally Invasive Procedures
V--Y lip lift
V–Y lip lift, or the V to Y lip advancement, is a relatively new technique; it is most commonly used for upper lip augmentation [67], but its use has also been described in the lower lips [68]. There are various modifications of the V to Y technique, the specific details of which are beyond the scope of this review. However, broadly speaking there are two main techniques. 2 ‘V’ incisions can be placed adjacent to each other intraorally as described by Samian [69] in order to create a ‘W’ with the base of the ‘W’ orientated towards the lip sulcus and the tip towards the vermillion mucosal junction. Alternatively, 2 parallel ‘V’-shaped incisions can be made in the lips to create one smaller triangular unipedicled flap and a larger bipedicled ‘V’ flap [70]. In both techniques, the incisions are closed in a ‘V’ to ‘Y’ fashion, providing lip augmentation. By shortening the buccal surface horizontally, the distance between the oral commissures is reduced and it appears that a remarkable amount of lip protrusion can be produced in this manner. In one quantitative analysis, lip protrusion in profile was estimated to increase by 40% [68]. As it is a more invasive procedure than the injection of HA fillers, there is more postoperative swelling and downtime. However, shape and volume retention at 2 years appear satisfactory [70]. The scars are in theory hidden in the V to Y lip lift, and the permanence of results is appealing. However, one should bear in mind that this procedure shortens the horizontal distance between the oral commissures and therefore is unsuitable for those with already short upper lips to avoid imbalance in facial proportions.
Gull Wing/Direct Lip Lift
A direct or gull wing lip lift is used to create a more defined lip border. The technique is older than that of the V to Y lip lift; the first publication on the direct lift was by Meyer and Kesserling in 1976 [71]. The procedure involves excision of the skin at the junction between the pink vermillion lip and the white lip. The vermillion lip is advanced upwards creating a bigger vermillion lip show, and depending on the length of skin excised, it can also be used to elevate the lip corners, making it useful in older patients with natural sagging of the oral commissures. The biggest problem associated with the procedure is the associated scarring as the scars are not hidden, but may be faint and easily concealed with lipstick. In a systematic review examining surgical lip enhancement techniques, the rate of hypertrophic scarring associated with direct lip lift ranged from 3.1% to 27.2% in the literature [72]. Other reported complications associated with direct lip lift include asymmetry requiring revisions [73] and insufficient or under correction [74]. In the author’s opinion, a gull wing lip lift does not significantly alter the overall lip volume. The fact that it shortens and lifts the lips and its ability to lift the oral commissures makes it more suitable for older patients, as their main issues are more likely to be elongation of the vermillion lip and sagging of the lip corners. They are also less likely to desire a drastic enhancement in lip volume as it would look unnatural. However, with the other modern techniques of lip enhancement available, the risk of unsightly scarring is probably an unnecessary risk to take. Soft HA fillers such as VolbellaTM combined with botulinum Toxin type A can be used to give natural, subtle enhancement of the lips and lifting the oral commissures with no scarring and minimal downtime.
Conclusion
This review has summarised the available evidence in the literature pertaining to the most aesthetically pleasing lip. Full lips have always been associated with youth and beauty; lips are central to the aesthetics of the lower face. There is no universally ideal lip that is applicable to every patient. Consideration of the ethnicity, age and personal preference of the patient should be taken into consideration. Beauty preferences are subject to sociocultural influences and trends; therefore, ideals may only represent a snapshot in time. Continual research and analysis into lip aesthetics will enable those practising in the field to keep up to date with such trends.
References
Linkov G, Wick E, Kallogjeri D, Chen CL, Branham GH (2019) Perception of upper lip augmentation utilizing simulated photography. Arch Plast Surg 46(3):248–254
Pallett PM, Link S, Lee K (2010) New, “Golden” ratios for facial beauty. Visi Res 50(2):149
Enquist M, Arak A (1994) Symmetry, beauty and evolution. Nature 372(6502):169–172
Kar M, Muluk NB, Bafaqeeh SA, Cingi C (2018) Is it possible to define the ideal lips? Acta Otorhinolaryngol Ital. 38(1):67–72
Sim RS, Smith JD, Chan AS (2000) Comparison of the aesthetic facial proportions of southern Chinese and white women. Arch Facial Plast Surg 2(2):113–120
Farkas LG, Hreczko TA, Kolar JC, Munro IR (1985) Vertical and horizontal proportions of the face in young adult North American Caucasians: revision of neoclassical canons. Plast Reconstr Surg. 75(3):328–338
Young P (2019) Assessment of ideal dimensions of the ears, nose, and lip in the circles of prominence theory on facial beauty. JAMA Facial Plast Surg 21(3):199–205
Luthra A (2015) Shaping lips with fillers. J Cutan Aesthet Surg 8(3):139–142
Popenko NA, Tripathi PB, Devcic Z, Karimi K, Osann K, Wong BJF (2017) A Quantitative approach to determining the ideal female lip aesthetic and its effect on facial attractiveness. JAMA Facial Plast Surg 19(4):261–267
Burusapat C, Lekdaeng P (2019) What Is the most beautiful facial proportion in the 21st century? comparative study among Miss Universe, Miss Universe Thailand, Neoclassical Canons, and Facial Golden Ratios. Plast Reconstr Surg Glob Open 7(2): e2044. https://doi.org/10.1097/GOX.0000000000002044
Shen H, Chau DK, Su J, Zeng LL, Jiang W, He J, Fan J, Hu D (2016) Brain responses to facial attractiveness induced by facial proportions: evidence from an fMRI study. Sci Rep. 25(6):35905. https://doi.org/10.1038/srep35905
Bueller H (2018) Ideal facial relationships and goals. Facial Plast Surg. 34(5):458–465
Powell N, Humphreys B (1984) Proportions of the aesthetic face. Thieme-Stratton, Germany, p 104
Wong WW, Davis DG, Camp MC, Gupta SC (2010) J Plast Reconstr Aesthet Surg. 63(12):2032–2039
Heidekrueger PI, Szpalski C, Weichman K, Juran S, Ng R, Claussen C, et al. Lip Attractiveness: A Cross-Cultural Analysis. Aesthet Surg J. 2017 01;37(7):828–836.
Nomura M, Motegi E, Hatch JP, Gakunga PT, Ng’ang’a PM, Rugh JD, et al (2009) Esthetic preferences of European American, Hispanic American, Japanese, and African judges for soft-tissue profiles. Am J Orthod Dentofacial Orthop 135(4 Suppl):S87–95.
Hoefflin SM (2006) The definition of facial beauty. In: Panfilov DE (ed) Aesthetic surgery of the facial mosaic. Springer, Berlin, Heidelberg, pp 43–51
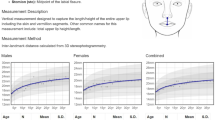
Zankl A, Eberle L, Molinari L, Schinzel A (2002) Growth charts for nose length, nasal protrusion, and philtrum length from birth to 97 years. Am J Med Genet. 111(4):388–391
Harris R, Nagarkar P, Amirlak B (2016) Varied definitions of nasolabial angle: searching for consensus among rhinoplasty surgeons and an algorithm for selecting the ideal method. Plast Reconstr Surg Glob Open 4(6):e752. https://doi.org/10.1097/GOX.0000000000000729
Armijo BS, Brown M, Guyuron B (2012) Defining the ideal nasolabial angle. Plast Reconstr Surg 129(3):759–764
Brown M, Guyuron B (2013) Redefining the ideal nasolabial angle: part 2. Expert analysis. Plast Reconstr Surg 132(2):221e-e225
Rosen HM (1991) Aesthetic refinements in genioplasty: the role of the labiomental fold. Plast Reconstr Surg. 88(5):760–767
Naini FB, Cobourne MT, Garagiola U, McDonald F, Wertheim D (2017) Mentolabial angle and aesthetics: a quantitative investigation of idealized and normative values. Maxillofac Plast Reconstr Surg 39(1):4. https://doi.org/10.1186/s40902-017-0102-8
Czarnecki ST, Nanda RS, Currier GF (1993) Perceptions of a balanced facial profile. Am J Orthod Dentofacial Orthop. 104(2):180–187
Maloney BP (1996) Cosmetic surgery of the lips. Facial Plast Surg. 12(3):265–278
Farkas JP, Pessa JE, Hubbard B, Rohrich RJ (2013) The science and theory behind facial aging. Plast Reconstr Surg Glob Open 1(1):e8–e15. https://doi.org/10.1097/GOX.0b013e31828ed1da
Iblher N, Kloepper J, Penna V, Bartholomae J-P, Stark GB (2008) Changes in the aging upper lip: a photomorphometric and MRI-based study (on a quest to find the right rejuvenation approach). J Plast Reconstr Aesthet Surg. 61(10):1170–1176
Anic-Milosevic S, Mestrovic S, Prlić A, Slaj M (2010) Proportions in the upper lip-lower lip-chin area of the lower face as determined by photogrammetric method. J Craniomaxillofac Surg. 38(2):90–95
Hier LA, Evans CA, BeGole EA, Giddon DB (1999) Comparison of preferences in lip position using computer animated imaging. Angle Orthod 69(3):231–238
Sarnoff DS, Gotkin RH (2012) Six steps to the “perfect” lip. J Drugs Dermatol 11(9):1081–1088
Kollipara R, Walker B, Sturgeon A (2017) Lip Measurements and Preferences in Asians and Hispanics: A Brief Review. J Clin Aesthet Dermatol. 10(11):19–21
Rhee SC (2018) Differences between Caucasian and Asian attractive faces. Skin Res Technol 24(1):73–79
Lemperle G, Anderson R, Knapp TR (2010) An index for quantitative assessment of lip augmentation. Aesthet Surg J 30(3):301–310
Bisson M, Grobbelaar A (2004) The esthetic properties of lips: a comparison of models and nonmodels. Angle Orthod. 74(2):162–166
Ding A, Zhang Y (2020) What is the perfect nose? Lesson learnt from the literature. RHINOL 3(3):25–30
Ding A (2020) The ideal eyebrow: lessons learnt from the literature. Aesthetic Plast Surg. https://doi.org/10.1007/s00266-020-01920-x
Heidekrueger PI, Juran S, Szpalski C, Larcher L, Ng R, Broer PN (2017) The current preferred female lip ratio. J Cranio-Maxillofac Surg 45(5):655–660
Mommaerts MY, Moerenhout BAMML (2011) Ideal proportions in full face front view, contemporary versus antique. J Cranio-Maxillofac Surg 39(2):107–110.
Langlois JH, Roggman LA (1990) Attractive faces are only average. Psychol Sci 1(2):115–121
Rubenstein AJ, Kalakanis L, Langlois JH (1999) Infant preferences for attractive faces: a cognitive explanation. Dev Psychol 35(3):848–855
Spiegel JH, Spiegel OL (2019) Lip lifting: not just fullness—everything you need to know about lifting and creating youthful, beautiful lips. Facial Plast Surg 35(2):129–133
Sito G, Consolini L, Trévidic P (2019) Proposed guide to lip treatment in caucasian women using objective and measurable parameters. Aesthet Surg J 39(12):NP474– NP483
Klein AW (2005) In search of the perfect lip: 2005. Dermatol Surg 31(11 Pt 2):1599–1603
Penna V, Fricke A, Iblher N, Eisenhardt SU, Stark GB (2015) The attractive lip: a photomorphometric analysis. J Plast Reconstr Aesthet Surg 68(7):920–929
Trévidic P, Sykes J, Criollo-Lamilla G (2015) Anatomy of the lower face and botulinum toxin injections. Plast Reconstr Surg 136(5 Suppl):84S-91S
Agrawal KS, Bachhav M, Naik CS, Tanwar H, Sankhe SS (2016) Autologous fat transfer for esthetic contouring of face in posttraumatic nonfunctional maxillofacial deformities. Craniomaxillofac Trauma Reconstr 9(2):113–120
Coleman SR (1997) Facial recontouring with lipostructure. Clin Plast Surg 24(2):347–367
Coleman SR (2006) Facial augmentation with structural fat grafting. Clin Plast Surg 33(4):567–577
Coleman SR (1995) Long-term survival of fat transplants: controlled demonstrations. Aesthetic Plast Surg 19(5):421–425
Mojallal A, Foyatier J-L (2004) Historical review of the use of adipose tissue transfer in plastic and reconstructive surgery. Ann Chir Plast Esthet 49(5):419–425
Sasson DC, Turin SY, Gosain AK (2020) Novel passage of dermis-fat graft for augmentation of vermilion deficiency following cleft lip repair. Cleft Palate Craniofac J 57(7):919–922
Gatti JE (1999) Permanent lip augmentation with serial fat grafting. Ann Plast Surg 42(4):376–380
To WC, Seeley BM, Castor SA, Papay FA (2002) One-year survival of AlloDerm allogenic dermal graft and fat autograft in lip augmentation. Aesthet Surg J 22(4):349–354
Kaminagakura E, Rosa JA, Carvalho YR, Almeida JD (2013) Undesirable effect of cosmetic lip augmentation with autologous fat tissue. BMC Res Notes 5(6):79
Ergün SS, Cek DI, Baloğlu H, Algün Z, Onay H (2001) Why is lip augmentation with autologous fat injection less effective in the vermilion border? Aesthetic Plast Surg 25(5):350–352
Maas CS, Eriksson T, McCalmont T, Mabry D, Cooke D, Schindler R (1998) Evaluation of expanded polytetrafluoroethylene as a soft-tissue filling substance: an analysis of design-related implant behavior using the porcine skin model. Plast Reconstr Surg 101(5):1307–1314
Hanke CW (2002) A new ePTFE soft tissue implant for natural-looking augmentation of lips and wrinkles. Dermatol Surg. 28(10):901–908
Brody HJ (2001) Complications of expanded polytetrafluoroethylene (e-PTFE) facial implant. Dermatol Surg 27(9):792–794
Cox SE (2005) Who is still using expanded polytetrafluoroethylene? Dermatol Surg 31(11 Pt 2):1613–1615
Hubmer MG, Hoffmann C, Popper H, Scharnagl E (1999) Expanded polytetrafluoroethylene threads for lip augmentation induce foreign body granulomatous reaction. Plast Reconstr Surg 103(4):1277–1279
Paddle A, Wordsworth M, Atherton D (2018) Silicone lip implant for augmentation in cleft lip. J Plast Reconstr Aesthet Surg 71(4):546–547
Narins RS, Beer K (2006) Liquid injectable silicone: a review of its history, immunology, technical considerations, complications, and potential. Plast Reconstr Surg 118(3 Suppl):77S-84S
Mercer N (2011) Re: a retrospective study on liquid injectable silicone for lip augmentation: long term results and patient satisfaction. Rony A. Moscona, Lucian Fodor. J Plast Reconstr Aesthet Surg (2010) 63, 1694–1698. J Plast Reconstr Aesthet Surg 64(6):831
Raphael P, Harris R, Harris SW. Five-year Experience with Perma Facial Implant. Plast Reconstr Surg Glob Open. 2014;2(5):e153. Published 2014 Jun 6. https://doi.org/10.1097/GOX.0000000000000091
Guida S, Mandel VD, Farnetani F, Manola CM, Rubino G, Ruzzu S et al (2017) Permanent implants for lip augmentation: results from a retrospective study and presentation of tips and tricks. J Plast Reconstr Aesthet Surg 70(5):699–704
Segall L, Ellis DAF (2007) Therapeutic options for lip augmentation. Facial Plast Surg Clin North Am 15(4):485–490, vii.
Obradovic B, Obradovic M (2015) Triple V–Y vermilion augmentation of the upper lip. J Craniofac Surg 26(8):e736–e738
Jacono AA, Quatela VC (2004) Quantitative analysis of lip appearance after V–Y lip augmentation. Arch Facial Plast Surg 6(3):172–177. https://doi.org/10.1001/archfaci.6.3.172
Samiian MR (1993) Lip augmentation for correction of thin lips. Plast Reconstr Surg 91(1):162–166
Mutaf M (2006) V–Y in V–Y procedure: new technique for augmentation and protrusion of the upper lip. Ann Plast Surg 56(6):605–608
Meyer R, Kesselring UK (1976) Aesthetic surgery in the perioral region. Aesthetic Plast Surg 1(1):61–69
Moragas JSM, Vercruysse HJ, Mommaerts MY (2014) “Non-filling” procedures for lip augmentation: a systematic review of contemporary techniques and their outcomes. J Cranio-Maxillofac Surg 42(6):943–952
Holden PK, Sufyan AS, Perkins SW (2011) Long-term analysis of surgical correction of the senile upper lip. Arch Facial Plast Surg 13(5):332–336
Fanous N (1984) Correction of thin lips: “lip lift.” Plast Reconstr Surg 74(1):33–41
Funding
None to declare.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest to disclose.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
For this type of study informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ding, A. The Ideal Lips: Lessons Learnt from the Literature. Aesth Plast Surg 45, 1520–1530 (2021). https://doi.org/10.1007/s00266-021-02190-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-021-02190-x