
Abstract
Vaginal labiaplasty has become a more frequently performed procedure as a result of the publicity and education possible with the internet. Some of our patients have suffered in silence for years with large, protruding labia minora and the tissue above the clitoris that is disfiguring and uncomfortable and makes intercourse very difficult and painful. We propose four classes of labia protrusion based on size and location: Class 1 is normal, where the labia majora and minora are about equal. Class 2 is the protrusion of the minora beyond the majora. Class 3 includes a clitoral hood. Class 4 is where the large labia minora extends to the perineum. There are two principal means of reconstructing this area. Simple amputation may be possible for Class 2 and Class 4. Class 2 and Class 3 may be treated with a wedge resection and flap advancement that preserves the delicate free edge of the labia minora (Alter, Ann Plast Surg 40:287, 1988). Class 4 may require a combination of both amputation of the clitoral hood and/or perineal extensions and rotation flap advancement over the labia minora.
Level of Evidence V
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Avoid common mistakes on your manuscript.
Introduction
Abnormally protruding labia minora past the labia majora is a well-documented complaint by women for both the aesthetic and the functional problems they cause. These often include insecurity when wearing tight clothing, embarrassment when unclothed, hygiene, dryness, irritation, tearing, and discomfort during sexual intercourse. Consequences of hypertrophy of the labia minora are diminished self-esteem, job security (models), athletic activity, and intimate relationships. Since identification of this concern, several surgical procedures have evolved [1–6].
Previous attempts to describe a classification system for hypertrophy of the labia minora are too vague for surgeons attempting to categorize and define a procedural approach in practice [5]. Techniques for repairing labia minora protrusions have also become varied and complicated, while all are reported to enjoy continued success and satisfaction [1, 2, 4–6].
To avoid confusion in diagnosis and improve reconstructive treatment, we propose a simple standardized classification system that includes the variations encountered by the examining physician, and suggest a reconstructive approach for the operating surgeon.
Classifications
A four-class system is used to describe the possible variations of labia minora protrusion (Table 1).
-
Labia minora that are limited to just the central portion of the introitus and extend to the borders of the labia majora up to a maximum of 2 cm from the fourchette are described as Class 1 (Fig. 1) and considered within normal limits.
Fig. 1 
Class 1 is an extension of the labia minora of 1 or 2 cm above the fourchette. This usually corresponds with approximately the thickness of the labia majora and may, of course, vary with the patient’s weight or habitus. The clitoris has a small hood that may be visible but not protruding excessively. This is within normal limits
-
If the labia minora extends beyond the labia majora and is more than 2 cm from the fourchette, it is Class 2 (Fig. 2).
Fig. 2 
a Class 2 is an extension of the labia minor significantly beyond the labia majora. This may be in the range of 2 cm or as much as 8 cm in length. In Class 2, the clitoris has a small hood that does not extend significantly beyond the labia, which may be visible but does not extend beyond the labia majora. b (left) A Class 2 with a wedge resection, as described by Alter [1], wherein a full-thickness portion of excessive labia is to be removed. c (right) Closure of the created defect, preserving the delicate free edge of the labia with an inconspicuous scar posteriorly
-
When a separate extension of the labia minora tissue extends above the clitoris and is more than 2 cm beyond the labia majora, it is Class 3 (Fig. 3).
Fig. 3 
a Class 3, wherein the labia minora extend well beyond the labia majora, maybe by many centimeters, and the clitoral hood is excessive and extends well beyond the labia majora. b (left) Repair of Class 3 labia minora using the Altar flap and reduction of the clitoral hood c by direct excision. c (right) Repair as described in a
-
In the most extreme circumstances, excess tissue may extend more than 2 cm beyond the clitoral hood and beyond the perineum (Class 4) (Fig. 4).
Fig. 4 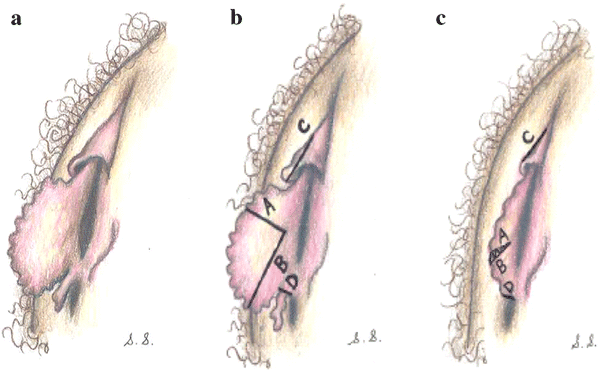
a (left) Class 4 defect. b (center) Line of excision of the labia minora, a flap of labia minor as described by Alter [1]. Lines A, B, and C are direct excisions of the clitoral hood, and D is a direct excision of redundancy of the perineum. c (right) Closure and repair of defect in A




Each class of labia minora protrusion has an appropriate surgical correction procedure.
Materials and Methods
We perform all surgical procedures with the patient under diazepam and ketamine dissociative anesthesia in the interest of patient safety and comfort [7]. Occasionally, for economic reasons, local anesthesia is possible. For a modest correction of Class 1 labia minora (<2-cm protrusion), the protruding tissue of the clitoral hood of Class 3 (Figs. 1, 2, 3, 5, 6), and the perineum of Class 4 (Figs. 8, 9), direct excision is possible. Tissue to be excised is marked to allow a line of resection that leaves 1 cm of labia minora intact and to completely remove the anterior and posterior protrusions of Class 3 and Class 4 cases. Preoperative marking assists evaluation of symmetry in the operating room. A surgical clamp is placed along the lines of resection, is left in place for a few minutes, and then the tissue is excised. The two mucosal surfaces of the remaining labia are then sutured with a running absorbable stitch (5/0 Vicryl) to provide hemostasis and juxtaposition of the edge of these delicate tissues.

Before (a) and after (b) photos of vaginal labioplasty 17-year-old Class 3 patient. She had seen a female plastic surgeon who declined surgery and did not refer her

a A 34-year-old dancer with protruding labia minora. She said that it was an embarrassment when in a bathing suit or tights and especially when nude. b Patient shown after both labia were repaired
When the protrusion of the labia minora extends 2 cm beyond the fourchette, a wedge resection, as described by Alter [1], may be performed. This technique allows for a full-thickness portion of the labia minora to be removed radial to the vaginal opening (Fig. 3). A V-shaped wedge is excised from the most protuberant portion of the labia minora. The incised edges are then approximated leaving a free border of the reduced labia without any exposed scar. This technique enables considerable reduction of the labia while maintaining a natural edge.
Results
We have been in practice since 1978 but have performed vaginal labioplasty for more than 100 patients in just the past 10 years. Most have been pleased with the results. We have never had a case of infection, excessive bleeding, or any other dissatisfaction in patients, who range in age from 16 to 52. There have been no cases of hypertrophic scars, contracture, or hyper- or hyposensitivity. We had one unhappy patient in whom the two lips did not match exactly. They were not visible in repose but she was not pleased with the appearance of the results.
A recent article in Plastic Surgery News suggested that labiaplasty was an effort to distort normal variations to please others or conform to a perception of style; that concept is a mistake. We recently had a patient who had worked for two famous academic plastic surgeons in another city. When she asked about labioplasty for protruding labia minora, they both told her she was within normal limits and ignored her symptoms. Another slim patient was told to by her gynecologist “gain some weight” so the labia majora might increase in size to hide the protruding clitoris and labia minora. Both where pleased with labiaplasty and very disappointed that their other consultants had been so dismissive, even derisive, of their deformity.
Discussion
Women are embarrassed and confused about having external genitalia that do not appear to be normal. Once they discuss this matter, we find that large labia minora are more than just a nuisance. They are painful when girls are simply sitting down because the labia become pinched and pulled. They are embarrassed when wearing tight-fitting clothes or a bathing suite. No one else may notice the protrusion, but they think it is devastating. The labia minora are not particularly sensitive sexually and women report that it is not of any benefit during sexual intercourse or foreplay. At times, the labia may become dry and often develops cracks on the surface (Figs. 7, 8, 9). Women with severe cases report bleeding after intercourse. One of our rhinoplasty patients, a beauty queen, requested labia reduction. She said, “I don’t know how to explain this problem. It is as though you would try to pull your ear across your cheek and put it in your mouth.” Once the excess labia are removed, women are overwhelmingly relieved and happy with the final result (Figs. 7, 8, 9). We have been performing labiaplasty for years but were unaware of how common this problem is until we published a brief paper on the topic [3]. Recently, after posting the paper on our website, a lawyer, who had been a patient for 20 years, requested this reconstruction. She said that she had been suffering her entire life with this problem and had no idea that there was anything that could be done about it. She knew it was abnormal but thought there was no recourse to uncomfortable intercourse. She and her husband thank us repeatedly for this small procedure (Fig. 7).

a A 48-year-old lawyer patient complained that protruding labia minora have contributed to irritation while walking and sitting as well as confidence issues. b After labia excision, patient reported dramatic functional improvement and renewed comfort socially

a A 41-year-old wife and mother. Note the tissue paper remnants. b Two years after single amputation (“clip and snip”)

a A 34-year-old computer engineer and mother with a Class 4 deformity. b Two years after surgery. c Note the natural edge and normal appearance of this “clip and snip” procedure without any noticeable scar
Critics of the single “clip and snip” procedure claim that a scar may form on the amputated free edge. None of our patients have developed such a scar, and none are pictured in the literature. Various flaps may leave the free edge denervated and numb. Simple amputation leaves full innervation to the very edge. Therefore, not only is the “clip and snip” quicker and easier, it may yield a more sensitive structure.
Complications
The only complication in our patient cohort was a woman who was concerned about the symmetry of her labia minora and reported reduced autologous lubrication. Although she had reported difficult lubrication with hypertrophic labia minora, this case indicates the care that must be practiced when evaluating symmetry.
To aid consistency and avoid confusion among physicians, we have developed a simple classification system for evaluating hypertrophic labia minora. While multiple systems have been proposed, confusion persists due to vague criteria and lack of indication for correction of associated categories.
We conclude that vaginal labia reduction is a safe procedure that can be performed on an outpatient basis. This classification system aids in evaluating the degree of deformity and suggests appropriate repair.
References
Alter GJ (1998) A new technique for aesthetic labia minora reduction. Ann Plast Surg 40:287
Choi HY, Kim KT (2000) A new method for aesthetic reduction of labia minora (the deepithelialized reduction of labioplasty). Plast Reconstr Surg 105:419–422
Girling VR, Salisbury M, Ersek RA (2005) Vaginal labioplasty. Plast Recontr Surg 115(6):1792–1793
Rouzier R, Louis-Sylvestre C, Paniel BJ, Haddad B (2000) Hypertrophy of labia minora: experience with 163 reductions. Am J Obstet Gynecol 182:35–40
Pardo J, Sola V, Ricci P, Guilloff E (2006) Laser labioplasty of labia minora. Int J Gynaecol Obstet 93:38–43
Felicio YA (2007) Labial surgery. Aesthet Surg J 27:322–328
Ersek RA (2004) Dissociative anesthesia for safety sake: ketamine and diazepam—a 35 year personal experience. Plast Reconstr Surg 1113(7):1955–1959
Acknowledgments
We would like to thank Eugene Gonzales, Rachel Salas, Jill Niemtschk, Kimberly Hickman, Carmel Kenan, Rebecca Allison, Tori Farnsworth, Priscilla Tambunga and the entire Personique Surgery Center staff for their efforts in the completion of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chang, P., Salisbury, M.A., Narsete, T. et al. Vaginal Labiaplasty: Defense of the Simple “Clip and Snip” and a New Classification System. Aesth Plast Surg 37, 887–891 (2013). https://doi.org/10.1007/s00266-013-0150-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-013-0150-0