
Abstract
Background
Breast volume is a relevant measure for the prevention and prediction of diseases and for aesthetic surgery. This study evaluated a new technique to determine breast volume and compared measures using a three-dimensional (3D) body surface scanner and magnetic resonance imaging (MRI) scans, with the latter used as the standard method.
Methods
Both MRI scans and body surface 3D scans were obtained from 22 women. For each method, breast volumes were assessed. The MRI calculations of the breast volumes were performed by a specially trained radiologist using analysis software. A textured 3D image was generated by a calibrated digital texture camera after breast surface data acquisition. The volume assessment of the 3D photography was calculated using a software package after manual outlining of the breast and automated projection of a dorsal limit. Linear regression was used to predict the MRI volume assessment with the 3D image volume assessment.
Results
The mean breast volume according to MRI volumetry was 442.8 ml on the left side and 471.8 ml on the right side. The mean breast volume using a 3D body surface volume assessment method was 273.8 ml (observer A) and 226.2 ml (observer B) on the left side and 284.4 ml (observer A) and 234.9 ml (observer B) on the right side. The use of linear regression models showed R 2 values of 0.59–0.77. The mean time for MRI recording and volume assessment was 68.0 ± 14.1 min for both sides and 11.6 ± 1.5 min for 3D recording and volume assessment.
Conclusions
The 3D surface-based volume measurements are feasible in terms of time and can predict the MRI breast volume with sufficient accuracy. This might facilitate the broad use of such an assessment technique in a large-scale epidemiologic study using breast volume as a study aim. Additionally, further development of volume assessments could help to implement this technique in breast surgery procedures.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Breast size measurement is important in several fields of research and medical care. It is used to optimize the cosmetic outcomes of breast surgery [1–5] but is linked to an increased breast cancer risk [6–8]. Measurement of breast size is described as a risk factor for the development of type 2 diabetes mellitus [9] and is of interest in aesthetic surgery regarding changes in breast shape during pregnancy [10]. Although breast volume assessment is not routinely performed in clinical practice, measurement of breast size may be a helpful diagnostic tool in various clinical and research settings.
Various methods used to measure breast volume have been reported (Table 1) [1–5, 11–30]. Morphometric methods calculate the breast volume from distances between defined reference points on the breast surface. These reference points are either measured on the patient’s body surface [24, 28] or taken from two-dimensional images such as photographs, mammograms [19, 31] or ultrasounds [21, 23] of the breast. These methods often are referred to as direct or indirect anthropomorphic measurements.
Archimedean methods are based on Archimedes’ principle of water displacement: The patient bends over the top of a filled water container, with the breast displacing water. This water is collected and measured [11, 32].
Thermoplastic sheets are a possibility for generating a three-dimensional (3D) negative cast of the breast. The resulting 3D shell is filled with water or sand to determine the breast volume [14, 17, 33]. This technique additionally allows an evaluation of symmetry, shape, and surface of the breast.
Furthermore, modern radiologic procedures such as computed tomography (CT) and nuclear magnetic resonance imaging (MRI) are widely available tools for measurement of breast volume [3, 11, 12, 15, 16, 18, 22]. To date, breast MRI can be considered the gold standard for breast size measurements [3], to which all other techniques should be compared.
Finally, new 3D body surface imaging methods such as stereo photography [2, 4, 34] and laser scanning [12, 20] are available. These methods create a virtual three-dimensional model of the breast with the body in an upright position [16]. Thus, the quantitative evaluation of symmetry, volume, shape, contour, surface, and distance measurements without contact or distortion become possible [2, 4, 12, 20, 34, 35]. Nevertheless, these new noncontact methods such as stereo photography [2, 25, 26, 30, 34, 36] and laser scanning [12] might be costly. Laser scanning devices especially need to be set up very precisely using a precise geometric apparatus [26].
Our study introduced an optical, noninvasive, 3D body surface imaging method referred to as 3D body surface volume assessment using solely visible light for measuring breast volume and surface area. This study aimed to explore how well breast volume measurement using the 3D body surface method predicts breast MRI volumetry and to assess interobserver agreement using the 3D body surface method and two independent observers.
Materials and Methods
Patients
Between March 2009 and November 2009, a total of 22 female patients who attended the University Breast Center outpatient clinics at the University Hospital of Erlangen were included in this study. The patients were older than 18 years, needed an MRI scan of the breasts independently of this study, and had no major malformations of the breast due to natural reasons or previous surgery. All the patients provided written informed consent, and the study was approved by the ethics committee at the University Hospital of Erlangen.
The MRI volume for each breast was measured by one observer. Two independent observers performed 3D body surface volume assessments, and the results were compared.
MRI Volumetry
The MRI scans were performed with a 1.5 tesla scanner (Avanto; Siemens, Erlangen, Germany). The patient was placed in a prone position with a standard breast case to prevent compression. A standard four-channel receiver breast coil was used in all cases. The examinations covered the entire breast in an axial scan direction. No intravascular contrast agent was used. The calculations of the breast volumes were performed by a specially trained radiologist using an analysis software (Syngo Software Argus 4D; Siemens). This software had been established already in clinical routine for cardiac measurements.
The breast itself was defined to include the areola, nipple, and outer surface skin as the surface limit and the pectoral muscle (excluded from volume) as the dorsal limit. The medial parasternal limit was identified, and the lateral border was defined as this point of the lateral thorax wall, where the subcutaneous fat of the breast reached the same height as the subcutaneous fat of the thorax wall. From this point, an arched line was drawn radial to the pectoral muscle. The contour was marked on every single image. The volume was calculated afterward by the software.
3D Body Surface Volume Assessment
The 3D-image was taken with the patient in an upright position using an optical 3D sensor (BreastSCAN3D; 3D-Shape GmbH, Erlangen, Germany) for acquisition of the breast surfaces. The sensor is based on a modification of the phase-measuring triangulation method. A sequence of phase-shifted fringe patterns of structured light is projected on the region of interest. Two CCD cameras record the data from different directions. Subsequently, the images of the phase-shifted patterns are evaluated via a four-shift algorithm to receive the 3D shape of the object’s surface. The 3D sensor takes advantage of an astigmatic optical device to project precise sinusoidal intensity-coded fringe patterns instead of a commonly used Ronchi-grating fringe projection. After breast surface data acquisition, a calibrated digital texture camera generates an additional textured image, which is made to overlap the geometric data. The result is a textured 3D image [37, 38] (Fig. 1).

Three-dimensional (3D) volume measurement and different aspects of the 3D measurement process. (a) Triangle-structured texture of 3D image with photo texture overlay. (b) Triangle-structured texture for calculation purposes. (c) Chest wall after removal of the breast. (d) Chest wall with interpolated dorsal boundary. (e) Breast computation for calculation of the volume
The surrounding light was standardized for every patient to avoid distortion. The photo was taken during an inspiration. The calculation of the 3D photography was performed using a software package (slim3D; 3D-Shape GmbH) according to a standardized workflow consisting of outlining the breast and calculating a back wall to complete the limits of the assumed breast volume by a new nonlinear subdivision scheme. This scheme enabled seamless integration of synthetic surfaces into measured data and volume calculation based on newly defined pyramids with the surface triangles as their base area and the volume’s center of gravity as their tip (modified Stoke’s integral theorem) [38]. This calculation was performed by two specially trained observers.
Statistical Considerations
This study aimed to explore how well breast volume measurement using the 3D body surface method predicts breast MRI volumetry and to assess interobserver agreement using the 3D body surface method performed by two independent observers.
The prediction of MRI volumes by 3D volumes was analyzed by linear regression models. For each observer (observers A and B) and each side (left and right breasts), the regression coefficients were estimated, and the R² statistic, which measures the predictive strength between the two methods, was calculated. The regression line and its 95% confidence band, which reflects the uncertainty of the line, are displayed as well as the prediction band, which reflects the uncertainty about future observations. The prediction band should capture 95% of future observations. For each regression analysis, the measurements of the opposite observer are used as “future observations” for purposes of validating the model (Fig. 2a–d).

Prediction of magnetic resonance imaging (MRI) measures from three-dimensional (3D) measures (circles). (a) Left breast and observer A. (b) Left breast and observer B. (c) Right breast and observer A. (d) Right breast and observer B. Solid line shows regression line. Long dashed curves indicate confidence band. Short dashed lines indicate prediction band (95% of future observations). Each regression analysis is evaluated by the opposite observer (squares)
Linear models were chosen because low-degree polynomial and natural cubic spline models, respectively, did not improve the predictive strength (R² similar to those of linear models). The assumption of normally distributed residuals was checked using the Shapiro–Wilk normality test with a significance level 0.1 and graphically by Q–Q plots.
The interobserver agreement was measured with concordance correlation coefficients (CCC) and analyzed with Bland–Altman plots. The CCC ranges from −1 (perfect reversed agreement) to 0 (no agreement at all) to +1 (perfect agreement) [39]. With Bland–Altman plots, the average of both observers’ measurements is plotted against the difference in the measurements. The mean difference and the “limits of agreement” (mean ± 1.96 SD) which include 95% of the differences, are calculated and displayed [40] (Fig. 3a, b).
All statistical analyses were performed using the R system for statistical computing (version 2.10.1; R Development Core Team, Vienna, Austria, 2009).

Bland-Altman plots for volume assessment of the left (a) and right (b) breasts. The middle dashed line indicates the mean difference. The upper and lower dashed lines display “limits of agreement” (mean ± 1.96 SD)
Results
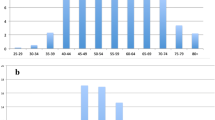
The mean age of the patients was 43.1 ± 13.1 years (range 25–71 years), and the mean body mass index (BMI) was 22.6 ± 3.3 kg/m2 (range 18–32 kg/m2). The patient characteristics are presented in Table 2. Surgery of the breast had been performed previously for 36.3% of the patients. At the time of the examination, the diagnoses were distributed as follows: benign lesion (31.8%), malignant lesion (59.1%), and normal mammogram (9.1%). The reasons for performing an MRI scan and thus inclusion in the study were unclear mammogram result (18.2%), screening for high-risk familial breast cancer (31.8%), and further diagnosis as part of preoperative breast cancer diagnostics (50%).
The mean breast volume using MRI volumetry was 442.8 ml on the left side and 471.8 ml on the right side. The confidence intervals can be seen in Table 3. The mean breast volumes using 3D body surface volume assessment were 273.8 ml (observer A) and 226.2 ml (observer B) on the left side and 284.4 ml (observer A) and 234.9 ml (observer B) on the right side. The confidence intervals can be seen in Table 3.
The mean time for MRI recording and volume assessment was 68 ± 14.1 min for both sides, and the mean time for 3D recording and volume assessment was 11.6 ± 1.5 min. Comparing these two methods regarding complete time, interobserver variability for the 3D method was assessed by Bland–Altman plots. The limits of agreement were −51.7 to 146.7 for the left breast and −27.8 to 126.8 for the right breast. The CCC was 0.90 for the left breast and 0.93 for the right breast.
For prediction of MRI volumes by 3D body surface volume assessment, linear regression models were built. Regression lines Y = a + bX with intercepts a between 114 and 192 and slopes b between 1.1 and 1.3 describe the relation between the two methods. The findings showed an R² of 0.72 for observer A and an R² of 0.59 for observer B. For the left breast, R² values of 0.77 (observer A) and 0.74 (observer B) were found. The prediction bands capture 95% of the future observations (Fig. 2a–d).
Discussion
This study showed that 3D breast volumetry is feasible and can be used to predict volumes obtained from MRI volumetry. With regard to the assessment and recording time, the 3D-measurement was significantly faster than the MRI measurement. Furthermore, the interobserver agreement was high (CCC ≥ 0.90).
As observed, the 3D method measures had a much smaller volume than the MRI. However, knowing the intercept and the slope of the regression line enabled acceptable prediction of the MRI volume with the 3D method. The R² values of approximately 0.75 confirmed the predictive strength. Other studies comparing a 3D surface method with MRI scans also measured MRI volumes larger than the 3D estimates [12, 16].
Direct comparison of 3D pictures with the MRI images showed some possible explanations for the difference. The prone position of the patients during an MRI scan changes the form of the breast and might impact the measured volume. The axillary fat (processus axillaris) is shifted to the front and might be added to the breast, whereas with an upright patient position, this tissue remains in the axillary region.
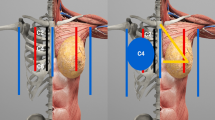
Figure 4 attempts to picture the possible major difference between the MRI and the 3D body surface scan. There is a relevant volume beneath the body surface, which would not be included in the calculation with the 3D method. The interpolation of the body surface (yellow line) and the dorsal limit of the thorax (red line) mark an area that would be included when the volume of the breast is measured using MRI scans. We hypothesize that this difference adds up to the difference between the MRI and the 3D body surface scan. The difference can be found in the positive intercept of the regression lines. The slopes greater than 1 indicate that the difference increases with increasing breast volume (Fig. 2a–d).

Exemplary difference in measurement methods. The red line represents the dorsal border of the defined volume in the magnetic resonance imaging (MRI) measurement. The yellow line represents the dorsal boundary in the three-dimensional (3D) method
Several limitations of the described measurement method must be weighed against its advantages. It works without X-rays, is fast, and has low disturbance. Additionally, the pictures are taken with the patient in an upright position, so the result is very close to the normal aspect of the breast. However, to date, this method cannot be applied for patients with clearly ptotic breasts. For these patients, the submammarian fold is difficult to determine and hence is the caudal limit of the breast.
Another possible source of inaccuracy is the dorsal boundary of the breast. Using the 3D photometric method, the dorsal limits are not visible, and the body surface surrounding the breast has an influence on the interpolation of the dorsal limit, which is used for the volume calculation. The form of the thorax itself or the amount of subcutaneous fatty tissue, for example, could have a relevant influence on the interpolation.
Problems occurring with the use of MRI are based primarily on the accrual. The MRI scans are too expensive to be performed routinely for volume measurement and too time intensive. Because the scan is performed with the patient in a prone position, the final picture is not an exact reproduction of the normal aspect. On the other hand, the measurement of ptotic breasts is not a problem, and the dorsal end of the breast can be delineated easily.
Due to the limited sample size, our analysis cannot be adjusted for possible confounders such as age, BMI, or possibly the breast size itself. Larger studies are needed to facilitate the development of more accurate and more advanced models. Compared with other studies, which have used dummies to compare methods [12, 16, 20], our study clearly aimed at implementation in clinical practice and therefore chose to test the methods with actual human beings.
In summary, we believe that the described measurement method is feasible and that the availability of the raw data allows implementation of this method in the measurement of breast volumes for large-scale epidemiologic studies such as those examining breast cancer or diabetes risk. Especially for measurements in the premenopausal setting, the X-ray free technique offers some advantages. After these early analyses, the accuracy of breast volume estimation compared with the MRI scan will be the objective of further mathematical modelling. This will enable the use of volume estimation for planning of surgical procedures in the near future.
References
Eder M, Papadopulos NA, Kovacs L (2007) Breast volume determination in breast hypertrophy. Plast Reconstr Surg 120:356–357
Galdino GM et al (2002) Clinical applications of three-dimensional photography in breast surgery. Plast Reconstr Surg 110:58–70
Herold C et al. (2010) MRI-based breast volumetry evaluation of three different software solutions. J Digit Imaging 23:603–610
Nahabedian MY, Galdino G (2003) Symmetrical breast reconstruction: Is there a role for three-dimensional digital photography? Plast Reconstr Surg 112:1582–1590
Pawluczyk O et al (2003) A volumetric method for estimation of breast density on digitized screen-film mammograms. Med Phys 30:352–364
Boyd N et al (2009) Breast tissue composition and other risk factors for breast cancer in young women: a cross-sectional study. Lancet Oncol 10:569–580
Hasenburg A et al (2000) Breast size as risk factor for tumor size at diagnosis. Anticancer Res 20:2041–2044
Jernstrom H et al (2005) Insulin-like growth factor-1 (IGF-1) genotype predicts breast volume after pregnancy and hormonal contraception and is associated with circulating IGF-1 levels: implications for risk of early-onset breast cancer in young women from hereditary breast cancer families. Br J Cancer 92:857–866
Ray JG et al (2008) Breast size and risk of type 2 diabetes mellitus. CMAJ 178:289–295
Rinker B, Veneracion M, Walsh CP (2008) The effect of breastfeeding on breast aesthetics. Aesthet Surg J 28:534–537
Bulstrode N, Bellamy E, Shrotria S (2001) Breast volume assessment: comparing five different techniques. Breast 10:117–123
Kovacs L et al (2007) Comparison between breast volume measurement using 3D surface imaging and classical techniques. Breast 16:137–145
Bookstein FL (1997) Landmark methods for forms without landmarks: morphometrics of group differences in outline shape. Med Image Anal 1:225–243
Campaigne BN et al (1979) Measurement of breast volume in females: description of a reliable method. Ann Hum Biol 6:363–367
Caruso MK et al (2006) The cost effectiveness of three different measures of breast volume. Aesthetic Plast Surg 30:16–20
Eder M et al (2008) Breast volume assessment based on 3D surface geometry: verification of the method using MR imaging. Biomed Tech Berl 53:112–121
Edsander-Nord A, Wickman M, Jurell G (1996) Measurement of breast volume with thermoplastic casts. Scand J Plast Reconstr Surg Hand Surg 30:129–132
Fowler PA et al (1990) Cyclic changes in composition and volume of the breast during the menstrual cycle, measured by magnetic resonance imaging. Br J Obstet Gynaecol 97:595–602
Kalbhen CL et al (1999) Mammographic determination of breast volume: comparing different methods. AJR Am J Roentgenol 173:1643–1649
Kovacs L et al (2006) New aspects of breast volume measurement using 3-dimensional surface imaging. Ann Plast Surg 57:602–610
Malini S, Smith EO, Goldzieher JW (1985) Measurement of breast volume by ultrasound during normal menstrual cycles and with oral contraceptive use. Obstet Gynecol 66:538–541
Palin WE Jr, von Fraunhofer JA, Smith DJ Jr (1986) Measurement of breast volume: comparison of techniques. Plast Reconstr Surg 77:253–255
Sinha SP et al (2007) Multimodality 3D breast imaging with X-ray tomosynthesis and automated ultrasound. Conf Proc IEEE Eng Med Biol Soc 2007:1335–1338
Smith DJ Jr et al (1986) Breast volume and anthropomorphic measurements: normal values. Plast Reconstr Surg 78:331–335
Tepper OM et al (2008) Three-dimensional imaging provides valuable clinical data to aid in unilateral tissue expander-implant breast reconstruction. Breast J 14:543–550
Thomson JG et al (2009) Surface area measurement of the female breast: phase I. Validation of a novel optical technique. Plast Reconstr Surg 123:1588–1596
van Engeland S et al (2006) Volumetric breast density estimation from full-field digital mammograms. IEEE Trans Med Imaging 25:273–282
Westreich M (1997) Anthropomorphic breast measurement: protocol and results in 50 women with aesthetically perfect breasts and clinical application. Plast Reconstr Surg 100:468–479
Loughry CW et al (1989) Breast volume measurement of 598 women using biostereometric analysis. Ann Plast Surg 22:380–385
Sheffer DB et al (1986) Validity and reliability of biostereometric measurement of the human female breast. Ann Biomed Eng 14:1–14
Thurfjell E et al (1996) Breast size and mammographic pattern in relation to breast cancer risk. Eur J Cancer Prev 5:37–41
Schultz RC, Dolezal RF, Nolan J (1986) Further applications of Archimedes’ principle in the correction of asymmetrical breasts. Ann Plast Surg 16:98–101
Katch VL et al (1980) Contribution of breast volume and weight to body fat distribution in females. Am J Phys Anthropol 53:93–100
Losken A et al (2005) Validating three-dimensional imaging of the breast. Ann Plast Surg 54:471–476 discussion 477–478
Lee HY, Hong K, Kim EA (2004) Measurement protocol of women’s nude breasts using a 3D scanning technique. Appl Ergon 35:353–359
Tepper OM et al (2006) Virtual 3-dimensional modeling as a valuable adjunct to aesthetic and reconstructive breast surgery. Am J Surg 192:548–551
Karbacher S, Häusler G, Schönfeld H (1999) Reverse engineering using optical range sensors in handbook of computer vision and applications, vol 3. Academic Press, Boston
Karbacher S, Seeger S, Häusler G (2001) Refining triangle meshes by nonlinear subdivision. In: Proceedings of the third international conference on 3-D digital imaging and modeling. IEEE Computer Society, Los Alamitos, pp 270–277
Lin LI (1989) A concordance correlation coefficient to evaluate reproducibility. Biometrics 45:255–268
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 327:307–310
Acknowledgments
This work was supported by a grant of the Support Association of the Tumor Registry of the University Hospital Erlangen.
Conflict of interest
Stefan Karbacher and Klaus Veit are employees of 3D-Shape GmbH Inc. However, the other authors declare no conflict of interest. The 3D imaging device was commercially purchased from 3D Shape GmbH, and no financial benefits were paid for the performance of the research.
Author information
Authors and Affiliations
Corresponding author
Additional information
Martin C. Koch and Boris Adamietz contributed equally to this work.
Rights and permissions
About this article
Cite this article
Koch, M.C., Adamietz, B., Jud, S.M. et al. Breast Volumetry Using a Three-Dimensional Surface Assessment Technique. Aesth Plast Surg 35, 847–855 (2011). https://doi.org/10.1007/s00266-011-9708-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-011-9708-x