
Abstract
Introduction
Tibiofemoral dislocation is the most serious form of instability following total knee arthroplasty (TKA). It is little reported in the literature, despite severity comparable to that in the native knee. The present systematic review and meta-analysis aimed to identify risk factors and treatment strategies.
Methods
The Cochrane, Medline (via PubMed), Google, and PROSPERO data-bases were searched in January 2018 following the PRISMA meta-analysis guidelines. All articles referring to tibiofemoral dislocation following primary TKA were included for analysis and extraction of individual data. Study data comprised age, gender, comorbidities, primary and revision implant design, aetiology, and treatment strategy.
Results
Individual data for 57 patients (23 studies) were analyzed. A total of 62.0% of primary implants were posterior-stabilized (49 patients) and 30.4% posterior-cruciate-retaining (24 patients). Obesity was the most frequent comorbidity (39.2%; 31 patients), followed by severe pre-operative deformity (31.6%; 25 patients). Aetiologies of dislocation were mainly related to comorbidity (15 studies; 65.2%) or intra-operative iatrogenic destabilization (14 studies; 60.9%). Non-operative treatment (splint) after dislocation was associated with high rates of recurrence (39.1%) but significantly fewer complications (p = 0.033). Implant revision surgery (45 patients; 80.4%) usually involved higher-constraint models (31 patients; 70.8%).
Conclusions
Improved implant design has reduced the rate of tibiofemoral dislocation, although this complication remains serious in both the short and the long term. The present review identified patient- and surgeon-related risk factors. Awareness of the former, which are identifiable pre-operatively, and of the most frequent technical errors is critical.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) is one of the most frequent orthopaedic procedures, and epidemiological studies forecast a regular increase of 3–4% in incidence per year up to 2030 [1,2,3]. Functional results and quality of life following TKA are assessed as good or very good, and 15-year survival exceeds 90% [4].
TKA revision, other than in septic aetiology, mainly concerns mechanical loosening [5]. This implicates implant design, type of bone fixation, and also ligament balance in the joint [6]. This step of the procedure is particularly complex, being the final adjustment of the joint, with deleterious consequences if adaptation is less than perfect [7, 8]: too little residual ligament laxity will cause polyethylene wear and excess stress on the bone fixation interfaces, while too much laxity will lead to instability, the most severe form of which is tibiofemoral dislocation.
This is a complication seldom reported in the literature. Frequency is estimated at 0.15–0.5% in primary TKA [9,10,11] and 3.3% in implant revision [12]. Factors predictive of tibiofemoral instability have been analyzed and the aetiologies are well-known [13]. Actual data on dislocation, on the other hand, are sparse and have not to date been specifically analyzed, although the condition is as serious as dislocation in the native knee and can even lead to amputation [14, 15].
The aims of this systematic review of the literature were to describe influencing factors for tibiofemoral dislocation after primary TKA and to assess treatment strategies.
Material and methods
Search strategy
The Cochrane and Medline (via PubMed) data-bases were searched for relevant articles and protocols, following the PRISMA guidelines for literature reviews. The last search was conducted in January 2018. No time limit was imposed on publication dates. Articles were selected if written in French or in English, with abstract available online. Before drawing up the final search strategy, a preliminary search was made of the Medline data-base to identify MeSHs words ‘dislocation’, ‘knee’, ‘arthroplasty’, and synonymous key-words. A simplified version of the strategy was implemented to study the non-published “gray” literature on the Google Search (advanced) and Google Scholar (advanced) search engines, clinical trial registries, the OpenGrey repository and websites of meetings and recognized societies. Authors were contacted whenever further data or clarifications were needed.
Eligibility and selection criteria
The results of the systematic search were synthesized using the Zotero reference management software package. Doublets were eliminated. Titles and Abstracts were selected according to the study inclusion and exclusion criteria by two of the authors (LR and GV). Full-text articles were then selected when titles and abstracts appeared relevant. Full-text reading for inclusion was performed by the two authors independently, with discussion to achieve consensus in case of disagreement. Inclusion criteria comprised (1) articles referring to tibiofemoral dislocation in primary TKA and (2) articles concerning TKA revision for tibiofemoral dislocation. Exclusion criteria comprised (1) the term “dislocation” being used to designate some other pathology, such as aseptic implant loosening, mobile insert dislocation, or patellofemoral dislocation; (2) articles concerning unicompartimental knee arthroplasty; (3) articles with insufficient data, despite direct contact with the corresponding author (2 emails at 4 weeks’ interval without response by 12 weeks).
Critical assessment of included studies
Data relevance was systematically discussed by the two authors (LR and GV). The Methodological Index for Non-Randomized Studies (MINORS) [16] was used to assess methodological quality and risk of bias in non-randomized surgical studies. This is a 12-item critical assessment tool, validated for quality assessment in non-randomized surgical studies, both comparative and not. Items are scored as 0 (not reported), 1 (insufficiently reported), or 2 (adequately reported), with an ideal score of 16 for non-comparative studies and 24 for comparative studies.
Data extraction
The two authors independently extracted the data from all included studies. Pilot extraction on the first three studies was used to standardize the process, then applied to the other studies independently. Data comprised age, gender, body mass index (BMI), comorbidities, implant design, time to dislocation and surgical revision, type of revision and type of revision implant, and causes of dislocation as identified by the study authors. Discrepancies in extraction were discussed, examined, and resolved.
Statistical analysis
Statistical analysis was conducted using Comprehensive Meta-analysis (Version 2.0; Biostat, Englewood, NJ, USA) and Stata software (version 13; StataCorp, College Station, TX, USA). Recurrence rates and 95% confidence intervals were estimated using random-effect models, assuming between- and within-study variability. Statistical heterogeneity in results was assessed on forest plots, confidence intervals, and I2. I2 values range between 0 and 100% and are typically considered low for < 25%, moderate for 25–50%, and high for > 50%. Publication bias was assessed by funnel plots and Egger’s test. Subgroup analysis was then performed. Finally, sensitivity analysis assessed the influence of the studies’ inclusion and exclusion on overall recurrence rates. More precisely, sensitivity analysis measured the impact of studies including only one patient (case reports).
For descriptive analyses, data were presented as mean and standard deviation or median and interquartile range, according to statistical distribution. All statistical analyses were carried out taking into account between- and within-study variation. To address non-independence of data due to study effects, random-effect models were performed. More precisely, a generalized linear mixed model was applied, using logistic regression.
Results
Systematic literature search
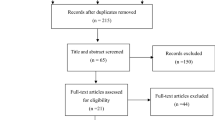
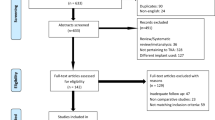
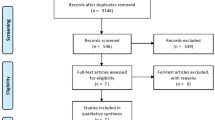
Data-base searches selected 247 articles. After reading titles and abstracts, 84 were short-listed for full-text reading. Fifty-nine articles not meeting the selection criteria were excluded, and final qualitative analysis concerned 25 studies (79 patients). Figure 1 shows the selection PRISMA flowchart.

PRISMA flowchart
The selected studies underwent systematic qualitative analysis. Most of the 25 (n = 22) were case reports; the other three were retrospective case series. Global heterogeneity (I2 index) was low, at 14.3%. Table 1 presents study characteristics. Critical assessment on MINORS gave a mean score of 12.48/16 [range, 10–14] (Table 1). Publication bias on funnel plot (Fig. 2) was assessed as low.

Funnel plot of the study
Population data
A total of 26.6% of the study population were male (n = 21), 64.4% female (n = 51), and gender was unknown for 8.8% (n = 7) (Table 2). Mean age at first dislocation was 67.5 ± 10.5 years [range, 46–85 years]. Mean time from primary TKA to first dislocation was 27.1 ± 40.1 months [range, 0.1–216 months]. In 35 patients (44.3%), dislocation occurred within the first six months; 12.7% (n = 10) had late dislocation at > five years. Osteoarthritis (n = 72; 91.1%) was the main indication for first-line treatment, followed by rheumatic arthropathy (n = 6; 7.6%) and trauma (n = 1; 1.3%). Surgical approaches and techniques were conventional, but poorly detailed in most studies. Primary implants were posterior-stabilized in 49 patients (62.0%), including nine constrained designs (CCK) (11.4%). A total of 30.4% of implants spared the posterior cruciate ligament (cruciate-retaining: CR) (n = 24) (Table 3).
Dislocation: diagnosis, mechanism, comorbidities, complications, aetiologies
Diagnosis of tibiofemoral dislocation was straightforward in all cases, with suggestive clinical presentation associating pain, deformity, and total functional impotence.
Displacement was posterior in 69 cases (83.3%), anterior in nine (11.4%), and lateral in one (1.3%). Intervals to dislocation were twice as long in anterior as posterior dislocation (65.9 versus 32.4 months). Lesion mechanisms were not always clearly identified but were either traumatic (32 patients; 40.5%), usually by low-energy body-height fall, or atraumatic (26 patients; 32.9%) due to movement in hyperflexion.
Obesity (BMI > 30) was the most frequent comorbidity, in 31 patients (39.2%) in nine studies, followed by severe pre-operative deformity, defined as > 10° varus/valgus or > 20° flexion contracture (n = 25; 31.6%) (12 studies), central or peripheral neurologic pathology (n = 6; 7.6%) (5 studies), and, to a lesser extent, psychiatric disorder or decompensated metabolic disease (Table 4).
Complications following dislocation mainly comprised knee extensor system lesions (n = 11; 14.0%): patellar fracture, patellar or quadriceps tendon tear [31], and popliteal pedicle neurovascular lesions (n = 4; 5.1%), leading to thigh-level amputation in one case (1.27%).
Aetiologies identified by study authors (Table 5) were varied and can be roughly divided into three categories: comorbidity-related, iatrogenic, or implant-related (design or constraint). Overall comorbidities were the main factor in 15 studies (65.2%), followed by intra-operative iatrogenic lesions (collateral ligament lesions, extensor system destabilization, or implant malpositioning) in 14 studies (60.9%), and implant design in three studies (n = 20; 12%), all concerning first-generation posterior-stabilized models. There was one case (1.27%) of traumatic dislocation at first verticalization after sciatic and femoral motor block [25].
Treatment options
Foremost any relocation manoeuvres, vascular and neurologic examination is essential, both before and after relocation, and vascular imaging (arteriography or CT angiography) should be performed in case of any doubt. Under general anaesthesia, relocation is performed by an orthopaedic surgeon and one assistant. Gentle and persistent axial traction are first applied to the distal tibia, then followed by anterior or posterior forces (in the opposite direction of the dislocation deformity) to relocate. Assessment of the relocation and associated injuries (fracture, ligaments…) is immediately performed by X-ray. Finally, the limb is immobilized in a 15 to 20° of flexion semi-rigid splint. No case of failure to relocate by external manoeuvres has been reported in the selected articles.
Non-operative treatment by semi-rigid splint immobilization in extension was for a mean four weeks (range, 2–10 weeks). It was implemented in first-line in 23 cases (29.1%), mostly when comorbidities precluded revision surgery (n = 14; 60.1%) or dislocation was early, or associated with trauma (n = 6; 23%). The analysis of the whole literature showed a recurrence rate of 39.1% (n = 9), with revision surgery in eight cases (88.9%) (Table 6). When failure occurred, it was always within the first six weeks.
Surgeons have chosen surgical options in first line in 48 patients (60.8%) and in second line, after failure of non-operative treatment, in eight (10.1%). Revision strategies varied between studies, and authors provided rationales.
Total revision replacing femoral and tibial components was performed in 45 patients (80.4%), systematically with more highly constrained components. No recurrence occurred and functional results were considered satisfactory by the surgeons, although objective comparison on clinical scores was lacking.
Simple polyethylene insert augmentation was used in 14 patients (25.0%): in early revision (< 6 months) for inadequate ligament balance in flexion/extension in 12 cases (85.7%), or late revision (> 5 years) for insert wear in two cases (16.7%). Simple insert replacement led to failure, with recurrence of dislocation, in 35.7% of cases (n = 5), requiring total revision with increased constraint.
Bony and ligament lesions following dislocation were managed surgically in all cases. The two cases of medial collateral ligament avulsion were treated by suture and hamstring (gracilis) tendon reinforcement. One case of patellar fracture was treated by internal fixation, and 11 patients (13.9%) with patellar or quadriceps tendon tear were successfully treated by suture reinforced by VY plasty or allograft. The rate of deep infection following revision surgery was 10.7% (n = 6), in two cases (33%) requiring new surgery by knee fusion (Tables 5 and 6).
Discussion
The present systematic review about tibiofemoral dislocation following primary TKA identified key factors for this rare but serious complication. Influencing factors were either patient- or surgeon-related.
Patient-related factors were principally comorbidity (mainly obesity (39.2%) and neuropsychiatric disorders (10.1%)) or severe pre-operative deformity (varus/valgus > 10°). The impact of obesity is easily explained by increased mechanical stress on the joint and poorer muscle quality [39]. This is seen by the fact that most low-energy dislocations in native knees concern obese subjects (57%) [27, 40, 41]. Moreover, morbid obesity is associated with 8% greater risk of medial collateral ligament avulsion in the early TKA post-operative period [42]. Neurologic pathology inducing peripheral neuromuscular disorder underlie desynchronization of joint agonist/antagonist muscles [29, 43]. Knee instability mainly implicates hamstring muscle spasticity [44,45,46]. Severe varus/valgus deformity causes ligament lesions (distension on the convex and retraction on the concave side) that can be severe and difficult to treat, especially for surgeons with limited experience [24, 26, 47].
Surgeon-related factors frequently concerned certain technical errors: faulty ligament balance in flexion and extension [18,19,20, 32, 33] especially with residual laxity in flexion, excessive soft-tissue release [35, 37], and tibial implant malpositioning, specifically in internal rotation [38]. Ligament balance in TKA is recognized as a particularly delicate step [6, 21, 23], involving all the key elements of the procedure: patient-related factors, implant positioning, and surgical technique. Good balance is essential to short-term success (functional results) but also to long-term outcome (implant survival).
Except for mistaken initial choice of constraint, implant design is no longer a determining factor for dislocation [48]. However, certain concepts and precautions have to be borne in mind by the surgeon for each type of design when he chooses one.
Posterior cruciate ligament (PCL) sparing implants depend for their stability in flexion largely on the PCL, which must therefore be intact, with normal tension. Anatomic and histologic studies have shown strong correlations between radiologic osteoarthritis grade and histologic PCL degeneration stage [17, 28, 49]. Moreover, in case of macroscopically abnormal anterior cruciate ligament, the PCL is affected in more than 50% of cases even if not torn.
In posterior-stabilized implants, dislocation mainly concerned only certain first-generation designs [22, 30, 34, 37]. To improve motion in flexion, the posterior cam of the tibial insert was reduced in size and set back so as to reduce “jump distance” [36].
Ultracongruent designs, being more “anatomic”, show a greater tendency for anteroposterior femoral translation over the tibia on kinematic studies [50]. Stability thus requires optimal soft tissue tension balance.
Treatment of dislocation comprises two distinct steps. (1) In emergency, the procedure for TKA dislocation is the same as in native knee [14, 15]. (2) After this emergency step, treatment is discussed in the light of comorbidities, soft tissue lesions, implant malpositioning, and implant design. To date, it is not possible to suggest a validated treatment for TKA dislocations because of the limitations of the available literature. Each case is specific and treatment is decided based on the pros and cons of each solution and discussion with the patient. Non-operative treatment runs a significant risk of recurrence (39.1%) but with few other complications. Implant revision with increased constraint has a high success rate (100%), but with a 10.7% rate of sepsis, which may lead to repeat revision or fusion, or at least to amputation.
This review has several limitations. First of all, heterogeneous studies were included to increase the strength of the overall analysis. This heterogeneity is a consequence of the study designs (retrospective case series or case reports), due to the rarity of this complication. This bias was controlled partly thanks to the study methodology, with a precise definition of dislocation (excluding simple instability), and to the fact that authors of each included study were contacted to check their methodology and results. The use of only English and French language papers may have incurred a selection bias, although no articles in any other language were found during various database searches. Another limitation was that each article included in the systematic review was also subject to its own biases, which could create a downstream effect in drawing the conclusions of this review. Finally, no meta-analysis with homogeneous group comparison was possible (because of the rarity of that complication), thus limiting the conclusions about the real impact of each risk factor.
Conclusion
Tibiofemoral dislocation in primary TKA is not exceptional, as the incidence of TKA is high. It is especially serious, both in the short term and in the longer term at revision. The surgeon’s awareness of the influencing factors and of the most frequent technical errors is determining. Treatment should be appropriate for each patient considering comorbidities, mechanism of dislocation, advantages, and risks of surgical solutions.
References
UK National Joint Registry (2018) www.njrcentre.org.uk/. Accessed 11 Dec 2017
U.S. Department of Health & Human Services (2018) HCUPnet. www.hcupnet.ahrq.gov/. Accessed 04 Nov 2017
The Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) (2017) Annual Reports www.aoanjrr.sahmri.com/fr/annual-reports-2017/. Accessed 29 Nov 2017
Forster MC (2003) Survival analysis of primary cemented total knee arthroplasty: which designs last? J Arthroplast 18:265–270. https://doi.org/10.1054/arth.2003.50051
Healy WL, Della Valle CJ, Iorio R et al (2013) Complications of total knee arthroplasty: standardized list and definitions of the knee society. Clin Orthop 471:215–220. https://doi.org/10.1007/s11999-012-2489-y
Peters CL (2006) Soft-tissue balancing in primary total knee arthroplasty. Instr Course Lect 55:413–417
Meloni MC, Hoedemaeker RW, Violante B (2014) Soft tissue balancing in total knee arthroplasty. Joints 2:37–40
Roche M, Elson L, Anderson C (2014) Dynamic soft tissue balancing in total knee arthroplasty. Orthop Clin N Am 45:157–165. https://doi.org/10.1016/j.ocl.2013.11.001
Villanueva M, Ríos-Luna A, Pereiro J et al (2010) Dislocation following total knee arthroplasty: a report of six cases. Indian J Orthop 44:438–443. https://doi.org/10.4103/0019-5413.69318
Conti A, Camarda L, Mannino S et al (2015) Anterior dislocation in a total knee arthroplasty: a case report and literature review. J Orthop 12:S130–S132. https://doi.org/10.1016/j.jor.2014.06.014
Arnout N, Vandenneucker H, Bellemans J (2011) Posterior dislocation in total knee replacement: a price for deep flexion? Knee Surg Sports Traumatol Arthrosc 19:911–913. https://doi.org/10.1007/s00167-010-1258-2
Saleh KJ, Dykes DC, Tweedie RL et al (2002) Functional outcome after total knee arthroplasty revision: a meta-analysis. J Arthroplasty 17:967–977. https://doi.org/10.1054/arth.2002.35823
Parratte S, Pagnano MW (2008) Instability after total knee arthroplasty. J Bone Joint Surg Am 90:184–194
Lachman JR, Rehman S, Pipitone PS (2015) Traumatic knee dislocations: evaluation, management, and surgical treatment. Orthop Clin N Am 46:479–493. https://doi.org/10.1016/j.ocl.2015.06.004
Maslaris A, Brinkmann O, Bungartz M et al (2018) Management of knee dislocation prior to ligament reconstruction: what is the current evidence? Update of a universal treatment algorithm. Eur J Orthop Surg Traumatol. https://doi.org/10.1007/s00590-018-2148-4
Slim K, Nini E, Forestier D et al (2003) Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 73:712–716
Öztürk A, Akalin Y, Çevik N, Akça MÇ (2016) Simultaneous posterior dislocation of primary total knee arthroplasty with ipsilateral tibial shaft fracture: a case report and review of literature. J Clin Orthop Trauma 7:58–60. https://doi.org/10.1016/j.jcot.2016.08.002
Ross JP, Brown NM, Levine BR (2015) Chronic knee dislocation after Total knee arthroplasty. Orthopedics 38:e1155–e1159. https://doi.org/10.3928/01477447-20151123-07
Jethanandani RG, Maloney WJ, Huddleston JI et al (2016) Tibiofemoral dislocation after Total knee arthroplasty. J Arthroplast 31:2282–2285. https://doi.org/10.1016/j.arth.2016.03.010
Sharkey PF, Hozack WJ, Booth RE et al (1992) Posterior dislocation of total knee arthroplasty. Clin Orthop:128–133
Vaishya R, Vijay V, Vaish A (2015) Dislocation of a constrained total knee arthroplasty with patellar tendon rupture after trivial trauma. Chin J Traumatol Zhonghua Chuang Shang Za Zhi 18:241–244
Serbest S, Tosun HB (2015) Dislocation of a revision total knee arthroplasty: rare but serious complication. Pan Afr Med J 20:193. https://doi.org/10.11604/pamj.2015.20.193.6374
Sato Y, Saito M, Akagi R et al (2012) Complete anterior knee dislocation 16 years after cruciate-retaining total knee arthroplasty. Orthopedics 35:e585–e588. https://doi.org/10.3928/01477447-20120327-33
Hagedorn J, Levine BR (2012) Revision surgery for a dislocated constrained total knee arthroplasty. Orthopedics 35:e1099–e1103. https://doi.org/10.3928/01477447-20120621-30
Sisak K, Lloyd J, Fiddian N (2011) Multi-ligament instability after early dislocation of a primary total knee replacement - case report. Knee 18:59–61. https://doi.org/10.1016/j.knee.2009.12.002
Ugutmen E, Ozkan K, Unay K et al (2008) Lateral dislocation of the knee joint after total knee arthroplasty: a case report. Cases J 1:75. https://doi.org/10.1186/1757-1626-1-75
Schuh A, Hönle W (2007) Atraumatic dislocation in mobile-bearing total knee arthroplasty: two case reports. Zentralbl Chir 132:460–464. https://doi.org/10.1055/s-2007-981304
Wazir NN, Shan Y, Mukundala VV, Gunalan R (2007) Dislocation after total knee arthroplasty. Singap Med J 48:e138–e140
Bron JL, Saouti R, De Gast A (2007) Posterior knee dislocation after total knee arthroplasty in a patient with multiple sclerosis. A case report. Acta Orthop Belg 73:118–121
Ng TP, Chiu KY (2003) Recurrent dislocation of total knee arthroplasty: an unusual cause. J Arthroplasty 18:1067–1070
Mine T, Tanaka H, Taguchi T et al (2004) Patellar tendon rupture and marked joint instability after total knee arthroplasty. Arch Orthop Trauma Surg 124:267–271. https://doi.org/10.1007/s00402-003-0505-0
Su Y-P, Chiu F-Y, Chen T-H (2003) Posterior dislocation after posterior stabilization TKA. J Chin Med Assoc 66:120–122
Pao J-L, Jiang C-C (2003) Above-knee amputation after recurrent dislocations of total knee arthroplasty. J Arthroplast 18:105–109. https://doi.org/10.1054/arth.2003.50006
Gidwani S, Langkamer VG (2001) Recurrent dislocation of a posterior-stabilized prosthesis: a series of three cases. Knee 8:317–320
Wang CJ, Wang HE (1997) Dislocation of total knee arthroplasty. A report of 6 cases with 2 patterns of instability. Acta Orthop Scand 68:282–285
Lombardi AV, Mallory TH, Vaughn BK et al (1993) Dislocation following primary posterior-stabilized total knee arthroplasty. J Arthroplast 8:633–639
Galinat BJ, Vernace JV, Booth RE, Rothman RH (1988) Dislocation of the posterior stabilized total knee arthroplasty. A report of two cases. J Arthroplasty 3:363–367
Bargren JH (1980) Total knee dislocation due to rotatory malalignment of tibial component: a case report. Clin Orthop:271–274
Tomlinson DJ, Morse CI, Winwood K, Onambélé-Pearson G (2016) The impact of obesity on skeletal muscle strength and structure through adolescence to old age. Biogerontology 17:467–483. https://doi.org/10.1007/s10522-015-9626-4
Georgiadis AG, Mohammad FH, Mizerik KT et al (2013) Changing presentation of knee dislocation and vascular injury from high-energy trauma to low-energy falls in the morbidly obese. J Vasc Surg 57:1196–1203. https://doi.org/10.1016/j.jvs.2012.11.067
Azar FM, Brandt JC, Miller RH, Phillips BB (2011) Ultra-low-velocity knee dislocations. Am J Sports Med 39:2170–2174. https://doi.org/10.1177/0363546511414855
Winiarsky R, Barth P, Lotke P (1998) Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am 80:1770–1774
Busse ME, Wiles CM, van DRWM (2005) Muscle co-activation in neurological conditions. Phys Ther Rev 10:247–253. https://doi.org/10.1179/108331905X78915
Shannon FJ, Cogley D, Glynn M (2004) Total knee replacement in patients with multiple sclerosis. Knee 11:485–487. https://doi.org/10.1016/j.knee.2003.10.006
Rao V, Targett JPG (2003) Instability after total knee replacement with a mobile-bearing prosthesis in a patient with multiple sclerosis. J Bone Joint Surg Br 85:731–732
Dawson-Bowling S, Tavakkolizadeh A, Cottam HL, Butler-Manuel PA (2008) Multiple sclerosis and bilateral dislocations of total knee replacements: a case report. Knee Surg Sports Traumatol Arthrosc 16:148–151. https://doi.org/10.1007/s00167-007-0439-0
Vince KG, Abdeen A, Sugimori T (2006) The unstable total knee arthroplasty: causes and cures. J Arthroplasty 21:44–49. https://doi.org/10.1016/j.arth.2006.02.101
Jeffcote B, Nicholls R, Schirm A, Kuster MS (2007) The variation in medial and lateral collateral ligament strain and tibiofemoral forces following changes in the flexion and extension gaps in total knee replacement. A laboratory experiment using cadaver knees. J Bone Joint Surg Br 89:1528–1533. https://doi.org/10.1302/0301-620X.89B11.18834
Dejour H, Walch G, Peyrot J, Eberhard P (1988) The natural history of rupture of the posterior cruciate ligament. Rev Chir Orthop Reparatrice Appar Mot 74:35–43
Mazzucchelli L, Deledda D, Rosso F et al (2016) Cruciate retaining and cruciate substituting ultra-congruent insert. Ann Transl Med 4. https://doi.org/10.3978/j.issn.2305-5839.2015.12.52
Acknowledgments
Acknowledgments to Myriam Galvin (Clinical Research Assistant).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rouquette, L., Erivan, R., Pereira, B. et al. Tibiofemoral dislocation after primary total knee arthroplasty: a systematic review. International Orthopaedics (SICOT) 43, 1599–1609 (2019). https://doi.org/10.1007/s00264-019-04287-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-019-04287-0