
Abstract
Purpose
Little data is available on the number of osteosynthesis of limbs in a country. Incidence of osteosynthesis is an essential element for the formation and organization of care. Based on the data from the work of the Hospital Information Technology Agency (http://www.atih.sante.fr/) and available in open access, we wanted to know the incidence of the number of osteosynthesis performed in France and their evolution over ten years between 2006 and 2015.
Methods
The data analyzed are derived from the website of the technical agency of information on the hospitalization (ATIH).
Results and conclusions
In France, in 2015, 267,999 limb osteosyntheses were performed. Between 2006 and 2015, the number of osteosynthesis increased by 9.1%. The incidence of limb osteosynthesis is 403.7 per 100,000 people, rising 3.9% between 2006 and 2015. In comparison, the incidence of hip prostheses increased by 12.6%, knee prosthesis by 57.4%. The main bias of the study is of course the quality of the coding of the surgeons and the establishments, a type of fracture that can enter into one or several categories of acts. In ten years, the incidence of osteosynthesis has increased little in France. The evolution is more pronounced on fractures affecting mainly the elderly, fracture of the upper end of the femur, fracture of the distal end of the radius and fracture of the ankle. The incidence of many acts of osteosynthesis is very low and therefore responsible for a weak experience for most surgeons.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
While many publications refer to fracture numbers [1, 2], little data is available on the number of osteosynthesis of limbs in a country [3], whereas fracture registers [4], allow for follow-up, better than clinical studies [5], while keeping the objective of better use of health systems in order to avoid unnecessary losses [6]. Beyond the choice of the best implant or the best surgical technique, the incidence of the osteosyntheses of the limbs has an impact on the teaching, if a minimum number of acts is not realized [7, 8]. Some surgical gestures are considered rare, some complex, sometimes both, and require an experiment. During the training of surgeons, some fractures and their treatment are mentioned only during theoretical education for a resident. Resident was unable to see or practice all types of osteosynthesis, especially since working time is limited [9].
In France, in the field of traumatology, this low exposure to osteosynthesis during the teaching period is accentuated by the desired orientation of the residents toward an early orthopaedic hyperspecialization. Many young surgeons have focused their training on the treatment of high-volume specific pathology, increasing their efficiency [10, 11]. After their installation, they no longer wish to participate in the continuity of care, having lost their competence in the field of treatment of fractures.
This decision is reinforced by the fact that many centers, in charge of trauma emergencies, do not have the appropriate equipment for care because of their own cost or storage and the low volume of passage. The number of patients per structure can be a guarantee of quality or faster management of repetitive acts [12]. The incidence of osteosynthesis, unrecognized, is an essential element for the formation and organization of care.
Based on the data from the work of the Hospital Information Technology Agency (http://www.atih.sante.fr/) and available in open access, we wanted to know the incidence of the number of osteosynthesis performed in France and their evolution over ten years between 2006 and 2015.
Methods
The data analyzed are derived from the website of the technical agency of information on hospitalization (ATIH); 139 acts derived from the common classification of medical procedures (CCAM (http://www.ameli.fr/accueil-de-la-ccam/index.php)) were retained, 62 for the lower limb, 67 for the upper limb. The key word was “osteosynthesis”. The chapters consulted are those of the upper and lower limbs. By way of comparison, we have also extracted the prosthesis of hip, knee and shoulder, first intention.
Results
In 2015, the French population was estimated at 66,381 million people (INSEE (https://www.insee.fr/fr/statistiques/1906663?sommaire=1906743)). According to the Direction of Research, Studies, Evaluation and Statistics (Drees (http://drees.social-sante.gouv.fr/IMG/pdf/rpps_medecins_-_synthese_des_effectifs_au_1er_jan2015.pdf)), as of January 1, 2015, 3157 orthopaedic surgeons were active, representing a ratio of 1 per 21,000 people.
267,999 limb osteosyntheses were performed. In ten years, between 2006 and 2015, the number of osteosynthesis increased by 9.1%. The incidence of limb osteosynthesis is 403.7 per 100,000 people (Table 1), rising 3.9% between 2006 and 2015 with a peak in 2009–2010. In comparison, the incidence of hip prostheses increased by 12.6%, knee by 57.4% (Table 2).
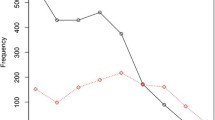
The incidence of osteosynthesis of the upper limb is 208.6 per 100,000 people (Table 3) slightly increased since 2006. Osteosynthesis of the distal end of one or both bones of the forearm is the most common with 53,204 acts, accounting for 19.85% of total osteosynthesis, 52% of which by plates in 2015 compared with 28% in 2006 (Fig. 1). The incidence is 80.1 per 100,000 people.

Evolution of lower extremity osteosynthesis techniques of a forearm bone from 2006 to 2015
Diaphysis osteosynthesis of the bones of the forearm is rarer with 8330 acts (12.5 per 100,000 people), including 5499 plates (8.3 per 100,000 people). Diaphysis osteosynthesis of the humerus is only performed in 2224 cases (3.4 per 100,000 people), that of a fracture of the scaphoid, without pseudarthrosis, in 2147 cases (3.2 per 100,000 people).
The incidence of osteosynthesis of the lower limb is 195.2 per 100,000 people and has decreased overall since 2006 (Table 4). Osteosynthesis of femoral fractures is increasing, particularly fractures of the upper femur (79.5 per 100,000 people). Osteosyntheses of malleolar fractures are frequent (38.2 per 100,000 people). As expected, osteosyntheses of fractures of the tibial pilon are rare (5.3 per 100,000 people) like that of the calcaneum (2.6 per 100,000 people).
Discussion
The main bias of the study is of course the quality of the coding of the surgeons and the establishments, a type of fracture that can enter into one or several categories. It should not be forgotten that the choice of coding impacts the remuneration of doctors especially in private practice. In our study, we did not wish to differentiate the frequency of acts in private and public practice.
Training and experience
For some uncommon acts of osteosynthesis, the question of the teaching of the surgical procedure as well as the safeguarding of acquired knowledge is asked. Osteosyntheses with a high incidence such as the hip, the lower extremity of the radius or the ankle have a high probability of being realized by the resident with good memorization of repetitive learning gestures: but a large part, complex or rare osteosyntheses can escape the teaching with only the theoretical teaching or at most a surgical assistance.
The courses developed by the industrialists or at the congresses participate in the diffusion of the most recent techniques and to share experiences on rare cases. Today, simulation training [13], is also a response to lack of exposure to acts, but it appears to be more commonly developed for frequent acts and basic techniques [14].
Beyond the simple technique, how to choose the right surgical management, choose the right technique of osteosynthesis when the type of fracture is infrequent, a choice that must also take into account evolutions, innovations and obsolescence of knowledge? The maintenance of knowledge can only be done with difficulty on the set of types of osteosynthesis at the time when the overspecialization is requested by the patients. The lack of practice and the low incidence have an impact on the literature as well: Only multicentric studies can be conducted on these low-impact osteosyntheses. The poor results of certain types of osteosynthesis may be due to the lack of practice, the small number of cases practiced, with very poor literature, sometimes with high rates of complications. For a majority of act of osteosynthesis, individual experience is fundamental.
Organization care
Sometimes a surgeon will make a gesture every two or three years because of its frequency. Associated with the tendency toward hyper-specialization, the relevance of organizations on the territories is a central answer: in France, hand emergencies have been organized (http://www.fesum.fr/). Trauma centers must cope with the demand for quality care and combine urgency and hyperspecialization. In France traumatology and osteosynthesis essentially of the lower limb, are not considered a noble activity of orthopaedic surgery. Some types of fractures can today lead to having an expertise not on the osteosynthesis but also on the prostheses such as for example the prostheses of shoulder in full growth. The centers of reference in traumatology often come from an organization based on the emergency of the 1970s, resulting from road accidents. The evolution over ten years shows an overall stagnation of the osteosynthesis with a decrease in certain areas of traumatology but there is a field in full development, that of geronto traumatology, which requires other skill than the usual centre of adult traumatology: Should we develop senior trauma centres as has been done for paediatric trauma? If the organization should, from the point of view of current incidences in France, be centered around geronto-traumatology, sports traumatology, road or heavy traumatology and paediatric traumatology, each center should be necessarily multidisciplinary, multi-professional, according to age and/or associated pathologies.
During this ten year period, there was a peak in osteosynthesis activity between 2009 and 2010 with an increase in the fractures of the upper end of the femur and fractures of the distal wrist. One of the phenomena that caught our attention was the fact that the winter of 2009–2010 was particularly harsh in France: In terms of snow occurrences, the winter of 2009–2010 is thus one of the snowiest in Europe, over the last 30 years. Always because of the persistent cold, the snow frequently hold on the ground. This peak also makes it possible to understand that only data collections over the long term make it possible to weight the analyzes.
Evolution of practices
During these ten years the most visible change in practice for osteosynthesis has been the increasing use of osteosynthesis plate for fractures of the distal end of the radius which exceeds the use of the pins, change observed in the US [15], change of practice related to new generations of surgeon and their hyper-specialization [16]. If the impact of a change in practice, type of osteosynthesis, on the clinical improvement of patients is not proven in the long term, the economic impact of practice changes must be measured [17, 18].
There is also a marked increase in clavicle osteosynthesis over this ten year period, with an increase in incidence of 50%. This evolution in management is due to certain results of orthopaedic treatment perceived as bad but not clearly proved [19]. There may also be a generational phenomenon due to hyperspecialization and/or training centres and different lobbies or school head of surgery, as observed for fractures of the distal end of the radius. Inter-relationships in the health care system can also affect treatment choices [20, 21]. It is also necessary to take account of the increasing demands of patients in a very efficient healthcare system in France, with increasingly demanding patients.
Conclusion
In ten years, the incidence of osteosynthesis has increased little in France. The evolution is more pronounced on fractures affecting mainly the elderly, fracture of the upper end of the femur, fracture of the distal end of the radius and fracture of the ankle.
The incidence of many acts of osteosynthesis is very low and therefore responsible for a weak experience for most surgeons. This weak experiment can impact the results in the literature. For frequent acts, due to the increasing importance of fractures of the elderly, organizations need to be adapted.
For all types of osteosyntheses, the present French territorial organizations are disseminating the competences, where the experiments arrive at their limits.
The information gathering system already set up in France would allow the creation of a register for the surgical treatment of fractures with a few modifications: The incidence of osteosyntheses is higher than that of prostheses and the technical guidelines can have a strong impact on costs.
References
Maravic M, Le Bihan C, Landais P, Fardellone P (2005) Incidence and cost of osteoporotic fractures in France during 2001. A methodological approach by the national hospital database. Osteoporos Int 16(12):1475–1480
van Staa TP, Dennison EM, Leufkens HG, Cooper C (2001) Epidemiology of fractures in England and Wales. Bone 29(6):517–522
Garcia P, Domnick C, Lodde G, Raschke MJ (2016) Operative treatment in orthopedics and trauma surgery: are more operations carried out in Germany? Unfallchirurg doi:10.1007/s00113-016-0275-0
Wennergren D, Ekholm C, Sandelin A, Möller M (2015) The Swedish fracture register: 103,000 fractures registered. BMC Musculoskelet Disord 16:338. doi:10.1186/s12891-015-0795-8
Sedrakyan A, Campbell B, Graves S, Cronenwett JL (2016) Surgical registries for advancing quality and device surveillance. Lancet 388(10052):1358–1360. doi:10.1016/S0140-6736(16)31402-7
Berwick DM, Hackbarth AD (2012) Eliminating waste in US health care. JAMA 307:1513-1516
Lonergan PE, Mulsow J, Tanner WA, Traynor O, Tierney S (2011) Analysing the operative experience of basic surgical trainees in Ireland using a web-based logbook. BMC Med Educ 11:70. doi:10.1186/1472-6920-11-70
Jeray KJ, Frick SL (2014) A survey of resident perspectives on surgical case minimums and the impact on milestones, graduation, credentialing, and preparation for practice: AOA critical issues. J Bone Joint Surg Am 96(23):e195. doi:10.2106/JBJS.N.00044
Ahmed N, Devitt KS, Keshet I, Spicer J, Imrie K, Feldman L, Cools-Lartigue J, Kayssi A, Lipsman N, Elmi M, Kulkarni AV, Parshuram C, Mainprize T, Warren RJ, Fata P, Gorman MS, Feinberg S, Rutka J (2014) A systematic review of the effects of resident duty hour restrictions in surgery: impact on resident wellness, training, and patient outcomes.Ann. Surg 259(6):1041–1053. doi:10.1097/SLA.0000000000000595
Mauser NS, Michelson JD, Gissel H, Henderson C, Mauffrey C (2015) Work-hour restrictions and orthopaedic resident education: a systematic review. Int Orthop 40(5):865–873. doi:10.1007/s00264-015-3045-7
Shervin N, Rubash HE, Katz JN (2007) Orthopaedic procedure volume and patient outcomes: a systematic literature review. Clin Orthop Relat Res 457:35–41
Metcalfe D, Salim A, Olufajo O, Gabbe B, Zogg C, Harris MB, Perry DC, Costa ML (2016) Hospital case volume and outcomes for proximal femoral fractures in the USA: an observational study. BMJ Open 6(4):e010743. doi:10.1136/bmjopen-2015-010743
Stirling ER, Lewis TL, Ferran NA (2014) Surgical skills simulation in trauma and orthopaedic training. J Orthop Surg Res 9:126. doi:10.1186/s13018-014-0126-z
LeBlanc J, Hutchison C, Hu Y, Donnon TA (2013) Comparison of orthopaedic resident performance on surgical fixation of an ulnar fracture using virtual reality and synthetic models. J Bone Joint Surg Am 95(9):e60, S1-5. doi:10.2106/JBJS.K.01284
Koval KJ, Harrast JJ, Anglen JO, Weinstein JN (2008) Fractures of the distal part of the radius. The evolution of practice over time. Where’s the evidence? J Bone Joint Surg Am 90(9):1855–1861. doi:10.2106/JBJS.G.01569
Waljee JF, Zhong L, Shauver MJ, Chung KC (2014) The influence of surgeon age on distal radius fracture treatment in the United States: a population-based study.J. Hand Surg Am 39(5):844–851. doi:10.1016/j.jhsa.2013.12.035
Toon DH, Premchand RA, Sim J, Vaikunthan R (2017) Outcomes and financial implications of intra-articular distal radius fractures: a comparative study of open reduction internal fixation (ORIF) with volar locking plates versus nonoperative management. J Orthop Traumatol. doi:10.1007/s10195-016-0441-8
Lenza M, Faloppa F (2015) Surgical interventions for treating acute fractures or non-union of the middle third of the clavicle. Cochrane Database Syst Rev 5:CD007428. doi:10.1002/14651858.CD007428.pub3
Campbell EG, Weissman JS, Vogeli C, Clarridge BR, Abraham M, Marder JE, Koski G (2006) Financial relationships between institutional review board members and industry. N Engl J Med 355(22):2321–2329
Cvetanovich GL, Chalmers PN, Bach BR Jr (2015) Industry financial relationships in Orthopaedic surgery: analysis of the sunshine act open payments database and comparison with other surgical subspecialties. J Bone Joint Surg Am 97(15):1288–1295. doi:10.2106/JBJS.N.01093
Huard S, Blanchet N, Leclerc G, Rochet S, Lepage D, Garbuio P, Obert L (2010) Fractures of the distal radius in patients over 70 years old: volar plates or K-wires? Chir Main 29(4):236–241. doi:10.1016/j.main.2010.06.012
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors have no financial and personal relationships with other people or organizations that could inappropriately influence their work.
Rights and permissions
About this article

Cite this article
Papin, P., Berthonnaud, E. Incidence of osteosynthesis of members in France. International Orthopaedics (SICOT) 41, 1501–1506 (2017). https://doi.org/10.1007/s00264-017-3502-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-017-3502-6