
Abstract
Purpose
Patients suffering from post traumatic osteoarthritis of the acetabulum often require a total hip arthroplasty at a relatively young age. Long-term data outcome studies for this population are lacking. We report on the long-term outcome of 20 acetabular fractures in 20 patients treated with impaction bone grafting and a cemented cup after a mean follow-up of 18 years (range, 12–26 years).
Methods
The group consisted of 14 males (70 %) and six females (30 %) with an average age of 53.3 years (range, 35–75 years) at time of surgery. No patients were lost to follow-up. Four patients died and three patients underwent a revision; at review 13 patients were still living with their implant in situ. Survivorship analysis was performed at 20 years follow-up for three endpoints.
Results
Survival rate with endpoint revision for any reason at 20 years postoperative was 74.7 % (95 % confidence interval (CI), 40–91 %), 80.0 % (95 % CI, 41–95 %) for endpoint aseptic loosening, and 63.9 % (95 % CI 32–84 %) for endpoint radiographic failure. Three acetabular components were revised at 14.5, 15.3, and 16.7 years postoperative. Two cups failed for aseptic loosening and one cup failed due to septic loosening. The average postoperative Harris hip score was 82 (range, 56–100).
Conclusion
Acetabular reconstruction with impaction bone grafting and the use of a cemented cup after acetabular fracture is an attractive technique with acceptable long-term results and a low complication and re-operation rate.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Despite the frequent use of open reposition and internal fixation (ORIF) in an effort to overcome joint damage after an acetabular fracture, post traumatic osteoarthritis is still present in 20–30 % of all cases and finally 30 % requires a total hip arthroplasty (THA) [1, 2]. Unfortunately, the results of total hip arthroplasties after post traumatic osteoarthritis appear to be inferior in comparison with THA after primary osteoarthritis [3, 4]. Significantly higher rates of aseptic loosening have been reported, which is attributable to the extent of bone stock loss, the abnormal anatomy after trauma, and the relatively young age of the patients who often have an increased activity level [5, 6]. Several authors reported inferior results of cemented cups compared to uncemented cups due to pre-existing acetabular bone loss, deformity, and compromised bone quality which may interfere with the component fixation [7, 8]. Review of the literature shows a trend towards the use of uncemented cups; however long-term results are unavailable for both cemented and uncemented cups.
We previously reported our approach in these patients using impaction bone grafting (IBG) and a cemented cup [9]. The aim of this study was to report the long-term clinical and radiographic outcome of these acetabular reconstructions with impaction bone grafting and a cemented cup after acetabular fractures at a mean follow-up of 18 years after surgery (range, 12–26 years).
Materials and methods
In this retrospective review we report on 20 consecutive patients treated from January 1984 till January 2000. All patients were treated with a cemented cup in combination with the technique of IBG for secondary osteoarthritis due to an acetabular fracture.
Fourteen males (70 %) and six females (30 %) were treated 12 (60 %) times on the left and eight (40 %) times on the right side. Nineteen fractures (95 %) occurred due to traffic accidents with high impact forces. One patient (5 %) sustained a fracture after being crushed between a truck and a wall. Twelve patients (60 %) were initially treated with ORIF and eight (40 %) were treated with closed reduction and traction.
All patients received IBG based on the combination of secondary osteoarthritis, loss of bone stock or gross deformation of the acetabulum after enduring an acetabular fracture. The average age at time of the initial fracture was 34.5 years (range, 16–72 years) and the average time from initial fracture till the operation was 20 years (range, six months to 40 years). The average age at time of surgery was 53.3 years (range, 35–75 years).
Pre-operative defects were classified according to the American Academy of Orthopaedic Surgeons (AAOS) [10]. Type 1 segmental acetabular defects were present in three patients (15 %), type 2 cavitary defects in ten (50 %), type 3 combined defects in five (25 %), and type 5 arthrodesis in two patients (10 %). At time of operation 19 patients were class A according to the Charnley classification [11], and one patient class C as a result of bilateral THA.
No patient was lost to follow-up; however, four patients died during follow-up at respectively three, four, 19, and 21 years postoperatively. None of the deceased patients died due to causes related to the THA. These patient have been followed on a regular basis and their data were included until death. Three patients underwent revision surgery, leaving 13 surviving patients with an implant still in situ available for this study. This group contained seven men (54 %) and six women (46 %) with a mean follow-up of 18 years (range, 12–26 years) after surgery.
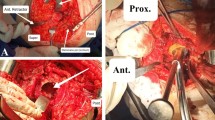
All hips were approached with a posterolateral approach. The surgical technique of cementing a cup with IBG is described in detail in our previous report [12]. Six medial wall and three peripheral wall deficiencies were reconstructed with metal meshes. Sixteen patients received an autograft, one patient only received an allograft, and three patients were treated with both auto- and allograft chips. The bone chips were produced by using a rongeur resulting in chips with an approximate diameter of 7–10 mm. The bone grafts were firmly impacted, and the last impactor was oversized by 2–4 mm relative to the final cup diameter to ensure a reproducible thickness of the cement layer. All patients were treated with antibiotic loaded cement, either Palacos® bone cement loaded with gentamicin (Merck Darmstadt, Germany) or Surgical Simplex® bone cement loaded with erythromycin and colistin (Stryker Orthopaedics, Newbury, UK). After cement pressurization the cup was inserted.
All patients were seen at least biennial for clinical and radiographic follow-up. The Harris hip score (HHS), Oxford hip score (OHS), and the visual analogue scale (VAS) for pain in rest, during activity, and for satisfaction were obtained at our clinical scoring station by an independent observer.
All radiographs were assessed by three authors (EB, MtS, and BWS). The extent of the acetabular defects was determined by using the operation record and evaluating the preoperative radiograph. Incorporation of the graft was assessed according to Slooff et al. [13]. Radiolucencies were scored in the three zones of DeLee and Charnley [14]. Migration of the cup was measured in relation to the inter-teardrop line [15, 16]. Heterotopic ossifications were scored according to Brooker et al. [17].
Clinical failure was defined as the need for a revision of the acetabular component for any reason. Radiographic failure was defined as a radiolucent line wider than 2 mm in all three zones of DeLee and Charnley [14] or migration of the socket of more than 5 mm in relation to the inter-teardrop line [15, 16]. All these radiographic endpoints were measured in the anterior-posterior view.
Kaplan-Meier survival analysis was performed for three endpoints: revision for any reason, revision for aseptic loosening, and radiographic loosening. All analyses were performed with Graphpad Prism® (La Jolla, CA) version 6.0.
Results
Clinical results
Of the surviving patients, two were unable to complete the questionnaires due to mental illness. However, their clinical status and their radiographs were available. The average pre-operative HHS was 43 (range, 26–61) (n = 10) and improved to 82 (range, 56–100) (n = 11) at final follow-up. The average post-operative OHS was 18 (range, 12–29) (n = 10), VAS rest was 13 (range 0–60) (n = 11), VAS during exercise was 18 (0–70) (n = 11), and VAS satisfaction was 89 (55–100) (n = 11). Seven out of 11 patients reported no pain in rest at final follow-up.
Revisions and re-operations
Three acetabular components were revised at a mean follow-up of 15.5 years (range, 14.5–16.7 years). The first revision was performed 14.5 years postoperative as a result of progressive pain and cup migration due to a late hematogenous infection. This patient was treated with a two stage revision for septic loosening of both components. The other two patients were treated for aseptic loosening with migration of the cup at respectively 15.3 and 16.7 years postoperative.
One patient was reoperated for a hematogenous infection four months after index surgery of the THA. The implant remained in situ and the infection was cured by placement of gentamicin beads and treatment with oral antibiotics. One other patient was reoperated upon for aseptic loosening of the femoral component 14 years postoperatively. The acetabular components in both patients are still in situ and functioning. There were no dislocations.
Radiographic analysis
Radiographs were complete in 19 patients (95 %) (Fig. 1). Five acetabular components were loose on radiographs, and their follow-up until radiographic failure was at 8, 11, 14.1, 14.5, and 16.7 years post operation. Three of these acetabular components had been revised (two due to aseptic loosening and one due to septic loosening), as mentioned before. One patient died with a migrated cup in situ. The last patient is still functioning with the loose cup in situ; radiographs showed a radiolucent line in zone one, an osteolytic process in zone three, and craniomedial migration of more than 5 mm. The majority of the migration occurred in the first postoperative year and stabilized afterwards. Although this cup failed for radiographic survivorship, the patient still reported a HHS of 96 at final follow-up.

a The anterior–posterior radiographs of a 52-year-old woman with an extensive acetabular fracture treated conservatively. b Eight years after the trauma with post traumatic osteoarthritis, extensive bone loss, and an impaired biomechanical anatomy. c Directly postoperative after the acetabular reconstruction with a mesh on the medial side of the bone graft, thereby restoring the biomechanical anatomy. d The last radiograph taken 23 years postoperative at last inspection
Analysis of the remaining 12 cups revealed radiolucent lines in nine of the 36 evaluated zones (25 %). Three cups showed radiolucent lines in two zones and three cups showed a radiolucent line in one zone. Five of these nine zones were progressive. Graft incorporation was seen in 31 zones, six zones were not incorporated, and we were unable to classify two zones due to an overlying mesh. The average wear was 0.09 mm/year (range, 0.03–0.22 mm/year). Eleven patients (55 %) showed no sign of peri-articular ossifications, eight patients (40 %) were class І, and one patient (5 %) was class ІІІ according to the Brooker classification [17]. Three of these nine patients (33 %) had pre-existent peri-articular ossification.
Survivorship analysis
Using the Kaplan-Meier survival analysis, the 20-year survivorship was 74.7 % (95 % CI 40–91 %; Fig. 2a and Table 1) for cup revision for any reason, 80.0 % (95 % CI 41–95 %; Fig. 2b) for cup revision for aseptic loosening, and 63.9 % (95 % CI 32–84 %; Fig. 2c) for radiographic failure.

a–c Kaplan-Meier survival curves showing the survival of the acetabular components for three endpoints: revision for any reason, revision for aseptic loosening, and radiographic failure. The dashed lines indicate the 95 % confidence interval
Discussion
The purpose of this study was to fill the gap in literature on long-term outcome data after inserting a total hip implant in patients with secondary osteoarthritis after an acetabular fracture. Therefore, we report the long-term survival of cemented cups in combination with IBG after enduring an acetabular fracture with loss of bone stock. The outcome is acceptable with a survival rate of the acetabular reconstructions of 75 % with endpoint revision for any reason after 20 years follow-up.
Even though our group is small, we think our data are relevant. All patients with secondary osteoarthritis after an acetabular fracture were treated with the same protocol during the observed study period, so there is no treatment bias. We only use impaction bone grafting in acetabuli that are really deformed after the acetabular fracture, so this study is based on the more severe cases. In cases with minimal bone loss or deficiency after an acetabular fracture, we just cement the cup. No patient was lost to follow-up, despite the long follow-up. The technique of using IBG with a cemented cup has not changed and is still an option nowadays. In addition, the average follow-up of 18 years is long compared to similar studies that report an average follow-up of 4.7–12 years [1, 4, 7, 8, 18–20]. All our patients were seen on a biennial basis at our outpatient clinic and radiographic files were complete in nearly all cases.
Limitations of this study are the amount of patients included and the lack of pre-operative radiographs of the initial trauma. Pre-operative radiographs of the original trauma were only available in eight out of 20 patients (40 %) due to the fact that the initial trauma was treated in another trauma center. Therefore, it was impossible to classify the initial fracture pattern.
Comparison of our results to the literature is hampered due to the lack of studies with a similar follow-up. Weber et al. [7] reported a survival rate with endpoint aseptic loosening of 83 % (95 CI, 72–97 %) after 15 years follow-up in a group that contained 44 cemented cups and 22 uncemented cups. The average follow-up for the uncemented cups was 3.9 years and 14.9 years for the cemented cup. Therefore, the survival after 15 years within their population was mainly based on the results of the cemented cups, which confirms that cemented cups do well after acetabular fractures with comparable outcomes to ours at 15 years. Certainly, the survival rates in our study slightly declined after 20 years, but Harris hip scores were still acceptable and comparable to scores published by other authors which varied between 72 and 93 after substantially shorter follow-up periods [1, 7, 18–20]. In addition, both the survival and the clinical scores are comparable to the results seen in patients treated with acetabular IBG and a primary THA [21]. Complication rates remained low with two re-operations and three revisions. All three revised hips are currently still functioning after an average follow-up of ten years after revision. This correlates with the statement that the use of IBG reconstitutes the bone stock loss, facilitating a future revision when necessary [9, 22].
We agree with Romness and Lewallen et al. [8] that the extent of bone stock loss and presence of abnormal anatomy increases the failure rate. However, we disagree with their recommendation that initial ORIF is essential to reconstruct the anatomy for a subsequent THA [18]. Miller et al. [23] presented a case series in which the accuracy of the fracture reduction with ORIF was thought to be anatomical in 58 %, imperfect in 29 %, and poor in 13 % on plain radiographs. Unfortunately, evaluation with CT images revealed an imperfect reduction in 51 % and poor reduction in 49 % of all cases. The author found no correlation between radiographic and clinical outcome [23]. There is also no clear evidence ORIF improves the success rate of the subsequent THA [6]. Due to the previous operation, there is an increased risk of developing an infection, peri-articular ossifications and scar tissue, and the presence of retained hardware increases the complexity of the placement of the THA [18, 24].
Placement of an uncemented implant without IBG can be challenging due to the necessary removal of retained hardware which can significantly lengthen the operation time and thereby cause increased infection risk [19, 25]. Bellabarba et al. [18] reported the results of a population treated with an uncemented cup and found a significant difference of 45 min in operation time between the ORIF and the closed-treatment group. Within our group we found no significant difference (p = 0.38, 23 min).
In conclusion, the use of a cemented cup in combination with IBG in deformed acetabuli with bone stock loss after acetabular fractures results in satisfying outcome, even at 20 years after surgery.
References
Ranawat A, Zelken J, Helfet D, Buly R (2009) Total hip arthroplasty for posttraumatic arthritis after acetabular fracture. J Arthroplast 24(5):759–767. doi:10.1016/j.arth.2008.04.004
Carroll EA, Huber FG, Goldman AT, Virkus WW, Pagenkopf E, Lorich DG, Helfet DL (2010) Treatment of acetabular fractures in an older population. J Orthop Trauma 24(10):637–644. doi:10.1097/BOT.0b013e3181ceb685
Malkin C, Tauber C (1985) Total hip arthroplasty and acetabular bone grafting for unreduced fracture-dislocation of the hip. Clin Orthop Relat Res 201:57–59
Berry DJ, Halasy M (2002) Uncemented acetabular components for arthritis after acetabular fracture. Clin Orthop Relat Res 405:164–167
Jimenez ML, Tile M, Schenk RS (1997) Total hip replacement after acetabular fracture. Orthop Clin N Am 28(3):435–446
Mears DC, Velyvis JH (2001) Primary total hip arthroplasty after acetabular fracture. Instr Course Lect 50:335–354
Weber M, Berry DJ, Harmsen WS (1998) Total hip arthroplasty after operative treatment of an acetabular fracture. J Bone Joint Surg Am 80(9):1295–1305
Romness DW, Lewallen DG (1990) Total hip arthroplasty after fracture of the acetabulum. Long-term results. J Bone Joint Surg Br Vol 72(5):761–764
Schreurs BW, Zengerink M, Welten ML, van Kampen A, Slooff TJ (2005) Bone impaction grafting and a cemented cup after acetabular fracture at 3–18 years. Clin Orthop Relat Res 437:145–151
D’Antonio JA, Capello WN, Borden LS, Bargar WL, Bierbaum BF, Boettcher WG, Steinberg ME, Stulberg SD, Wedge JH (1989) Classification and management of acetabular abnormalities in total hip arthroplasty. Clin Orthop Relat Res 243:126–137
Boardman KP, Charnley J (1978) Low-friction arthroplasty after fracture-dislocations of the hip. J Bone Joint Surg Br Vol 60-B(4):495–497
Schreurs BW, Slooff TJ, Gardeniers JW, Buma P (2001) Acetabular reconstruction with bone impaction grafting and a cemented cup: 20 years experience. Clin Orthop Relat Res 393:202–215
Slooff TJ, Buma P, Schreurs BW, Schimmel JW, Huiskes R, Gardeniers J (1996) Acetabular and femoral reconstruction with impacted graft and cement. Clin Orthop Relat Res 324:108–115
DeLee JG, Charnley J (1976) Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res 121:20–32
Garbuz D, Morsi E, Mohamed N, Gross AE (1996) Classification and reconstruction in revision acetabular arthroplasty with bone stock deficiency. Clin Orthop Relat Res 324:98–107
Goodman SB, Adler SJ, Fyhrie DP, Schurman DJ (1988) The acetabular teardrop and its relevance to acetabular migration. Clin Orthop Relat Res 236:199–204
Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr (1973) Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Joint Surg Am 55(8):1629–1632
Bellabarba C, Berger RA, Bentley CD, Quigley LR, Jacobs JJ, Rosenberg AG, Sheinkop MB, Galante JO (2001) Cementless acetabular reconstruction after acetabular fracture. J Bone Joint Surg Am 83-A(6):868–876
Lizaur-Utrilla A, Sanz-Reig J, Serna-Berna R (2012) Cementless acetabular reconstruction after acetabular fracture: a prospective, matched-cohort study. J Trauma Acute Care Surg 73(1):232–238. doi:10.1097/TA.0b013e31824cf39e
Pritchett JW, Bortel DT (1991) Total hip replacement after central fracture dislocation of the acetabulum. Orthop Rev 20(7):607–610
Welten ML, Schreurs BW, Buma P, Verdonschot N, Slooff TJ (2000) Acetabular reconstruction with impacted morcellized cancellous bone autograft and cemented primary total hip arthroplasty: a 10- to 17 year follow-up study. J Arthroplast 15(7):819–824
van Egmond N, De Kam DC, Gardeniers JW, Schreurs BW (2011) Revisions of extensive acetabular defects with impaction grafting and a cement cup. Clin Orthop Relat Res 469(2):562–573. doi:10.1007/s11999-010-1618-8
Miller AN, Prasarn ML, Lorich DG, Helfet DL (2010) The radiological evaluation of acetabular fractures in the elderly. J Bone Joint Surg Br Vol 92(4):560–564. doi:10.1302/0301-620x.92b4.23494
Sermon A, Broos P, Vanderschot P (2008) Total hip replacement for acetabular fractures. Results in 121 patients operated between 1983 and 2003. Injury 39(8):914–921. doi:10.1016/j.injury.2007.12.004
Willis-Owen CA, Konyves A, Martin DK (2010) Factors affecting the incidence of infection in hip and knee replacement: an analysis of 5,277 cases. J Bone Joint Surg Br 92(8):1128–1133. doi:10.1302/0301-620x.92b8.24333
Acknowledgments
We thank Dr. Jan C.M. Hendriks for statistical analysis of the data.
Conflict of interest
None to be declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bronsema, E., te Stroet, M.A.J., Zengerink, M. et al. Impaction bone grafting and a cemented cup after acetabular fracture. International Orthopaedics (SICOT) 38, 2441–2446 (2014). https://doi.org/10.1007/s00264-014-2411-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-014-2411-1