
Abstract
Purpose
Heterotopic ossification (HO) after total hip arthroplasty (THA) is a frequent complication that compromises the success of this procedure; however, its precise pathogenesis is unknown. Patient-related risk factors have previously been investigated to predict patients likely to have HO. In this study, we compared bone mineral density (BMD) between patients with and without HO after THA.
Methods
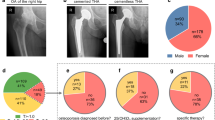
We measured BMD of the lumbar spine, radius, and calcaneus using dual-energy X-ray absorptiometry in 98 females who were scheduled to undergo THA. Radiographs were graded for the presence of HO according to the criteria of Brooker at a minimum follow-up of two years following THA. BMD were compared between those with HO and those without.
Results
In total, HO was observed in 20 of 98 hips. There were no significant differences in age, height, weight, body mass index, and pre-operative total hip score between the HO and non-HO groups. No significant difference was observed in BMD of the lumbar spine, distal radius, mid-radius, and calcaneus between the two groups.
Conclusions
Our findings suggest that generalized BMD is not related to the occurrence of HO after THA in women.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Heterotopic ossification (HO) after total hip arthroplasty (THA) is a frequent complication that sometimes compromises the success of this procedure [7]. Although the precise pathogenesis is unknown, HO seems to result from the differentiation of pluripotent mesenchymal stem cells, likely to be caused by an interaction between local and systemic factors [4].
Numerous factors have been reported to be associated with an increased incidence of HO. These factors were classified into three categories: (1) disease related (e.g., ankylosing spondylitis [1, 13, 24]); (2) operation technique related (e.g., soft tissue trauma [1] and surgical approach [19]); and (3) patient-related risk factors (e.g., male [2, 20], hypertrophic osteoarthritis (OA) [1, 2, 14, 20, 23], and history of HO [10]).
Other patient-related risk factors have been shown to be useful to predict patients likely to have HO. In particular, bone mineral density (BMD) was used to evaluate generalized bone status and diagnose the presence of osteoporosis clinically [15]. Men usually have a higher BMD compared with women [15]. In addition, patients with hypertrophic OA had a higher BMD compared with patients with no osteophytes [12]. Results of these clinical studies suggest that patients with higher BMD are at risk for HO after THA.
To further investigate the role of BMD as a predictor for HO after THA, we measured BMD of patients who were scheduled to undergo THA and determined whether patients with higher BMD are more likely to develop HO after THA.
Patients and methods
Between 2000 and 2006, we measured BMD of patients who were scheduled to undergo THA for hip OA. The protocol of this study was approved by the Institutional Review Board of our institution. We excluded patients with a history of hip osteotomy and OA hip secondary to hip fracture, inflammatory rheumatic disease, osteonecrosis, and infectious disease. Patients using any medication that could affect bone metabolism, such as steroids, were also excluded from the study.
The transgluteal approach and the Cementless Synergy total hip system (Smith and Nephew, TN, USA) were used in all cases. All the patients received non-steroidal anti-inflammatory drugs (NSAIDs) for pain for 7 days after THA. None of the patients received radiotherapeutic prophylaxis against HO.
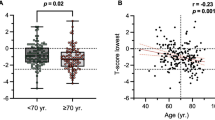
In total, 101 females were included in the study. Males were excluded from the analysis to match for sex. Three females were excluded from the study because they were lost to follow-up before the minimum two-year requirement after surgery. We could contact two of these by telephone, but they did not visit our hospital, and could not contact the third because she had moved elsewhere. The mean age of these three patients at surgery was 77.2 years (range 72–85 years) and the mean duration of follow-up was 1.1 years (range 0.5–1.8 years). Radiographically, none of these three patients showed signs of HO. With a recall rate of 97%, the remaining 98 women attended the follow-up for radiographical assessment for more than two years. The mean postoperative follow-up for the entire group was 5.3 years (range two to eight years), and the mean age at surgery was 61.2 years (range 43–84 years).
All radiographs were performed in the supine position. Anteroposterior radiographs were taken with a source-to-film distance of 110 cm. The patient’s feet were internally rotated with the toes at 15 ± 5° and the X-ray beam was centered on the superior aspect of the pubic symphysis.
Clinical symptoms were evaluated using Merle d’Aubigne and Postel’s [17] hip-joint scoring system, in which a maximum of six points in each case is assigned according to the following three criteria: pain, mobility, and walking ability.
Radiographs were graded for the presence of HO according to the following criteria of Brooker et al. [7]—class I: islands of bone within the soft tissues about the hip; class II: bone spurs from the pelvis or proximal end of the femur, leaving at least 1 cm between opposing bone surfaces; class III: bone spurs from the pelvis or proximal end of the femur, reducing the space between opposing bone surfaces less than 1 cm; and class IV: apparent bone ankylosis of the hip.
BMD of the lumbar spine (L2–4) in the anteroposterior projection was determined using dual-energy X-ray absorptiometry (DXA). Fractured vertebrae were eliminated from analysis. Radial BMD was measured in a non-dominant side of the distal and midshaft point located at one-third of the distance from the ulnar styloid process to the olecranon process (mid-radius) using DXA. The values obtained were expressed as grams per square centimeter for the projected area. EXP5000 (Lunar, Madison, WI) was used to measure BMD of the lumbar spine and radius. Calcaneal lateral integral BMD on the left side was measured by DXA (Heel Scan DX-2000; KDK, Kyoto, Japan). These values were also expressed as grams per square centimeter for the projected area.
The reproducibility expressed as coefficient of variation for the L2–4, radius, and calcaneus, was measured on five occasions consecutively on the same day in five healthy volunteers.
We assessed differences between the HO and non-HO groups using the Mann–Whitney U test. Differences with a p value of <0.05 were considered significant.
Results
Of the 98 hips reviewed, HO was observed in 20 (20.4 %). HO was graded as class I in 14 hips (14%), class II in two (2%), and class III in 4 (4%). There were no cases of class IV HO.
Patients were divided into HO (20 hips) and non-HO (78 hips) groups, and BMD was compared between the two groups. There were no significant differences in age, height, weight, body mass index, and pre-operative total hip score between the HO and non-HO groups (Table 1). Furthermore, no significant difference in BMD of the lumbar spine, distal radius, mid-radius, and calcaneus was observed between the HO and non-HO groups (Table 2).
The coefficients of variation for the L2–4, radius, and calcaneus were 1.1%, 1.8%, and 0.8%, respectively.
Discussion
In the present study, the patient-related risk factors of HO after THA have been investigated to predict which patients are likely to have HO [1, 2, 10, 13, 19, 20, 23, 24]. We measured BMD of patients who were scheduled to undergo THA to determine whether patients with higher BMD levels more often have HO after THA.
Our study had several limitations. First, this study is the inclusion of a relatively small number of patients with HO. Although there were no significant differences in BMD, mean BMDs measured at all locations considered in this study were lower in patients with HO than those without HO. In the future, large-scale studies will be useful for detailed investigation of the association between HO and BMD. Second, all the patients received non-steroidal anti-inflammatory drugs (NSAIDs) for seven days after THA. Recently, nonselective NSAIDs or selective cyclo-oxygenase-2 inhibitors have been reported to be equally effective for the prevention of HO [25]. NSAIDs may reduce the number of patients with HO in this study. Third, we did not measure the BMD around the hip joint. Degenerative changes in the articular cartilage of the hip joint are accompanied or preceded by increased subchondral bone density, leading to radiographically observable sclerosis [5]. These findings suggest that increased BMD around the osteoarthritic hip joint may be a component of the disease process in hip OA. Therefore, to estimate the relationship between HO and BMD, BMD at sites other than the proximal femur in patients with hip OA needs to be measured. We measured BMD at the lumbar spine, radius, and calcaneus. We considered that these sites are suitable to evaluate the general bone status of patients with OA.
Numerous publications have reported the relationship between generalized BMD and patients with OA hip [3, 8, 9, 11, 14, 16, 18]. Higher BMD was previously reported in patients with OA hip compared with healthy controls [3, 8, 9, 11, 14, 16, 18], and severe OA hip was associated with a higher BMD than mild OA hip [9, 18]. The general opinion is that the incidence of osteoporosis is inversely associated with the incidence of OA [21]. Despite such clinical evidence supporting the relationship between incidence of HO and generalized BMD in patients with OA hip, no relationship was observed in this study.
Bombelli classified the osteoblastic response of the OA hip into three categories—hypertrophic, normotrophic, and atrophic—based on osteophyte formation observed on radiographs [6]. There have been several reports of patients with hypertrophic OA who had higher BMD compared with those without osteophyte formation. For example, Hannan et al. [12] reported that in women with osteophytosis of the knee, femoral BMD was higher. Furthermore, Schnitzler et al. [22] examined bone histomorphometry of the iliac crest and spinal fracture prevalence in women with OA hip and concluded that patients with atrophic OA have a high prevalence of generalized osteoporosis. Patients with higher BMD were bone formers, and thus, had an increased tendency toward osteophytosis, in contrast to subjects with lower BMD. In our study, mean BMD of the lumbar spine, distal radius, mid-radius, and calcaneus were lower in patients with HO than those without HO. The bone status for patients with osteophyte formation associated with OA may be different from those with HO after THA.
In this study, no significant difference was observed in BMD of the lumbar spine, radius, and calcaneus between patients with HO and without HO after THA. Our findings suggest increased generalized BMD at the time of THA is not indicative of HO.
References
Ahrengart L (1991) Periarticular heterotopic ossification after total hip arthroplasty. Risk factors and consequences. Clin Orthop Relat Res 263:49–58
Ahrengart L, Lindgren U (1993) Heterotopic bone after hip arthroplasty. Defining the patient at risk. Clin Orthop Relat Res 293:153–159
Antoniades L, MacGregor AJ, Matson M, Spector TD (2000) A cotwin control study of the relationship between hip osteoarthritis and bone mineral density. Arthritis Rheum 43:1450–1455
Board TN, Karva A, Board RE, Gambhir AK, Porter ML (2007) The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 89:434–440
Bolotin HH (2007) DXA in vivo BMD methodology: an erroneous and misleading research and clinical gauge of bone mineral status, bone fragility, and bone remodelling. Bone 41:138–154
Bombelli R (1983) Osteoarthritis of the hip: classification and pathogenesis, 2nd edn. Springer, Berlin
Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr (1973) Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Joint Surg Am 55:1629–1632
Bruno RJ, Sauer PA, Rosenberg AG, Block J, Sumner DR (1999) The pattern of bone mineral density in the proximal femur and radiographic signs of early joint degeneration. J Rheumatol 26:636–640
Burger H, van Daele PL, Odding E, Valkenburg HA, Hofman A, Grobbee DE, Schutte HE, Birkenhager JC, Pols HA (1996) Association of radiographically evident osteoarthritis with higher bone mineral density and increased bone loss with age. The Rotterdam Study. Arthritis Rheum 39:81–86
DeLee J, Ferrari A, Charnley J (1976) Ectopic bone formation following low friction arthroplasty of the hip. Clin Orthop Relat Res 121:53–59
Gotfredsen A, Riis BJ, Christiansen C, Rodbro P (1990) Does a single local absorptiometric bone measurement indicate the overall skeletal status? Implications for osteoporosis and osteoarthritis of the hip. Clin Rheumatol 9:193–203
Hannan MT, Anderson JJ, Zhang Y, Levy D, Felson DT (1993) Bone mineral density and knee osteoarthritis in elderly men and women. The Framingham Study. Arthritis Rheum 36:1671–1680
Higo T, Mawatari M, Shigematsu M, Hotokebuchi T (2006) The incidence of heterotopic ossification after cementless total hip arthroplasty. J Arthroplasty 21:852–856
Jordan GR, Loveridge N, Bell KL, Power J, Dickson GR, Vedi S, Rushton N, Clarke MT, Reeve J (2003) Increased femoral neck cancellous bone and connectivity in coxarthrosis (hip osteoarthritis). Bone 32:86–95
Lim LS, Hoeksema LJ, Sherin K (2009) Screening for osteoporosis in the adult U.S. population: ACPM position statement on preventive practice. Am J Prev Med 36:366–375
Makinen TJ, Alm JJ, Laine H, Svedstrom E, Aro HT (2007) The incidence of osteopenia and osteoporosis in women with hip osteoarthritis scheduled for cementless total joint replacement. Bone 40:1041–1047
Merle D’Aubigne R, Postel M (1954) Function al results of hip arthroplasty with acrylic prosthesis. J Bone Joint Surg Am 36-A:451–475
Nevitt MC, Lane NE, Scott JC, Hochberg MC, Pressman AR, Genant HK, Cummings SR (1995) Radiographic osteoarthritis of the hip and bone mineral density. The Study of Osteoporotic Fractures Research Group. Arthritis Rheum 38:907–916
Pai VS (1994) Heterotopic ossification in total hip arthroplasty. The influence of the approach. J Arthroplasty 9:199–202
Ritter MA, Vaughan RB (1977) Ectopic ossification after total hip arthroplasty. Predisposing factors, frequency, and effect on results. J Bone Joint Surg Am 59:345–351
Sambrook P, Naganathan V (1997) What is the relationship between osteoarthritis and osteoporosis? Baillieres Clin Rheumatol 11:695–710
Schnitzler CM, Mesquita JM, Wane L (1992) Bone histomorphometry of the iliac crest, and spinal fracture prevalence in atrophic and hypertrophic osteoarthritis of the hip. Osteoporos Int 2:186–194
Sneath RJ, Bindi FD, Davies J, Parnell EJ (2001) The effect of pulsed irrigation on the incidence of heterotopic ossification after total hip arthroplasty. J Arthroplasty 16:547–551
Sundaram NA, Murphy JC (1986) Heterotopic bone formation following total hip arthroplasty in ankylosing spondylitis. Clin Orthop Relat Res 207:223–226
Xue D, Zheng Q, Li H, Qian S, Zhang B, Pan Z (2011) Selective COX-2 inhibitor versus nonselective COX-1 and COX-2 inhibitor in the prevention of heterotopic ossification after total hip arthroplasty: a meta-analysis of randomised trials. Int Orthop 35:3–8
Acknowledgement
We would like to thank our research assistants Ms Mieko Motoki, Ms Mari Tahara, Mrs Tomoko Maeda and Ms Rumi Inomata for their invaluable efforts in making this study possible. We also appreciate Dr Kenichi Mihara for advice on writing English articles.
Author information
Authors and Affiliations
Corresponding author
Additional information
No benefits in any form have been received or will be received from a commercial party related directly to the subject of this article.
Rights and permissions
About this article
Cite this article
Okano, K., Aoyagi, K., Osaki, M. et al. Bone mineral density is not related to heterotopic ossification after total hip arthroplasty. International Orthopaedics (SICOT) 36, 1163–1166 (2012). https://doi.org/10.1007/s00264-011-1446-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-011-1446-9