
Abstract
We retrospectively analysed 106 consecutive traumatic humeral shaft fractures over a five-year period. The mechanism of injury, age, gender, fracture types, associated injury and the presence of injury to the radial nerve were reviewed. The incidence was about 10 per 100,000 per year; most were closed fractures in young males which had been sustained as a result of traffic accidents. The age–gender distribution was characterised by gradually increased incidence from the fifth decade in women, while it reached a peak at the third decade and decreased after the fifth decade in men. The results revealed different epidemiological features from previous studies. The epidemiology differs between ethnicity and country, and updating the epidemiological features of humeral shaft fractures may provide information for appropriate treatment programmes. This study documents the epidemiology of humeral shaft fracture in Taiwan, probably for the first time in this Asian community.
Résumé
Nous avons analysé de façon rétrospective 106 fractures traumatiques de la diaphyse humérale sur une période de 5 ans. Le mécanisme du traumatisme, l’âge, le sexe, le type de fractures, le type de traumatismes et la présence de lésion du nerf radial ont été analysés. L’incidence est, approximativement de 10 pour un million de personnes par an. La plupart sont des fractures à foyer fermé sur des sujets jeunes de sexe masculin secondaires à des accidents de la circulation. L’analyse de l’âge et du sexe permet de mettre en évidence une augmentation de l’incidence de cette fracture chez les femmes dans les 5 premières décades, avec un pic à 30 ans et une diminution après 50 ans chez l’homme. Les résultats de l’étude épidémiologique permettent un algorithme chirurgical adapté. Il s’agit probablement de la première étude asiatique, elle a été réalisée à Taiwan.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Humeral shaft fractures account for 1∼3% of all fractures. There have been few studies about the epidemiology of humeral shaft fractures in the past 30 years. There are many inherent difficulties in the study of orthopaedic trauma epidemiology. Most of the studies on humeral shaft fractures pay more attention to the treatment options and compare their effects. A defined population should be studied in order to obtain a true picture of the epidemiology of these fractures. The epidemiological features of the humeral shaft fracture have been reported in European and African subjects, but it is not available in the Asian group. The epidemiological picture of fractures varies between communities as a result of differences in racial, socioeconomic, cultural, degree of urbanisation and other population characteristics. Hence, there is the need for this study. The study of orthopaedic epidemiology is useful in the planning, training and resource management of orthopaedic traumatology.
Materials and methods
We retrospectively analysed the antero-posterior radiographs of all in-patients and out-patients with humeral diaphyseal fracture over a 5-year period (January 2003 to December 2007) in our hospital. Our hospital serves a population of about 1,000,000 people in Taichung City of central Taiwan, and most of the patients with a traumatic event in this area were sent to the hospital. A diaphyseal fracture was defined as one occurring between the superior border of the insertion of the pectoralis major and the area immediately above the supracondylar ridge, according to Tytherleigh-Strong et al. [9]. We excluded pathological fractures of the humeral shaft due to the definition of the true injury mechanism in our group. There were 106 traumatic humeral shaft fractures in this series. The fracture patterns were classified according to the Orthopaedic Trauma Association system [5]. Open fractures were classified using the Gustilo system [2]. The medical records regarding the mechanism of injury, age, gender, fracture level and the presence of injury to the radial nerve were reviewed. The mechanism of injury was classified as a simple fall, fall from a height, traffic-related accident, sport-related and miscellaneous (e.g. crushing injury and assault). A simple fall was defined as that from a standing height and a fall from height as that from a higher level, such as falling down from stairs or furniture. The overall incidence and the age-specific incidence were calculated on the basis of data from the Taichung government [8].
Statistical analysis
Nominal variables were tested by the chi-square test. Multivariable logistic regression analysis was performed to identify causative factors for palsy of the radial nerve. The site of fracture, the pattern, age and mechanism of injury were treated as independent variables. We also compared the age effect between genders. Values are expressed as the odds ratio (OR) with their corresponding 95% confidence intervals (CI) and p-values. A p-value of less than 0.05 was considered to be significant. The statistical software used for the analyses was SAS 9.1 for Windows.
Ethical issue
The study was performed according to the Declaration of Helsinki [10], and the Local Ethics Committee approved the study protocol.
Results
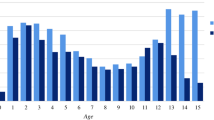
The epidemiological data and age distribution of the study cohort are shown in Table 1 and Fig. 1, respectively. Most of the fractures were closed injuries in adult patients resulting from traffic accidents. The mean age was 40.3 years (range 9 to 82). The mean age for females was 50.8 years (range 17 to 82) and for males 31.7 years (range 9 to 70) (p<0.005). The overall age distribution has a peak at the third decade. The age distribution in women was bimodal, with a peak in the third and seventh decades, while in men there was a peak in the third decade and a drop after the fifth decade. Type-A fractures (simple) were, by far, the most common (67.9%), followed by type-B (wedge; 28%) and type-C (complex; 3.7%). The mid-shaft was fractured in 66%, the proximal third in 13% and the distal third in 21.7% of patients. Type A3, a simple transverse fracture of the mid-shaft, was the most common (25.5%).

Age distribution of the 106 fractures of the humeral shaft
The mechanism of injury is shown in Table 1. Patients with fractures due to low-energy trauma tended to be older women and those with high-energy fractures were younger men.
There were two open fractures, one type II and one type III according to the Gustilo system. Fourteen (13.2%) fractures were associated with multiple trauma, 12 were traffic accident-related and two were caused by falling down from a height (Table 2). Radial nerve palsy occurred in 12 patients (11.3%), there were five of AO/OTA type A1, four of type A3, one of type B1 and two of type B2. Most of the radial nerve injuries occurred in the middle shaft and the high-energy injury groups.
Multivariate logistic regression analysis showed that there was an increased risk of palsy of the radial nerve with fractures of the middle or distal shaft (Table 3).
The overall incidence of fractures of the shaft of the humerus was about 10 per 100,000 per year. The age-specific incidence shows a bi-modal age distribution, with one peak in the third decade and a second major peak in the eighth decade. The gender-specific distribution of males showed a single peak in the third decade, which mainly resulted from high-energy trauma. The incidence of humeral diaphyseal fracture drops after the fifth decade. In contrast, the female distribution presented increased incidence from the fifth decade. A single peak in the eighth decade was noted in the female distribution and the humeral shaft fractures were mostly due to simple falls (Fig. 2). The odds of the patient age being greater than 50 years old for women is seven times greater than that for men in humeral shaft fractures in our study (p<0.05).

Age- and gender-specific incidence of 106 fractures of the humeral shaft
Discussion
The epidemiological features of the humeral shaft fracture have been reported in European [6, 9] and African subjects [3], but they are not available in the Taiwanese or the Asian groups. Our results differed in the findings of the age, distribution, gender and mechanism of injury from previous reports [3, 6, 9].
The studies from Europe show a bi-modal age distribution with a minor peak in the third decade and consisting mainly of men resulting from high-energy trauma and a second major peak in the eighth decade, mostly women with osteoporotic fractures resulting from simple falls [6, 9]. Our result showed a single-peak distribution with a major peak in the third decade, as most young males suffered from high-energy trauma. Their studies reflect the relatively lower incidence of high-energy trauma in Sweden and the United Kingdom than in Asia. The difference may be due to the population structure of aging society in the European community and the greater labour force population in the Asian communities.
The age- and gender-specific distribution in our study also differed from the previous studies. Our study shows a bi-modal age-specific distribution with one peak in the third decade due to the majority of men resulting from high-energy trauma and another peak in the eighth decade with aged women resulting from low-energy trauma. In the previous studies, the age-specific incidence increased from the fifth decade and was highest in the eighth decade; this pattern was the same for the gender-specific incidence. We have the same figure for the combined female and male distribution at the fifth decade as the previous studies. However, the age-specific incidence of humeral diaphyseal fractures in females after the fifth decade gradually increases, as in the European group, but it drops in aged males.
The odds ratio reveals that aged women have seven times the risk of humeral shaft fracture than young women. This means that the influence of fracture due to post-menopause osteoporosis gradually increased in the Asian group, just as in the European group. But the impact of osteoporosis in males and females is different in our group, in which the incidence in aged males is not increased. The incidence of the male age-specific distribution of humeral shaft fractures in our group differing from the gradually increasing incidence of previous reports may be due to race/ethnic differences. Marshall et al. [4] have proved the feature of thicker cortices and higher trabecular bone mineral density (BMD), which increases bone strength, of the femoral shaft with quantitative computed tomography (QCT) in the aged male Black and Asian groups than in the Caucasian group. The data could explain the lower hip fracture rates in the aged male Asians than in the aged male Whites. Although there is a lack of direct evidence of increased BMD of the humeral shaft between the Asian and White groups, the different bone densities between the races may also explain the trend of increasing incidence in aged white males.
The singular study about the epidemiological picture of humeral fractures in Africans is documented by Igbigbi and Manda for Malawians [3]. They did not mention the age-gender distribution, but the males (60%) had a dominant percentage compared to the females (40%). Teenagers (13–19 years of age) comprised the majority of humeral shaft fractures (51.9%). This was followed by young adults (20–29 years of age), with an incidence of 29.2%.There was only a 10% incidence after the third decade.
The incidence of radial nerve injury is about 11% in our cases. The injury of the radial nerve mostly occurred in the middle third (50%) but was of the highest risk in the distal third of the humeral shaft. Our finding is in agreement with the results reported by Shao et al. [7]. They have systematically reviewed the published evidence. The overall prevalence of radial nerve palsy in fractures of the shaft of the humerus in 4,517 fractures was 11.8%. Fractures of the middle and middle-distal parts of the shaft had a significantly higher incidence. Transverse and spiral fractures were more likely to be associated with radial nerve palsy than oblique and comminuted patterns of fracture.
The associated injury in humeral shaft fracture is about 13.2% in our series; all of these 14 patients had multiple fractures. Most (12/14) resulted from motor vehicle collisions (MVC), which is the major cause of humeral shaft fracture in our group. Adili et al. [1] have shown that the presence of a humeral shaft fracture in a multiply injured patient involved in an MVC is significantly associated with an increased incidence of both upper and lower extremity fractures.
Functional bracing is considered to be the gold standard treatment for acute humeral shaft fractures, but there are still some caveats. The restriction of active abduction and elevation of the shoulder to avoid angular deformity would prolong rehabilitation time. Surgery is indicated in multiple fractures and fractures associated with substantial chest/head injuries, which are difficult to control with a sling and swathe. The young male labour population, who need an early return to work, is dominant in our group; moreover, the 13% of cases in this group combine multiple fractures or associated injury in our study. Internal fixation may be preferred in these situations. Closed intramedullary nailing is considered for fractures of osteopaenic bone, segmental or multiple traumas. However, new locked screw-plate fixation with a minimally invasive approach is now being used to avoid shoulder complications from intramedullary nailing. Minimally invasive plating osteosynthesis with locking plates may be the favoured choice in acute humeral shaft fractures in the future.
In conclusion, we have presented the epidemiology of humeral shaft fractures in the Asian population, especially in Taiwan, not previously reported. The differences highlighted in this study when compared to other populations underscore the importance of this study in our population. A larger epidemiological investigation of ethnological or country differences is needed for the adequate care of these fractures. The information may be used to facilitate the planning of training and resource management in our given population.
References
Adili A, Bhandari M, Sprague S et al (2002) Humeral shaft fractures as predictors of intra-abdominal injury in motor vehicle collision victims. Arch Orthop Trauma Surg 122(1):5–9
Gustilo RB, Anderson JT (1976) Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am 58:453–458
Igbigbi PS, Manda K (2004) Epidemiology of humeral fractures in Malawi. Int Orthop 28:338–341
Marshall LM, Zmuda JM, Chan BK et al (2008) Race and ethnic variation in proximal femur structure and BMD among older men. J Bone Miner Res 23(1):121–130
Orthopaedic Trauma Association (OTA) (1996) Fracture and dislocation compendium. OTA. Available online at: http://www.ota.org/compendium/humnew.pdf
Rose SH, Melton LJ 3rd, Morrey BF et al (1982) Epidemiologic features of humeral fractures. Clin Orthop Relat Res 168:24–30
Shao YC, Harwood P, Grotz MR et al (2005) Radial nerve palsy associated with fractures of the shaft of the humerus: a systematic review. J Bone Joint Surg Br 87:1647–1652
Taichung government population statistics. Available online at: http://www.tccg.gov.tw/sys/SM_theme?page=41448784
Tytherleigh-Strong G, Walls N, McQueen MM (1998) The epidemiology of humeral shaft fractures. J Bone Joint Surg Br 80:249–253
World Medical Association (2004) Declaration of Helsinki. WMADo. Available online at: http://www.wma.net/e/policy/b3.htm
Acknowledgement
We thank Dr. Tsai-Chung Li, Mr. Pao-Hsuan Lin and the China Medical University Biostatistics Center for their help with the statistical analyses carried out for this paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tsai, CH., Fong, YC., Chen, YH. et al. The epidemiology of traumatic humeral shaft fractures in Taiwan. International Orthopaedics (SICOT) 33, 463–467 (2009). https://doi.org/10.1007/s00264-008-0537-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-008-0537-8