
Abstract
Elbow stiffness is a common disorder, which restricts daily activities. Between 30° and 130° of elbow movement is usually enough to perform most daily activities. However, a 10° to 15° loss of elbow extension may be a problem when the patient is an athlete. From 1996 to 2004, 20 elbows of 20 patients (who were available for follow-up examination) were treated by lateral and medial release at Kocaeli University, for post-traumatic elbow contracture. Preoperative and the postoperative 12-month follow-up measurements were performed. The mean preoperative arc of motion was 35° and this value improved to 86.2°. The maximum improvement at the arc of motion was 105°. In an effort to understand the pathophysiology of the condition, surgical approaches may be used safely. The purpose of this study was to assess the functional outcome of the elbow joint after using a combination of lateral and medial approaches to treat elbow stiffness.
Résumé
La raideur du coude est une pathologie fréquente qui restreint les activités quotidiennes. Pour celles-ci une mobilité de 30° à 130° est largement suffisante. Cependant un flessum de 10° à 15° peut être un problème quand le patient est un athlète. Revue d’une série de 20 patients (20 coudes) opérés de 1996 à 2004 par libération interne et externe pour une raideur post-traumatique. Les mesures étaient faites avant l’opération et 12 mois après. L’amplitude articulaire pré-opératoire moyenne était de 35° et était augmenté à 86,2°. Le maximum de gain était 105°.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Capsular contracture of the elbow joint has been known as the main pathological feature of the stiff elbow for a long time [14].
Morrey classified elbow stiffness as either extrinsic or intrinsic [12]. Jupiter et al. [9] described six subgroups of simple elbow stiffness, which may be treated successfully by soft tissue releases alone. However, most of those patients had both extrinsic and intrinsic causes.
An appropriate approach to the stiff elbow should expose the elbow joint and the pathological structures fully. Nevertheless, the chosen approach must be able to restore extention easily.
Urbaniak et al. [15] and Gates et al. [4] reported good results for anterior capsulectomy performed through an anterior approach. Nevertheless, two separate skin incisions, postero-medial or medial and anterior, were used successfully by Itoh et al. [8]. In view of the more simple and safe approaches available, the anterior approach may not be the best option.
The posterior approach has gained wide acceptance for elbow arthroplasty over the years [2]. Although most parts of the joint may be in view with this approach, the anterior capsule is far away, and haematoma and wound healing problems are seen frequently. This is a useful approach when the posterior compartment needs to be debrided.
Husband and Hastings [7] and Mansat and Morrey [10] reported successful outcomes with the lateral approach. Wada et al. [17] reported the superiority of the medial approach in respect to both the anterior and lateral approaches.
Materials and methods
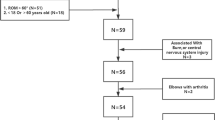
From 1996 to 2004, 20 elbows of 20 patients (who were available for follow-up examination) were treated by lateral and medial release at Kocaeli University, for post-traumatic contracture. The patients had an average age of 30 (range 8–77) years. There were nine female and 11 male patients; 11 left and nine right elbows. The aetiology was trauma; 11 had fallen from a height, six were traffic accidents, two machine compressions and one burn sequelae (Table 1).
Six of our patients had an associated injury.
The average time between the traumatic event and release was 6.8 (range 1–18) months. According to the classification of Kay, two of them were Type I, three were Type III and 15 Type IV. Eight patients had extrinsic, 12 had intrinsic causes.
During the operation, lateral release alone was sufficient to give a full range of motion in three patients. However, a medial release was added to the surgical procedure in the remaining patients. Anterior capsulectomy was performed in all patients.
Four patients suffered from recurrent stiffness and required a further operation. The mean interval from the time of the first operation to reoperation was 4.5 months.
Although no haemorrhage, haematoma or wound healing problems were encountered, three patients developed a postoperative infection which required debridement.
Passive range of motion (ROM) exercises were started on the first postoperative day. On the third postoperative day, continuous passive motion (CPM) exercises were added to the passive ROM exercises. During the hospital stay, both passive ROM and CPM exercises were maintained. When the patient was discharged from hospital, a home exercise program was used to prevent reccurrent stiffness.
We measured both preoperative and postoperative elbow movements manually with a goniometer. All patients used a custom-made splint in the postoperative period.
Results
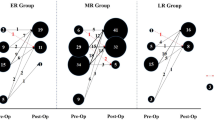
Preoperative and the postoperative 12-month follow-up measurements were performed. The mean preoperative arc of motion was 35° and this value improved to 86.2°. The maximum improvement at the arc of motion was 105°.
Three of the 20 elbows treated with a lateral release alone showed full ROM in the operating room. However, the remaining 17 patients required combined lateral and medial releases.
Four patients modified their jobs because of the insufficient elbow movements.
Postoperatively, the main complaint was periodical pain during daily activities, and cold intolerance was the next most common complaint. Additional complaints were transient paresthesia and restricted elbow motion. Three out of 20 patients had a transient ulnar paresthesia. Although seven patients had no complaint, other patients reported dissatisfaction when asked about postoperative satisfaction.
Discussion
A stiff elbow is usually defined as an elbow having a reduction of more than 30° in extension, or flexion less than 130° [11]. If the elbow has an arc of motion of 100°, from 30° to 130° of flexion, most activities of daily living are possible [11, 13].
Stiffness is a common problem after trauma to the elbow. Some conditions such as trauma to the elbow, burns, or coma may lead to impaired elbow functions. On the other hand, spinal cord injury, cerebral trauma, transplantation or prolonged artifical ventilation can lead to stiffness in an uninjured elbow [5]. Contracture of the elbow joint may be due to the intrinsic, extrinsic or combined pathology. More restriction at the joint and the necessity for difficult treatment modalities arise when the appropriate treatment is delayed. Boerboom et al. [1] reported that operative release within a year of the injury is twice as effective as the operation after a longer period. Early postoperative passive ROM exercises, followed by active ROM exercises, have a key role in the treatment.
Three articulations in a single joint capsule and the close relation of the joint surfaces may collude in the mechanism of the elbow stiffness.
Many techniques have been described for the operative release of a post-traumatic stiff elbow. Advocates of a lateral approach claim some advantages, such as less risk of nerve damage and wound problems [11]. This incision also permits evaluation and treatment of both the anterior and posterior trochlear and the radiohumeral joint. Ulnar paresthesia is the main complication seen after the release by lateral incision [3]. Because of this complication, anterior transposition of the ulnar nerve is suggested when symptoms persist.
Wada et al. [17] stated the benefits of the medial exposure and they found several advantages over the lateral approach. According to Wada et al. [17], pathological changes in the posterior oblique bundle of the medial collateral ligament, and anterior and posterior aspects of the elbow joint, can be seen via one medial incision. This incision allows a complete soft-tissue release and excision of loose bodies at the olecranon and coronoid fossae.
Preservation of the lateral collateral and annular ligaments is advocated by some authors to prevent elbow instability [6, 7, 16]. Although protection of the lateral collateral ligament was not attempted in our patients, instability at the elbow joint did not occur.
The arc of motion which was obtained at operation decreased rapidly in the early postoperative period. Elbow movements were reduced dramatically with the persistent postoperative rehabilitation. At the 1-year follow-up, the arc of motion was reduced near to the peroperative values, but not more.
Some patients may have a life-style which requires full elbow ROM which explains why our 17 patients stated dissatisfaction in the postoperative period, even though they had improved elbow ROM. The postoperative evaluation criterion should be the restoration of the daily activities, not patient satisfaction or reduction of elbow movements.
Various modalities are available for the treatment of the stiff elbow. However, there is no consensus as to which one is the most useful. We have used the combination of lateral and medial exposures to explore the whole circumference of the elbow for the resection of contracted structures. We have found similar results to those in the literature, but note that the best approach to the elbow joint is via the combined lateral and medial approach, which permits observation of all the contracted structures.
References
Boerboom AL, de Meyier HE, Verbung AD, Verhaar JA (1993) Arthrolysis for post-traumatic stiffness of the elbow. Int Orthop 17:346–349
Bryan RS, Morrey BF (1982) Extensive posterior exposure of the elbow: a triceps-sparing approach. Clin Orthop 166:188–192
Cohen MS, Hastings H II (1999) Operative release for elbow contracture; the lateral colateral sparing technique. Orthop Clin North Am 30:133–139
Gates HSD, Sullivan FL, Urbaniak JR (1992) Anterior capsulectomy and continuous passive motion in the treatment of post-traumatic flexion contracture of the elbow: a prospective study. J Bone Joint Surg Am 74:1229–1234
Gosling T, Blauth M, Lange T, Richter M, Bastian L, Krettek C (2004) Outcome assessment after arthrolysis of the elbow. Arch Orthop Trauma Surg 124:232–236
Hertel R, Pisan M, Lambert S, Ballmer F (1997) Operative management of the stiff elbow: squential arthrolysis based on a transhumeral approach. J Shoulder Elbow Surg 6:82–88
Husband JB, Hastings HD (1990) The lateral approach for operative release of post-traumatic contracture of the elbow. J Bone Joint Surg Am 72:1353–1358
Itoh Y, Saegusa K, Ishiguro T, Horiuchi Y, Sasaki T, Uchinishi K (1989) Operation for the stiff elbow. Int Orthop 13:263–268
Jupiter JB, O’Driscoll SW, Cohen MS (2003) The assessment and management of the stiff elbow. Instr Course Lect 52:93–111
Mansat P, Morrey BF (1998) The column procedure: a limited lateral approach for extrinsic contracture of the elbow. J Bone Joint Surg Am 80:1603–1615
Marti RK, Kerkhoffs GM, Maas M, Blankevoort L (2002) Progressive surgical release of a posttraumatic stiff elbow: technique and outcome after 2–18 years in 46 patients. Acta Orthop Scand 73:144–150
Morrey BF (1990) Post-traumatic contracture of the elbow: operative treatment, including distraction arthroplasty. J Bone Joint Surg Am 72:601–618
Morrey BF, Askew LJ, Chao EY (1981) A biomechanical study of normal functional elbow. J Bone Joint Surg Am 63:872–877
Tucker K (1978) Some aspects of post-traumatic elbow stiffness. Injury 9:216–220
Urbaniak JR, Hansen PE, Beissinger SF, Aitken MS (1985) Correction of post-traumatic flexion contracture of the elbow by anterior capsulectomy. J Bone Joint Surg Am 67:1160–1164
Viola RW, Hanel DP (1998) Early ‘simple’ release of posttraumatic elbow contracture associated with heterotropic ossification. J Hand Surg Am 24:370–380
Wada T, Ishii S, Usui M, Miyano S (2000) The medial approach for operative release of post-traumatic contracture of the elbow. J Bone Joint Surg Br 82:68–73
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was done at the Department of Orthopaedic Surgery and Traumatology, Kocaeli University.
Rights and permissions
About this article
Cite this article
Tosun, B., Gundes, H., Buluc, L. et al. The use of combined lateral and medial releases in the treatment of post-traumatic contracture of the elbow. International Orthopaedics (SICO 31, 635–638 (2007). https://doi.org/10.1007/s00264-006-0252-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-006-0252-2