
Abstract
Osteosarcoma, the most common type of primary malignant tumour that develops in bone, can be classified into several different sub-types. While the majority of osteosarcomas are highly malignant, there are some low-grade variants. Since the introduction of chemotherapy into the multi-modal treatment regimen of high-grade osteosarcoma, its prognosis has impressively improved, with long-term survival being achieved in two-thirds of all patients. This review summarises current chemotherapeutic treatment strategies in classical osteosarcoma and also addresses the indication for chemotherapy in more unusual types and variants. It emphasises the need for treatment in specialised centres and within prospective, multi-institutional trials, amongst which EURAMOS1 and EURO-B.O.S.S are currently active in many European countries.
Résumé
L’ostéosarcome est la tumeur osseuse la plus fréquente, cependant la plupart des ostéosarcomes ont une haute malignité, peu sont de malignité de bas de grade. Depuis l’utilisation de la chimio thérapie dans le traitement des ostéosarcomes de haute malignité, le pronostic a été très nettement amélioré, permettant une survie à long terme chez les deux tiers des patients. Cet article fait la revue des différentes stratégies thérapeutiques de chimiothérapie dans le traitement de l’ostéosarcome et de ses différents types. Il met en évidence que les traitements doivent être réalisés dans des centres spécialisés avec des études prospectives, multi sites, comme celles réalisées avec EURAMOS 1 et EURO-BOSS dans les pays européens.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteosarcoma, the most common type of primary malignant bone tumour, is defined by the presence of malignant mesenchymal cells producing osteoid or immature bone. The peak incidence of the most frequent type of osteosarcoma – high-grade central osteosarcoma – is in the second decade of life during the adolescent growth spurt. Untreated, osteosarcoma runs a relentless course with local and systemic disease progression and leads to death within a matter of months.
The inappropriate use of diagnostic tools and sub-optimal therapy can irrevocably compromise a patient’s chances of being cured. Therefore, affected patients should only be treated in specialised centres that are able to provide access to the full spectrum of care. In many countries, it is standard practice to provide such care within the framework of prospective clinical trials. Such trials have been essential in guaranteeing that as many patients as possible can benefit from modern, efficacious, interdisciplinary therapeutic regimens and in optimising these regimens. Every effort should be made to offer trial participation to all osteosarcoma patients.
Apart from several high-grade sub-types and entities, there are also several distinct low-grade variants of osteosarcoma. The critical role of surgery as the mode of local therapy in a curative approach needs to be stressed in all sub-types. Local treatment and chemotherapy are complementary components of treatment for high-grade tumours. This article focuses on the role of chemotherapy with an emphasis on the results of COSS, the German-Austrian-Swiss Cooperative Osteosarcoma Study Group.
High-grade central osteosarcoma
Indication for chemotherapy
High-grade central osteosarcoma is by far the most frequent sub-type, comprising up to 80% of all osteosarcomas. Prior to the introduction of chemotherapy in the 1970s, its prognosis – like that of all other high-grade variants – was dismal. Despite excellent local control rates with surgery, the vast majority of patients, even those with seemingly localised disease, rapidly developed pulmonary metastases and died. Accordingly, a renowned surgeon summarised the treatment results during a conference on bone sarcomas in the 1920s: “If you do not operate they die; if you do operate they die just the same” [7]. Such despondency is no longer justified, as prognosis has improved dramatically since the introduction of chemotherapy in the late 1970s. This was taken as sufficient proof of principle by most investigators. For those few who were still sceptical, a randomised trial between surgery plus postoperative chemotherapy and surgery only confirmed chemotherapy’s necessity and efficacy beyond any doubt [20].
Today, using a multi-modal approach consisting of preoperative (“neoadjuvant”) systemic polychemotherapy followed by local surgical therapy and then postoperative (“adjuvant”) chemotherapy, long-term, disease-free survival can be achieved in 60–70% of patients. Negative prognostic indicators include large tumour volume, axial site, primary metastases, increased alkaline phosphatase levels and a poor response to preoperative induction chemotherapy [3, 4]. The multi-modal treatment concept demands close interdisciplinary cooperation between orthopaedic surgeons, thoracic surgeons, radiologists, pathologists and oncologists. Early contact with an oncologist prior to biopsy is essential to ensure appropriate enrolment into clinical trials and participation in ancillary biological studies.
Roles of surgery and chemotherapy within multi-modal treatment
Complete surgery both of the primary tumour and, if present, all radiologically detectable metastases as well, is as much as a prerequisite for cure. The goals of surgery are to safely remove the tumour and yet preserve as much (extremity) function as possible. Local control is safely achieved by surgery with resection margins which are at least “wide” according to Enneking [8].
Microscopic sub-clinical metastases are present at the time of diagnosis in the majority of patients [3, 20]. The primary goal of chemotherapy within the multi-modal treatment concept is to eradicate these micrometastases. Chemotherapy alone is insufficient to reliably destroy either the primary tumour [17] or to eradicate clinically detectable metastases.
Timing of chemotherapy in relation to surgery
Chemotherapy can either be administered before (i.e. preoperative, induction or neoadjuvant chemotherapy) or after surgery (i.e. postoperative or adjuvant chemotherapy). Most current protocols employ chemotherapy both before and after surgery. The concern that delayed removal of the bulk tumour after neoadjuvant chemotherapy could compromise outcomes has not been substantiated. A prospective, randomised trial comparing immediate and delayed definitive surgery failed to detect effects on survival [13]. Similarly, neither the COSS-Group, in a large retrospective comparison of 157 patients with primary surgery and 1451 patients with preoperative chemotherapy [4], nor the Memorial Sloan-Kettering Cancer Center, who evaluated 279 patients treated either way [22], were able to detect survival differences between both approaches. Preoperative chemotherapy, however, offers several other advantages and is therefore the current standard. These advantages include:
-
1.
Gain of time in order to prepare definitive surgery for limb-salvage procedures.
-
2.
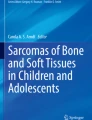
Delineation of tumour: chemotherapy induces the development of a well-formed avascular, collagenous capsule and contributes to the improvement of the quality and adequacy of the surgical margin. Osteosarcomas which are pre-treated by chemotherapy are better demarcated against surrounding tissues and easier to operate on [16]. Efficacious neoadjuvant chemotherapy is associated with reduced rates of local recurrence and can therefore make limb-salvage surgery safer [6, 26] (Fig. 1a,b).
Fig. 1 
Histology of osteosarcoma before (a) and after (b) preoperative chemotherapy (good response)
-
3.
Preoperative chemotherapy allows histological evaluation of the response to treatment, one of the most reliable prognostic indicators available to date [3]. Response is graded on the basis of the amount of remaining viable tumour in the resected specimen. A 10% cut-off is often used to discriminate between good and poor response. Sub-classifications into six (Salzer-Kuntschik) or four (Huvos) grades are currently practiced, allowing treatment effects to be described in more detail. In the COSS-trials, 5-year event-free survival in good responders was 68%, as compared to only 39% in poor responders [4] (Fig. 2).
Fig. 2 
Response to preoperative chemotherapy and survival. Grades 1 through 6 represent increasing tumour viability (reprinted from [3] with permission from the American Society of Clinical Oncology)


Surgery, chemotherapy and local control
Inadequate surgical margins and poor histological response are both important risk factors for local failure, the former being the more important. Local failure is about threefold more likely in patients with a poor response than in those with a good response, and nearly fivefold more likely in patients with inadequate surgical margins than in those with adequate ones [6, 26]. Both negative risk factors interact and, if simultaneously present, the risk for local failure increases excessively by a factor of almost 50 [26]. In view of the poor prognosis after local recurrence, reluctance to carry out limb-saving surgery – if not achievable with wide margins – is more than justified for poorly responding osteosarcoma [6].
Outline of current chemotherapy regimens
Chemotherapy for high-grade osteosarcoma is usually administered within prospective clinical trials. Its total duration is generally 6–12 months. Doxorubicin (=adriamycin) is an essential component of most regimens, but its use is limited by its potential for cardiotoxicity. Cisplatin, the second most commonly used drug, is included in most protocols, and high-dose methotrexate with leukovorin rescue is the third most commonly used agent in chemotherapy regimens [2, 3, 11, 21, 29]. High-dose methotrexate has the potential to cause severe, life-threatening toxicity, but it is generally well tolerated in young patients, provided that renal function is normal and that hyper-hydration, alkalinisation, close plasma level monitoring and adequate administration of the antidote leucovorine are guaranteed.
The benefit of adding ifosfamide, the fourth agent generally accepted as being active against the disease, to regimens of doxorubicin, cisplatin and high-dose methotrexate remains to be confirmed. The Italian and Scandinavian groups [2, 29] as well as our own COSS-group [11] have used all four drugs together with promising results. However, the addition of ifosfamide did not result in a survival advantage in a large, randomised North American study [21].
Salvage therapy for poor responders?
As mentioned above, a poor histological response to preoperative chemotherapy is associated with a markedly inferior prognosis. To date, attempts to modify postoperative chemotherapy based on response (“salvage chemotherapy”) have not resulted in convincingly improved outcomes. Controlled, randomised trials addressing this problem had not been performed until the European and American Osteosarcoma Study EURAMOS1 opened for recruitment early in 2005. Centres in Europe and North America are strongly encouraged to participate in this multi-national, transatlantic, intergroup study (Fig. 3a), which – in addition to addressing the salvage question – evaluates the value of interferon α maintenance therapy.

Outline of the chemotherapy regimens used in the current multi-centre trials EURAMOS1 (a) and EURO-B.O.S.S. (b). See text for details
Chemotherapy in older patients
Most patients with high-grade osteosarcoma are adolescents or young adults, and prospective studies have generally excluded patients over the age of 40 years. Reports dealing with older patients are few and limited to retrospective series. The impression that older patients fare less well may be in part attributable to the increasing proportion of unfavourable axial lesions with increasing age rather than to age itself [4]. A European review of outcomes came to the result that osteosarcoma in older patients is a curable condition and warrants intensive treatment with chemotherapy and surgical resection [15]. The Italian (ISG) and Scandinavian (SSG) Sarcoma Groups together with COSS have therefore developed a joint protocol for 41- to 65-year olds. This prospective European Bone Over 40 Sarcoma Study (EURO-B.O.S.S, Fig. 3b) offers multi-modal, age-adapted therapy based on pre- and postoperative doxorubicin, cisplatin and ifosfamide not only for osteosarcoma, but also for other high-grade spindle cell sarcomas of the bone, such as malignant fibrous histiocytoma (MFH), leiomyosarcoma, fibrosarcoma, dedifferentiated chondrosarcoma and angiosarcoma. The use of high-dose methotrexate, which may be associated with increased toxicity in older patients, is restricted to patients with an extremely poor histological response to preoperative chemotherapy and to a dose of 8 g/m2 (compared to 12 g/m2 in younger patients).
Chemotherapy in relapsed osteosarcoma
At present, there is no standard chemotherapy regimen for osteosarcoma which relapses following multi-modal first-line treatment. Prognosis is poor, with long-term post-relapse survival in less than 20% of the patients [9, 18]. However, there might be a second or sometimes even a third, fourth, or later chance, provided all metastases can be removed by surgery. Data from Italy [9] and the COSS-group [18] suggest a limited prolongation of survival with second-line multi-agent chemotherapy in patients with incompletely resected metastases. The adjuvant effect of second-line chemotherapy in patients with a second complete surgical remission is not as obvious, even though a limited benefit was observed in selected retrospective series [18, 27].
Complications of chemotherapy
The most frequent chemotherapy-related complications include infections associated with myelosuppression, mucositis, impaired renal function (tubular damage due to ifosfamide and glomerular dysfunction caused by cisplatin), hypomagnesaemia, hearing loss, gonadal dysfunction and anthracycline-induced cardiac dysfunction. Close monitoring during chemotherapy is mandatory in order to appropriately detect and adapt the relevant agents. Long-term follow-up is required not only to monitor the remission status but also in order to screen for and manage late effects occurring following completion of the chemotherapy regimen [19]. Strategies to reduce cardiotoxicity include continuous-infusion doxorubicin and the use of cardioprotective agents. The ongoing challenge is to further reduce late effects without compromising the efficacy of antineoplastic treatment.
Osteosarcoma variants
Several variants of osteosarcoma are distinguished from classical or conventional osteosarcoma because of differences in site, histology or biological behaviour [10].
Small cell osteosarcoma
This very rare form of osteosarcoma (1.3%) is a tumour that resembles Ewing’s sarcoma histologically but produces an osteoid matrix. It responds to treatment based on protocols for osteosarcoma [23].
Osteosarcoma occurring as secondary malignancy
Osteosarcoma arising as a secondary malignancy has historically been associated with a particularly grave prognosis. However, recent reports from France [30] as well as those from our COSS group [5] have demonstrated that affected patients may survive with complete surgery and polychemotherapy, which, of course, needs to take into account previous chemotherapy exposure. Secondary osteosarcomas remain a particular challenge for the orthopaedic surgeon, as they often arise in unfavourable axial sites.
Extraskeletal (=extraosseous) osteosarcoma
These osteoid-producing tumours that originate in other organs than bones are usually high-grade malignancies. They are rare (<5% of osteosarcoma) and uncommon under the age of 30. While some authors have reported poor results with doxorubicin/cisplatin-based regimens [1], COSS found that a treatment approach analogous to that pursued in conventional high-grade osteosarcoma led to favourable outcomes [12].
Surface osteosarcomas
A small proportion of osteosarcomas arises not intramedullarly but from the surface of bone. The World Health Organisation classification [10] now recognises three main sub-types of surface osteosarcoma: parosteal, periosteal and high-grade surface. Parosteal osteosarcomas are usually low-grade malignancies and are characterised by a tendency for local recurrence rather than for distant metastatic spread. Complete surgical resection with “wide margins” should be attempted. The indication for chemotherapy is limited to tumours which transform into high-grade malignancies (as is not so rarely the case after repeated local recurrences) and to cases with metastatic spread. Periostal osteosarcoma is considered to be an intermediate-grade tumour. Complete surgical resection is essential, but the role of chemotherapy remains uncertain [14]. High-grade surface osteosarcomas behave – and are therefore treated like – high-grade central tumours [24].
Craniofacial osteosarcoma
Complete surgical resection, the mainstay of treatment, might be particularly difficult to achieve in this anatomic location. With the exception of tumours of the skull, the metastatic rate of craniofacial osteosarcoma is lower in other sites. While a systematic review suggested a benefit from adjuvant chemotherapy [28], its exact role and indication remains under discussion.
Low-grade central osteosarcoma
This seems to represent the central counterpart of parosteal osteosarcoma arising in the medullary cavity of the bone. The same treatment principles as for parosteal osteosarcoma apply.
Other high-grade spindle cell sarcomas of bone
Due to their rarity, treatment of high-grade, non-osteogenic spindle cell sarcomas of the bone (see EURO-B.O.S.S., see above) remains largely individualised. A biological behaviour and chemosensitivity similar to those of high-grade osteosarcoma has been reported for some of these tumours, MFH in particular [25, 31]. Such similarities are suggestive that high-grade, non-osteogenic spindle cell sarcomas of the bone should respond to multi-agent chemotherapy as has been established for osteosarcoma. In order to evaluate the effect of such chemotherapy on outcome, the EURO-B.O.S.S -protocol includes these entities.
Conclusions
Multi-drug chemotherapy has a strong positive impact on disease-free survival in patients with osteosarcoma. Ongoing challenges include tailoring chemotherapy to the individual risk of relapse and the development of biologically driven treatment strategies.
References
Ahmad SA, Patel SR, Ballo MT, Baker TP, Yasko AW, Wang X, Feig BW, Hunt KK, Lin PP, Weber KL, Chen LL, Zagars GK, Pollock RE, Benjamin RS, Pisters PW (2002) Extraosseous osteosarcoma: response to treatment and long-term outcome. J Clin Oncol 20:521–527
Bacci G, Ferrari S, Longhi A, Picci P, Mercuri M, Alvegard TA, Saeter G, Donati D, Manfrini M, Lari S, Briccoli A, Forni C, Italian Sarcoma Group/Scandinavian Sarcoma Group (2002) High dose ifosfamide in combination with high dose methotrexate, adriamycin and cisplatin in the neoadjuvant treatment of extremity osteosarcoma: preliminary results of an Italian Sarcoma Group/Scandinavian Sarcoma Group pilot study. J Chemother 14:198–206
Bielack SS, Kempf-Bielack B, Winkler K (1996) Osteosarcoma: relationship of response to preoperative chemotherapy and type of surgery to local recurrence. J Clin Oncol 14:683–684
Bielack SS, Kempf-Bielack B, Heise U, Schwenzer D, Winkler K (1999) Combined modality treatment for osteosarcoma occurring as a second malignant disease. Cooperative German-Austrian-Swiss Osteosarcoma Study Group. J Clin Oncol 17:1164–1174
Bielack SS, Kempf-Bielack B, Delling G, Exner GU, Flege S, Helmke K, Kotz R, Salzer-Kuntschik M, Werner M, Winkelmann W, Zoubek A, Jurgens H, Winkler K (2002) Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 20:776–790
Bielack SS, Machatschek JN, Flege S, Jurgens H (2004) Delaying surgery with chemotherapy for osteosarcoma of the extremities. Expert Opin Pharmacother 5:1243–1256
Cade S (1955) Osteogenic sarcoma; a study based on 133 patients. J Roy Coll Surg Edin 1:79–111
Enneking WF, Spanier SS, Goodman MA (1980) A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res 153:106–120
Ferrari S, Briccoli A, Mercuri M, Bertoni F, Picci P, Tienghi A, Del Prever AB, Fagioli F, Comandone A, Bacci G (2003) Postrelapse survival in osteosarcoma of the extremities: prognostic factors for long-term survival. J Clin Oncol 21:710–715
Fletcher CDM, Unni KK, Mertens F (eds) (2002) WHO classification of tumours pathology and genetics of tumours of soft tissue and bone. IARC Press, Lyon
Fuchs N, Bielack SS, Epler D, Bieling P, Delling G, Korholz D, Graf N, Heise U, Jurgens H, Kotz R, Salzer-Kuntschik M, Weinel P, Werner M, Winkler K (1998) Long-term results of the co-operative German-Austrian-Swiss osteosarcoma study group’s protocol COSS-86 of intensive multidrug chemotherapy and surgery for osteosarcoma of the limbs. Ann Oncol 9:893–899
Goldstein-Jackson SY, Gosheger G, Delling G, Berdel WE, Exner GU, Jundt G, Machatschek JN, Zoubek A, Jurgens H, Bielack SS, Cooperative Osteosarcoma Study Group COSS (2005) Extraskeletal osteosarcoma has a favourable prognosis when treated like conventional osteosarcoma. J Cancer Res Clin Oncol 131:520–526
Goorin AM, Schwartzentruber DJ, Devidas M, Gebhardt MC, Ayala AG, Harris MB, Helman LJ, Grier HE, Link MP, Pediatric Oncology Group (2003). Presurgical chemotherapy compared with immediate surgery and adjuvant chemotherapy for nonmetastatic osteosarcoma: Pediatric Oncology Group Study POG-8651. J Clin Oncol 21:1574–1580
Grimer RJ, Bielack S, Flege S, Cannon SR, Foleras G, Andreeff I, Sokolov T, Taminiau A, Dominkus M, San-Julian M, Kollender Y, Gosheger G, European Musculo Skeletal Oncology Society (2005) Periosteal osteosarcoma – a European review of outcome. Eur J Cancer 41:2806–2811
Grimer RJ, Cannon SR, Taminiau AM, Bielack S, Kempf-Bielack B, Windhager R, Dominkus M, Saeter G, Bauer H, Meller I, Szendroi M, Folleras G, San-Julian M, van der Eijken J (2003) Osteosarcoma over the age of forty. Eur J Cancer 39:157–163
Hosalkar HS, Dormans JP (2004) Limb sparing surgery for pediatric musculoskeletal tumors. Pediatr Blood Cancer 42:295–310
Jaffe N, Carrasco H, Raymond K, Ayala A, Eftekhari F (2002) Can cure in patients with osteosarcoma be achieved exclusively with chemotherapy and abrogation of surgery? Cancer 95:2202–2210
Kempf-Bielack B, Bielack SS, Jurgens H, Branscheid D, Berdel WE, Exner GU, Gobel U, Helmke K, Jundt G, Kabisch H, Kevric M, Klingebiel T, Kotz R, Maas R, Schwarz R, Semik M, Treuner J, Zoubek A, Winkler K (2005) Osteosarcoma relapse after combined modality therapy: an analysis of unselected patients in the Cooperative Osteosarcoma Study Group (COSS). J Clin Oncol 23:559–568
Langer T, Stohr W, Paulides M, Kremers A, Dorr HG, Gobel U, Beck JD (2005) Prospective multicenter registration of major late sequelae in sarcoma patients using the Late Effects Surveillance System (LESS). Klin Pediatr 217:176–181
Link MP, Goorin AM, Miser AW, Green AA, Pratt CB, Belasco JB, Pritchard J, Malpas JS, Baker AR, Kirkpatrick JA et al (1986) The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 314:1600–1606
Meyers PA, Heller G, Healey J, Huvos A, Lane J, Marcove R, Applewhite A, Vlamis V, Rosen G (1992) Chemotherapy for nonmetastatic osteogenic sarcoma: the Memorial Sloan-Kettering experience. J Clin Oncol 10:5–15
Meyers PA, Schwartz CL, Krailo M, Kleinerman ES, Betcher D, Bernstein ML, Conrad E, Ferguson W, Gebhardt M, Goorin AM, Harris MB, Healey J, Huvos A, Link M, Montebello J, Nadel H, Nieder M, Sato J, Siegal G, Weiner M, Wells R, Wold L, Womer R, Grier H (2005) Osteosarcoma: a randomized, prospective trial of the addition of ifosfamide and/or muramyl tripeptide to cisplatin, doxorubicin, and high-dose methotrexate. J Clin Oncol 23:2004–2011
Nakajima H, Sim FH, Bond JR, Unni KK (1997) Small cell osteosarcoma of bone. Review of 72 cases. Cancer 79:2095–2106
Okada K, Unni KK, Swee RG, Sim FH (1999) High grade surface osteosarcoma: a clinicopathologic study of 46 cases. Cancer 85:1044–1054
Picci P, Bacci G, Ferrari S, Mercuri M (1997) Neoadjuvant chemotherapy in malignant fibrous histiocytoma of bone and in osteosarcoma located in the extremities: analogies and differences between the two tumors. Ann Oncol 8:1107–1115
Picci P, Sangiorgi L, Rougraff BT, Neff JR, Casadei R, Campanacci M (1994) Relationship of chemotherapy-induced necrosis and surgical margins to local recurrence in osteosarcoma. J Clin Oncol 12:2699–2705
Saeter G, Hoie J, Stenwig AE, Johansson AK, Hannisdal E, Solheim OP (1995) Systemic relapse of patients with osteogenic sarcoma. Prognostic factors for long term survival. Cancer 75:1084–1093
Smeele LE, Kostense PJ, van der Waal I, Snow GB (1997) Effect of chemotherapy on survival of craniofacial osteosarcoma: a systematic review of 201 patients. J Clin Oncol 15:363–367
Smeland S, Wiebe T, Bohling T, Brosjo O, Jonsson K, Alvegard TA (2004) Chemotherapy in osteosarcoma. The Scandinavian Sarcoma Group experience. Acta Orthop Scand Suppl 75:92–98
Tabone MD, Terrier P, Pacquement H, Brunat-Mentigny M, Schmitt C, Babin-Boilletot A, Mahmoud HH, Kalifa C (1999) Outcome of radiation-related osteosarcoma after treatment of childhood and adolescent cancer: a study of 23 cases. J Clin Oncol 17:2789–2795
Waddell AE, Davis AM, Ahn H, Wunder JS, Blackstein ME, Bell RS (1999) Doxorubicin-cisplatin chemotherapy for high-grade nonosteogenic sarcoma of bone. Comparison of treatment and control groups. Can J Surg 42:190–199
Acknowledgements
The authors thank Prof. Dr. Gernot Jundt, Basel, for providing the photomicrographs of histological sections for Fig. 1, and Lynn Hazelwood for language assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Carrle, D., Bielack, S.S. Current strategies of chemotherapy in osteosarcoma. International Orthopaedics (SICOT) 30, 445–451 (2006). https://doi.org/10.1007/s00264-006-0192-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-006-0192-x