
Abstract
The focus of this work was to study the serum interleukin-6 (IL-6) response to total hip replacement. Twenty-one patients received an uncemented total hip prosthesis. Venous samples for IL-6 determination were drawn before and after surgery. The IL-6 response was significant, and a peculiar heterogeneity of response was apparent: the medians of peak levels (82.3 pg/ml) and of areas under the response curve (51.8 pg/ml) distinguished between IL-6 high responders (HR) and IL-6 low responders (LR; p<0.0001). No difference was found in the gender composition of these groups, whereas the HR patients were older than the LR patients (p<0.05). The amount of IL-6 increase was found to correlate with patient age, whereas its slope was found to correlate with the duration of the surgical procedure. Moreover, the HR group presented a higher degree of hyperthermia in the days after surgery compared with the LR patients, without evidence of differences in postoperative complications, time to mobilisation, or length of stay in hospital. The main finding of our study was the evidence of a remarkable variability between individuals in the IL-6 response to surgery. Future studies are needed to identify the factors involved in the regulation of the cytokine response to surgery.
Résumé
Etude de la réponse de l’interleukine-6 (IL-6) du sérum à la prothèse totale de hanche. Vingt et un patients ont eu une prothèse totale non cimentée et des échantillons veineux ont été prélevés avant et après la chirugie. La réponse était significative avec une hétérogenéité apparente: le pic médian (82,3 pg/ml) et la zone située sous la courbe (AUC: 51,8 pg/ml) distinguaient entre les «IL-6 fort répondeurs» (HR) et les «IL-6 faibles répondeurs» (LR; p<0,0001). Il n’y avait pas de différence selon le sexe mais les patients HR étaient plus agés que les patients LR (p<0,05). Le niveau de l’IL-6 était en rapport avec l’age des patients tandis que son augmentation était en rapport avec la durée de l’acte chirurgical. Le groupe HR avait un plus grand degré d’hyperthermie post opératoire que le groupe LR sans différence dans les complications, le délai de mobilisation et la durée d’hospitalisation. Le fait principal était la variabilité inter individuelle dans la réponse de l’interleukine-6 à la chirurgie. Des études sont nécessaires pour caractériser les facteurs qui interviennent dans la réponse des cytokines à la chirurgie.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Recent studies have demonstrated that elective orthopedic surgery significantly elevates serum levels of interleukin-6 (IL-6) [1, 5, 7, 10, 11, 13, 16, 18–19]; in these circumstances, IL-6 rises rapidly in serum after the incision, peaking at 8–24 h. This increase has been attributed to the release of IL-6 from immunocompetent cells in the wound region [13, 16], and it was found to significantly correlate with surgical trauma as defined by operation length and the volume of blood loss during surgery [13].
Local and systemic inflammatory responses during and after surgery are important in the development of postoperative complications and in the general restitution [15]. Few studies have addressed the relationships between inflammatory response to elective orthopedic surgery and several possible determinant factors such as age, gender, lifestyle factors, severity of the pathological status, and duration of the intervention [12].
The focus of this work was to study the IL-6 response to elective total hip replacement surgery, with the following objectives: 1) to identify accurate parameters for evaluating the serum IL-6 response to surgery, 2) to quantify the serum response in a group of patients of different gender and age, 3) to characterize modulator factors of this response, and 4) to evaluate the relationships between IL-6 response and the clinical course in hospital.
Materials and methods
Subjects
The study population consisted of 21 consecutive patients (14 female, 7 male) who received a total hip prosthesis for primary osteoarthritis.
A postero-lateral surgical approach was used for all implants, with the surgical procedure aiming to obtain the maximum proximal interference press-fit. The implanted components were the Alloclassic stem and the Fitmore socket (Centerpulse, Winterthur, Switzerland).
To rule out the possible confounding effects of circadian variability, all patients were operated on between 0800 and 1100. Seventeen patients had general anaesthesia, and four had spinal anaesthesia, depending on patient and anaesthetist preference. The anaesthetic team was not involved in the study, and the choice of anaesthesia type was not influenced by the study.
Analgesic medication with nonsteroidal antiinflammatory drugs was avoided before and after the intervention, and only opioid agents were administered to treat pain.
The patients were thoroughly informed about the purposes and procedures of the study before they gave written consent. The study conformed to the guidelines in the Declaration of Helsinki and was approved by the regional ethics committee.
WOMAC and blood samples
The Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index was used to assess self-reported physical function, pain, and stiffness before the surgical procedure [4]. Samples of venous blood for IL-6 determination were drawn before surgery (PRE), and eight and 24 h after the incision, and at hospital discharge. Haemoglobin levels and leucocyte counts with differential were evaluated before surgery and once daily after the operation, and body temperature was monitored twice daily during the whole period in hospital.
Assays
Serum IL-6 concentrations were measured by commercially available ELISA (Quantikine Human IL-6 Immunoassay, R&D Systems, Abingdon, UK) according to the manufacturer’s instructions. The dynamic range was 3.12–300 pg/ml; the minimum detectable concentration (MDC) was <1 pg/ml. Values between the low standard and the MDC were extrapolated, and values below the MDC were posed as equal to 1/2 MDC. The ELISA readings were performed by a Microreader Instrument Elx808-I (Bio-Tek Instruments, Winooski, VT, USA), and the absorbance was measured at 450 and 570 nm.
Sera were immediately separated and stored at −20°C until assayed. All samples from any subject were processed in duplicate in the same assay session.
Leucocyte counts with differential and haemoglobin levels were analysed with an automated Cell-Dyn 4000 series analyser (Abbott Diagnostics Laboratories, Abbott Park, IL, USA).
Intra- and interassay coefficients of variation for all the above-mentioned assays were below 6% and 8%, respectively.
Statistical analysis
Normal distribution of the data was tested by the Shapiro-Wilk test. Because data were not normally distributed, nonparametric tests were used. The Friedman’s ANOVA was used to determine whether there were any significant differences over time among the samples. If a significant difference was present, a Dunn’s post hoc test was used to locate the difference, and the area under the response curve (AUC) was calculated for the day of intervention (three samples) according to the trapezoid method.
The slope of the rise was calculated for serum IL-6 by regressing the samples among the baseline (presurgery) and the peak response and using the slope of the line as the outcome variable, indicated as SLOPE rise. The slope of the recovery was calculated for serum IL-6 by regressing the samples among the peak response and the last sample (discharge) and using the slope of the line as the outcome variable, indicated as SLOPE rec.
For continuous variables, the comparisons between different subgroups were analysed by means of the nonparametric Mann-Whitney U-test applied to the raw data for each sample, to the AUCs and to the slope values; for categorical variables, differences were analysed by means of the Fisher’s exact test. The Spearman rank correlation analysis assessed the relationships among IL-6 response, clinical characteristics, and surgical parameters.
Statistical analysis was performed with the Statistica 6 for Windows (Statsoft, Tulsa, OK, USA) software package. All values are reported as mean ± SD. Statistical significance was set at p<0.05.
Results
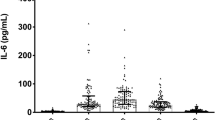
In the entire group of patients, the IL-6 response was significant, and mean peak level was reached 24 h after surgery (Table 1 and Fig. 1).

Serum IL-6 values for each sample are depicted for the two groups (IL-6 high responders=filled diamond; IL-6 low responders=empty circle). Statistically significant differences between the two groups are highlighted (*=p<0.05; **=p<0.01). The differences in peak levels, AUC, SLOPE rise, and SLOPE rec are depicted for HR and LR (*=p<0.05; **=p<0.01; ***=p<0.0001). Values are represented as means ± SD
The median both of the peak levels (82.3 pg/ml) and of the AUCs (51.8 pg/ml/die) determined two groups (p<0.0001): IL-6 high responders (HR, n=9) and IL-6 low responders (LR, n=10; Table 2). Two patients were excluded because they presented, respectively, peak levels above and AUC values equal to the respective medians (case 8 in Table 1) and AUC values above and peak levels equal to the respective medians (case 12 in Table 1).
No differences were found in smoking habits (HR, two smokers and seven nonsmokers vs. LR, four smokers and six nonsmokers, p=not significant) or in the gender composition of these two groups (HR, six women and three men vs. LR, six women and four men, p=not significant). The HR patients were found to be older than the LR patients (HR, 65.5±7.6 years vs. LR, 55.7±11.4 years, p<0.05), and the correlation analysis consistently showed positive relationships between age and both IL-6 peak and AUC values (Fig. 2). Moreover, a positive relationship was found between duration of surgery and SLOPErise (Fig. 2), whereas no correlations were found either among all the factors considered and the SLOPE rec or among WOMAC test scores and parameters of IL-6 response.

Linear correlations between age and IL-6 peak levels (panel A: r=0.53, p=0.016), age and IL-6 AUC (panel B: r=0.57, p=0.007),and duration of surgery and SLOPE rise (panel C: r=0.56, p=0.010) in the whole group of 21 patients
The patients presented moderate hyperthermia in the days after surgery, with evidence of difference in peak levels between HR and LR (HR, 38.2±0.4°C vs. LR, 37.8±0.2°C, p<0.05). However, no patient had a documented infection, and no differences were observed between HR and LR either in drop in haemoglobin levels (HR, −33.8±5.7% vs. LR, −35.9±9.6%, p=not significant) or in units of blood transfused after surgery (HR, 1.0±1.0 vs. LR, 0.9±1.0, p=not significant). Moreover, no differences between the two groups were found in the percentages of maximum increase in white blood cells (HR, 99.4±33.5% vs. LR, 98.4±59.9%, p=not significant) or neutrophils (HR, 189.1±53.1% vs. LR, 184.6±83.0%, p=not significant).
All patients were mobile by the third post-operative day, and no significant difference in length of hospital stay was apparent between the two groups (HR, 7.1±1.1 days vs. LR, 6.8±1.4 days, p=not significant).
Discussion
The main finding of this study was evidence of a remarkable variability between individuals in the serum IL-6 response to the elective orthopedic surgery. Several possible explanations of different inflammatory responses to similar traumatic insults deserve attention.
Even though the surgical procedure was performed in the most reproducible way by three experienced surgeons, an obvious variability in the local anatomy and in the anatomical characteristics of the disease was found. These differences could imply variable amounts of tissue dissection and damage, affecting the degree of local and systemic inflammatory responses.
Our data do not confirm that the duration of the intervention can be considered among the determinants of degree, but only of dynamics of the IL-6 increase. Also, the degree of morbidity, as indirectly evaluated on the basis of the WOMAC test scores, was not found to be related to the IL-6 response.
In accordance with the well-defined association between aging and increased levels of circulating cytokines [9], patient age was the most important factor involved in regulation of the inflammatory reaction to surgery. The possible explanation for this finding lies in the reduced adrenocortical responsiveness to surgical stress that is characteristic of aged individuals [2, 3]; the glucocorticoids released by the adrenal glands, inhibit the production of IL-6 [17]. Indeed, Hogevold et al. found that the IL-6 response to surgical trauma was attenuated by exogenous glucocorticoids [7].
The only clinical difference we observed between HR and LR patients was a higher degree of postoperative hyperthermia in the HR group. Because Kennedy et al. reported an increased risk of fever with blood transfusion and decreased haemoglobin [8], we also compared the HR and LR groups for units of blood transfused after surgery and drop in haemoglobin levels, but found no evidence of differences between the two groups. Furthermore, no differences between the two groups were observed in the percentages of maximum change of white blood cells and neutrophil count; this observation could be viewed as confirmation that IL-6 serum levels represent one of the most reliable markers for systemic inflammation, as recently highlighted by Giannoudis et al. [6].
Our conclusions can be summarised as follows: 1) IL-6 peak level, AUC calculated for the day of intervention, and slope of the postoperative rise were found to be the most informative parameters for quantifying the amount and dynamics of the serum IL-6 response, 2) elective orthopaedic surgery elicited a significant serum IL-6 response 24 h after the intervention, 3) the IL-6 increase was found to be related to patient age, while its slope was found to correlate with the duration of the surgical procedure, and 4) the HR group presented a higher degree of hyperthermia in the days after operation compared with the LR patients.
References
Andres BM, Taub DD, Gurkan I, Wenz JF (2003) Postoperative fever after total knee arthroplasty: the role of cytokines. Clin Orthop 415:221–231
Arnetz BB (1985) Endocrine reactions during standardized surgical stress: the effects of age and methods of anaesthesia. Age Ageing 14:96–101
Beale E, Zhu J, Belzberg H (2002) Changes in serum cortisol with age in critically ill patients. Gerontology 48:84–92
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW (1988) Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 15:1833–1840
Cruickshank AM, Fraser WD, Burns HJ, Van Damme J, Shenkin A (1990) Response of serum interleukin-6 in patients undergoing elective surgery of varying severity. Clin Sci (Lond) 79:161–165
Giannoudis PV, Hildebrand F, Pape HC (2004) Inflammatory serum markers in patients with multiple trauma. Can they predict outcome? J Bone Joint Surg Br 86:313–323
Hogevold HE, Kierulf P, Ovstebo R, Reikeras O (1992) Acute phase reactants and interleukin 6 after total hip replacement. Effects of high dose corticosteroids. Eur J Surg 158:339–345
Kennedy JG, Rodgers WB, Zurakowski D, Sullivan R, Griffin D, Beardsley W, Sheehan L (1997) Pyrexia after total knee replacement. A cause for concern? Am J Orthop 26:549–552
Krabbe KS, Pedersen M, Bruunsgaard H (2004) Inflammatory mediators in the elderly. Exp Gerontol 39:687–699
Krohn CD, Reikeras O, Aasen AO (1999) The cytokines IL-1beta and IL-1 receptor antagonist, IL-2 and IL-2 soluble receptor-alpha, IL-6 and IL-6 soluble receptor, TNF-alpha and TNF soluble receptor I, and IL10 in drained and systemic blood after major orthopaedic surgery. Eur J Surg 165:101–109
Krohn CD, Reikeras O, Mollnes TE, Aasen AO (1998) Complement activation and release of interleukin-6 and tumour necrosis factor-alpha in drained and systemic blood after major orthopaedic surgery. Eur J Surg 164:103–108
Menger MD, Vollmar B (2004) Surgical trauma: hyperinflammation versus immunosuppression? Langenbecks Arch Surg 389:475–484
Sakamoto K, Arakawa H, Mita S, Ishiko T, Ikei S, Egami H, Hisano S, Ogawa M (1994) Elevation of circulating interleukin 6 after surgery: factors influencing the serum level. Cytokine 6:181–186
Sehgal PB (1992) Regulation of IL6 gene expression. Res Immunol 143:724–734
Singer M, De Santis V, Vitale D, Jeffcoate W (2004) Multiorgan failure is an adaptive, endocrine-mediated, metabolic response to overwhelming systemic inflammation. Lancet 364:545–548
van Deuren M, Twickler TB, de Waal Malefyt MC, Van Beem H, van der Ven-Jongekrijg J, Verschueren CM, van der Meer JW (1998) Elective orthopedic surgery, a model for the study of cytokine activation and regulation. Cytokine 10:897–903
Vgontzas AN, Papanicolaou DA, Bixler EO, Lotsikas A, Zachman K, Kales A, Prolo P, Wong ML, Licinio J, Gold PW, Hermida RC, Mastorakos G, Chrousos GP (1999) Circadian interleukin-6 secretion and quantity and depth of sleep. J Clin Endocrinol Metab 84:2603–2607
Wilson KW, Wilson MR, McGlasson DL (1993) Serum endotoxin, tumor necrosis factor, and interleukin-6 response to total hip arthroplasty. Mil Med 158:712–716
Wirtz DC, Heller KD, Miltner O, Zilkens KW, Wolff JM (2000) Interleukin-6: a potential inflammatory marker after total joint replacement. Int Orthop 24:194–196
Acknowledgement
We wish to thank Dr. Roberto Pedrola for his assistance in sample collection.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Minetto, M.A., Oprandi, G., Saba, L. et al. Serum interleukin-6 response to elective total hip replacement surgery. International Orthopaedics (SICO 30, 172–176 (2006). https://doi.org/10.1007/s00264-006-0073-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-006-0073-3