
Abstract
Between September 2000 and February 2002 we inserted 120 total knee arthroplasties. In 60 patients we used the standard technique, and in 60 patients we used the OrthoPilot navigation system. Postoperatively all patients had standing long radiographs of the lower extremity from the hip joint to the ankle. We considered the ideal value of the anatomic lateral tibiofemoral angle (LTFA) to be 174°. In the standard group the mean value of LTFA was 174.9° and in the navigation group 174.3°. A deviation between 0° and 2° from the ideal value was seen in 42 cases in the standard group and in 53 cases in the navigation group. In the standard group 18 cases had a deviation of more than 2.1°, whereas there were only seven cases in the navigation group with a deviation exceeding 2.1°. There were no complications related to the use of the navigation system. The system affords a possibility to place femoral and tibial components precisely with less axis deviation than with the conventional technique.
Résumé
Entre septembre 2000 et février 2002 nous avons implanté 120 arthroplasties totales du genou. Chez 60 malades nous avons utilisé la technique standard et chez 60 malades nous avons utilisé le système de navigation OrthoPilot. Après l'opération tous les malades avaient une grande radiographie du membre inférieur, de la hanche à la cheville. Nous avons considéré que la valeur idéale de l'angle tibiofémoral latéral (LTFA) était de 174°. Dans le groupe standard la valeur moyenne de LTFA était 174.9°, dans le groupe navigation de 174.3°. Une déviation entre 0° et 2° de la valeur idéale a été notée dans 42 cas dans le groupe standard et dans 53 cas dans le groupe navigation. Dans le groupe standard 18 cas avaient une déviation de plus que 2.1°, alors qu'il y avait seulement 7 cas dans le groupe navigation avec une déviation dépassant 2.1°. Il n'y avait pas de complications relatives à l'usage du système de navigation. Le système offre une possibilité de placer les composants fémoral et tibial précisément avec moins de déviation de l'axe qu'avec la technique conventionnelle.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Proper component alignment is an essential step in the performance of a total knee replacement. Today it is possible to provide an accurate reproduction of anatomic axes and angles of the affected limb with the use of a navigation system. There are three different types of orthopaedic navigation systems. The purpose of this prospective study is to compare the roentgenographic results in patients who had a total knee arthroplasty (TKA) using the OrthoPilot kinematic CT-free navigation system with those of a matched group of patients who had the same type TKA implanted using the conventional procedure.
Material and methods
We studied 120 patients with a total of 120 TKAs implanted between September 2000 and February 2002. The patients were selected at random as they came for their first evaluation. The indications were primary osteoarthritis in 78 cases and secondary osteoarthritis in 42 cases. Details are given in Table 1.
In 60 cases the prosthesis was implanted using the conventional procedure (group 1), while in another 60 cases it was implanted using the OrthoPilot navigation system (group 2). All operations were performed by two experienced surgeons (RH and MJ). The surgical technique was the same in both groups. The patients were followed for an average of 15 (6–24) months.
In the patients in group 1 the femoral component was implanted after bone resection performed with the use of an intramedullary-placed femoral rod. The tibial component was inserted after proximal tibia resection with the use of an extramedullary alignment rod.
The OrthoPilot kinematic navigation system was used for patients in group 2. This is a CT-free system based on infrared data transmission between rigid bodies and camera. It needs no special pre-operative planning. The centres of the hip, knee and ankle joints were estimated kinematically. The tibial resection was then made by means of the special tibial cutting block with attached mobile rigid body and controlled by the navigation system. The special femoral cutting block with attached mobile rigid body was used for the distal femoral resection. The block gave the required valgus-varus position and anteversion-retroversion at the same time and was put into a correct position by means of computer navigation. The navigated implantation of a prosthesis lasted 10–15 min longer than the conventional procedure.
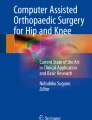
Radiographs used for evaluation were long and encompassed the entire lower extremity from the hip joint to the ankle. They were taken with the patient standing, trying to take weight equally on both feet, with the knee in maximal extension and facing the X-ray tube at a distance of 180 cm. For anteroposterior exposure the patient's patellae pointed strictly forward to guard against rotational error. A 100 mA, 0.05 s. exposure was used at 100–115 kV, depending on leg thickness; 105×35.5 cm films were used. Interobserver variability was insignificant. Angles were measured to the nearest whole degree using the same goniometer throughout the study. Measured angles are shown in Fig. 1.

Diagrams showing the measured angles. A anatomic lateral distal femoral angle (LDFA) is formed by intersecting the femoral anatomic axis with the tangent to the femoral condyles in the frontal plane. B anatomic lateral tibiofemoral angle (LTFA) is formed by intersecting the femoral anatomic axis with the tibial anatomic axis in the frontal plane. C anatomic medial proximal tibial angle (MPTA) is formed by intersecting the tibial anatomic axis with the tangent to the tibial plateau in the frontal plane. D anatomic posterior distal femoral angle (PDFA) is formed by intersecting the femoral anatomic axis and Bloomensaat´s line (pre-operative) or the tangent to the distal femoral cut (post-operative) in the sagittal plane. E anatomic posterior proximal tibial angle (PPTA) is formed by intersecting the tibial anatomic axis and the tangent to the tibial plateau in the sagittal plane
Results were classified according to the deviation of the anatomic lateral tibiofemoral angle (LTFA) from the "ideal" value of 174° into four groups: no deviation, deviation between 0.1° and 2.0°, deviation between 2.1° and 4.0° and deviation above 4.1°.
The Mann-Whitney U test was used for average comparison and the Bartlett test for standard deviation comparison.
Results
On the pre-operative radiographs there was no statistically significant difference of the measured angles between the groups. In group 2 we measured a mean anatomic LTFA=184.2° (160–195°) while the computer, with use of the kinematic examination, showed a mean LTFA=184.8° (162.4–194.1°). Post-operatively the mean LTFA for patients in group 2 using the computer was 174.7° (170.6–179°).
The post-operative measured values are given in Table 2. Post-operatively the Mann-Whitney U test revealed the only statistically significant difference between the groups, which was in the anatomic posterior proximal tibial angle (PPTA) (slope of the tibial component) (p<0,001). Statistical analysis using the Bartlett test found a significant difference in the deviation of LTFA from the ideal value (174°) between the two groups (p<0,02) (Table 3).
Discussion
Today it is possible to provide a more accurate reproduction of anatomical axes and angles of the affected limb with use of a navigation system or robot [4]. The advantage of these new systems seems to be useful, especially in complicated conditions [7, 16, 18, 21]. Radiographic assessment of the knee alignment after TKA has been presented in many studies [11]. Patel [12] compared axial alignment on short and long radiographs and concluded that short radiographs are adequate only for routine assessment in a busy out-patient clinic. Limb rotation and knee flexion have a significant effect on the measured anatomical axis [8]. Prakash et al. [14] described new computer software for measurement of limb alignment on scanned radiographs.
Lotke [9] and Townley [19] studied the influence of prosthesis positioning in total knee replacement and found a positive correlation between a good clinical result and a well-positioned prosthesis. Jeffery [5] concluded that accurate coronal alignment after total knee replacement is an important factor in the prevention of loosening. By correlation of laboratory and clinical observations, Bargren [1] found that the incorrect inserted tibial component fails under lower loads than the properly aligned component. Waugh [20] found a significant failure rate in cases with extreme varus or valgus alignments. The failure risk was lowest for knee replacements with an alignment between 2° of varus and 12° of valgus.
There are several radiographic studies on post-operative alignment of total knee replacements. Elloy [3] studied the accuracy of a system using intramedullary alignment: The mean error was 0.67° of valgus deviation from the mechanical axis; the maximum error was 6.68° valgus and 4.62° varus. Ritter [15] assessed the anatomic alignment: Kaplan-Meier survival curves showed significantly worse results in the varus group. Petersen and Engh [13] evaluated short and long radiographs: The mean tibiofemoral angle measured on the short films was 5.8° (range 4° varus to 13° valgus) and on the long films 7.2° (range 3° varus to 16° valgus).
Computer-assisted TKA has been mentioned only rarely [2]. We found only one study comparing radiographic assessment of alignment of the same components implanted with the use of a navigation system and in a standard manner [6]. The authors implanted 40 TKAs with use of the OrthoPilot navigation system and 40 using a classical technique. Better results were seen for the coronal and sagittal orientation of both tibial and femoral components in the navigated group. Mielke compared the results of different types of implants [10].
In contrast to Jenny and Boeri [6], we found a statistically significant difference between the groups in the post-operative value of the anatomic PPTA only. The more precise tibial component positioning in the sagittal plane (slope) was achieved with the use of the navigation system. A difference of less than 2° of the anatomic LTFA from the ideal value of 174° was achieved in nearly 90% of cases in group 2, whereas the navigation system was used in "only" 70% of cases in group 1.
Kinematic navigation affords a possibility to place both femoral and tibial components very precisely without risk of any greater axis deviation from the ideal value. This is especially important for the inexperienced orthopaedic surgeon. The OrthoPilot navigation system is safe. There were no complications related to its use in our study, and post-operative pain and knee function was not affected by the use of this computer-based alignment system.
Stulberg [17] performed 35 TKAs with use of a manual femoral and tibial intramedullary alignment system. In contrast to our study, there were substantial discrepancies between the alignment determinations obtained with use of the conventional radiographic measurements and those obtained with use of the intraoperative computer-assisted measurements. The average discrepancy between the radiographic and OrthoPilot pre-operative measurements of the tibiofemoral angle was 3.5° in Stulberg´s study and 0.6° in our study. The average discrepancy between the radiographic and OrthoPilot post-operative measurements was 2.1° in Stulberg´s study and 0.4° in our study.
References:
Bargren JH, Blaha JD, Freeman MAR (1983) Alignment in total knee arthroplasty. Clin Orthop 173:178–183
Delp SL, Stulberg SD, Davies B, Picard F, Leitner F (1998) Computer assisted knee replacement. Clin Orthop 354:49–56
Elloy MA, Manning MP, Johnson R (1992) Accuracy of intramedullary alignment in total knee replacement. J Biomed 14:363–370
Gossé F, Brack C, Gotte H, Roth M, Ruhmann O, Schweikard A, Vahldiek M (1997) Roboterunterstützung in der Knieendoprothetik. Orthopäde 26:258–266
Jeffery RS, Morris RW, Denham RA (1991) Coronal alignment after total knee replacement. J Bone Joint Surg [Br] 73:709–714
Jenny JY, Boeri C (2001) Navigiert implantierte Knietotalendoprothesen—eine Vergleichsstudie zum konvetionellen Instrumentarium. Z Orthop 139:117–119
Katz MM, Hungerford DS, Krakow KA, Lennox DW (1987) Results of total knee arthroplasty after failed proximal tibial osteotomy for osteoarthritis. J Bone Joint Surg [Am] 69:225–233
Lonner JH, Laird MT, Stuchin SA (1996) Effect of rotation and knee flexion on radiographic alignment in total knee arthroplasties. Clin Orthop 331:102–106
Lotke PA, Ecker ML (1977) Influence of positioning of prosthesis in total knee replacement. J Bone Joint Surg [Am] 59:77–79
Mielke RK, Clemens U, Jens JH, Kershally S (2001) Navigation in der Knieendoprothetik—vorläufige klinische Erfahrungen und prospektiv vergleichende Studie gegenüber konventioneller Implantationstechnik. Z Orthop 139:100–116
Oswald MH, Jakob RP, Schneider E, Hoogewood HM (1993) Radiological analysis of normal axial alignment of femur and tibia in view of total knee arthroplasty. J Arthroplasty 8:419–426
Patel DV, Ferris BD, Aichroth PM (1991) Radiological study of alignment after total knee replacement. Int Ortop 15:209–210
Petersen TL, Engh GA (1988) Radiographic assessment of knee alignment after total knee arthroplasty. J Arthroplasty 1:67–72
Prakash U, Wigderowitz CA, McGurty DW, Rowley DI (2001) Computerised measurement of tibiofemoral alignment. J Bone Joint Surg [Br] 83:819–824
Ritter MA, Faris PM, Keating EM, Meding JB (1994) Postoperative alignment of total knee replacement. Its effect on survival. Clin Orthop 299:153–156
Saleh KJ, Sherman P, Katkin P, Windsor R et al (2001) Total knee arthroplasty after open reduction and internal fixation of fractures of the tibial plateau. J Bone Joint Surg [Am] 83:1144–1148
Stulberg SD, Loan P, Sarin V (2002) Computer-assisted navigation in total knee replacement: results of an initial experience in thirty-five patients. J Bone Joint Surg [Am] 84:90–98
Toksvig-Larsen S et al (1998) Fixation of the tibial component of total knee arthroplasty after high tibial osteotomy. J Bone Joint Surg [Br] 80:295–297
Townley ChO (1985) The anatomic total knee resurfacing arthroplasty. Clin Orthop 192:82–96
Waugh MTW (1985) Tibiofemoral alignment and the results of knee replacement. J Bone Joint Surg [Br] 67:551–556
Windsor RE, Insall JN, Vince KG (1988) Technical considerations of total knee arthroplasty after proximal tibial osteotomy. J Bone Joint Surg [Am] 70:547–555
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hart, R., Janeček, M., Chaker, A. et al. Total knee arthroplasty implanted with and without kinematic navigation. International Orthopaedics (SICOT) 27, 366–369 (2003). https://doi.org/10.1007/s00264-003-0501-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-003-0501-6